Abstract
Background. Bioceramic sealers have gained popularity due to their distinctive bioactivity and superior sealing ability in comparison with other contemporary sealers. Therefore, it is important to understand their interactions with agents used in root canal therapy, such as intracanal medicaments (ICMs), and the impact of these interactions on the bonding ability of the sealer to radicular dentin.
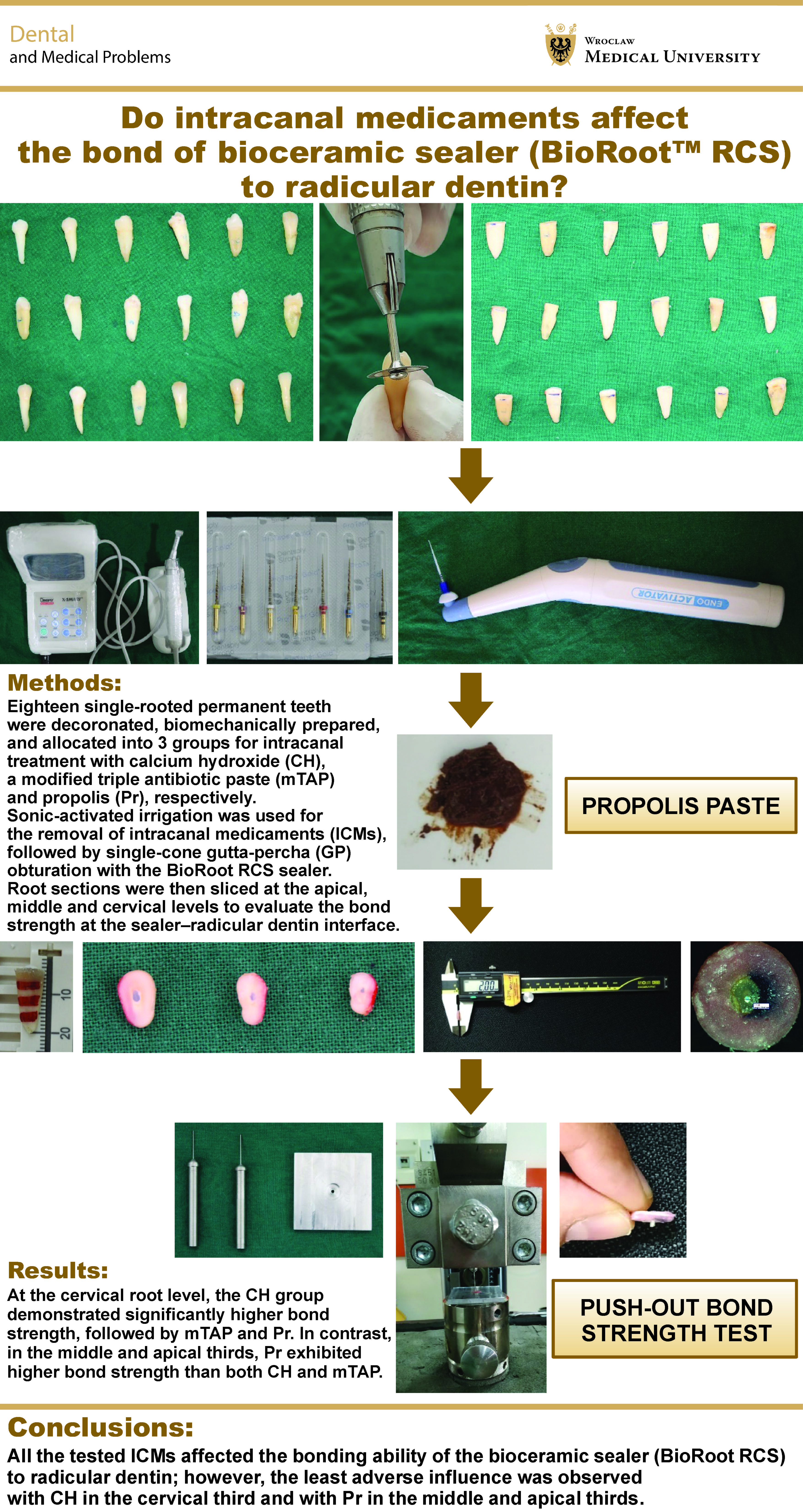
Objectives. The present in vitro study assessed the influence of 3 ICMs – calcium hydroxide (CH), a modified triple antibiotic paste (mTAP) and propolis (Pr)-based agents – on the bonding ability of bioceramic sealer (BioRoot™ RCS) to radicular dentin.
Material and methods. Eighteen single-rooted permanent teeth were decoronated, biomechanically prepared, and allocated into 3 groups for intracanal treatment with CH, mTAP and Pr, respectively. Sonic-activated irrigation was used for the removal of ICMs, followed by single-cone gutta-percha (GP) obturation with the BioRoot RCS sealer. Root sections were then sliced at the apical, middle and cervical levels to evaluate the bond strength at the sealer–radicular dentin interface.
Results. At the cervical root level, the CH group demonstrated significantly higher bond strength, followed by mTAP and Pr. In contrast, in the middle and apical thirds, Pr exhibited higher bond strength than both CH and mTAP.
Conclusions. All the tested ICMs affected the bonding ability of the bioceramic sealer (BioRoot RCS) to radicular dentin; however, the least adverse influence was observed with CH in the cervical third and with Pr in the middle and apical thirds.
Keywords: calcium hydroxide, propolis, bioactive, sealer, bond strength
Introduction
Successful endodontic therapy primarily depends on adequate chemo-mechanical debridement and disinfection, followed by three-dimensional (3D) obturation to achieve a corono-apical seal. Traditionally, root canal sealers have been used in combination with semisolid/solid core materials to obtain a 3D filling with a hermetic apical seal, ensuring their infiltration into lateral and accessory canals, and thereby reducing apical and coronal microleakage.1
Apart from the fundamental material requisites of biocompatibility, dimensional stability and antimicrobial properties, the primary requirement of an ideal root canal sealer is the formation of an adequate adhesive bond at the radicular wall–sealer/filling material interface to ensure a superior sealing ability. Several endodontic sealers with variable sealing abilities, based on different formulations, such as zinc oxide–eugenol, glass ionomer, salicylate (calcium hydroxide-based), silicone, epoxy resin, methacrylate, and more recently bioceramic sealers (calcium silicate–based, calcium phosphate-based and mineral trioxide aggregate (MTA)-based), have been introduced into endodontics.1
In a systematic review conducted by Alghamdi and Abduljawad, a total of 12 in vitro studies evaluating the apical sealing potential of various root canal obturation methods with different endodontic sealers, using the non-destructive fluid filtration technique, were assessed.2 In this review, when the apical sealing ability of a resin-based sealer (AH Plus) was compared with 2 different bioceramic sealers (iRoot SP and MTA Fillapex), one study by Zhang et al. reported no significant difference in apical sealing when iRoot SP was used with either cold lateral compaction or the single-cone gutta-percha (GP) technique.3 In contrast, Asawaworarit et al., who evaluated MTA Fillapex using warm vertical compaction, reported relatively lower apical microleakage after 4 weeks of evaluation.4
A scanning electron microscopy (SEM) analysis by Haji et al. evaluated the adhesion ability of 2 calcium silicate-based bioceramic sealers (BioRoot RCS and CeraSeal RCS) in comparison with a zinc oxide–eugenol-based sealer at the sealer–radicular dentin interface in the coronal, middle and apical thirds, based on the sealing ability scores (Ray and Seltzer, 1991), which categorized adhesion as very good (no gaps), good (minor gaps) or acceptable (frequently observed gaps).5 Both bioceramic sealers demonstrated “very good adhesion” in all thirds of the root as compared to the “acceptable adhesion” observed with the zinc oxide–eugenol sealer, thereby highlighting the superior physical properties of bioceramic sealers, such as wettability, dimensional stability, flow, and low film thickness, which promote greater surface penetrability.5
Another recent systematic review and meta-analysis by Rekha et al. assessed 24 in vitro studies for qualitative analysis, with sample sizes ranging from 10 to 26, of which 16 studies were included in the quantitative analysis.6 For the evaluation of microleakage, a review of 18 studies employing different advanced methods for assessing the sealing ability concluded that, although both epoxy resin-based and bioceramic sealers exhibited comparable adhesive properties, bioceramic sealers – owing to their desirable combination of a superior sealing ability and biocompatibility – may offer improved long-term success and better prognostic outcomes for the tooth.6
Among the various endodontic sealers available, calcium silicate-based sealers have garnered widespread interest and gained immense popularity in recent times owing to their superior sealing ability at the radicular interfacial dentin. This phenomenon is attributed to the precipitation of hydroxyapatite and the enhanced ion diffusion resulting from the degradation of the collagenous component, caused by the alkalinity of the sealer’s hydration products. Owing to their hydrophilic nature, these sealers utilize the natural moisture content within the dentinal tubules to complete the setting reaction, thereby establishing an intricate sealing bond with the radicular dentin and preventing apical leakage, which greatly contributes to the success of non-surgical endodontic therapy.1
For effective apical sealing, the confinement of the sealer within the canal space is crucial to prevent apical extrusion. This commonly encountered procedural mishap violates the biological objectives of obturation, as the unset sealer may act as a foreign body capable of inducing cytotoxic reactions and post-operative pain.
In a review evaluating the prevalence of sealer extrusion, a total of 439 completed non-surgical endodontic treatment procedures in permanent teeth, including both primary treatment and retreatment, were assessed.7 The review included reports published in 62 issues of the Journal of Endodontics (2015–2020) and 9 issues of the International Endodontic Journal (2020). Based on the criterion of any radiopaque material extending beyond the radiographic apex of the root, sealer extrusion was observed in 142 cases, accounting for 32.3% of the total cases.7
A systematic review conducted by Aminoshariae and Kulild reported that cases with sealer extrusion exhibited a 32% greater risk of unfavorable, non-healing outcomes as compared to cases without sealer extrusion.8 A prospective clinical trial conducted by Yu et al. reported a relatively higher incidence of sealer extrusion with the epoxy resin-based sealer AH Plus (41.5%) and the employment of the warm vertical obturation technique, compared to only 13.7% when the calcium silicate-based bioceramic sealer EndoSequence BC Sealer was used with the single-cone GP technique.9 Similarly, a study conducted by Tan et al. demonstrated that the calcium silicate-based bioceramic sealer TotalFill BC exhibited a lower rate of apical sealer extrusion as compared to the epoxy resin-based sealer AH Plus.10
In a study conducted by Chybowski et al., although a high incidence of apical sealer extrusion (47.4%) was documented following single-cone obturation with the calcium silicate-based bioceramic sealer EndoSequence BC Sealer, this finding was attributed to the excellent flowability of bioceramic sealers.11 Nevertheless, no significant adverse effects were observed, even after a follow-up period of 2.5 years. The authors suggested that, owing to the low solubility of calcium silicate components, the extruded sealer may persist within the periradicular tissues and potentially undergo bioactive interaction with tissue fluids, leading to hydroxyapatite formation within the host tissue and eventual replacement by bone.8, 11 Paradoxically, contrary to expectations, several researchers have demonstrated that even the extrusion of conventional endodontic sealers may not affect the overall outcomes of non-surgical endodontic treatment to a great extent. Goldberg et al. reported no statistically significant effect on treatment outcomes in the case of obturation with the lateral condensation technique, using epoxy resin- and zinc oxide-based sealers, with a mean follow-up period of 4.86 years.12 Similarly, Ricucci et al. concluded that the apically extruded root canal sealers did not produce statistically significant differences in treatment outcomes, even when the extruded material was radiographically evident.13 The authors further suggested that the presence of a pre-operative periradicular lesion was more likely to be the primary determinant of unsuccessful outcomes.13
The apical extrusion of the sealer and/or obturation materials is also associated with post-operative pain, one of the most common undesirable sequelae resulting from a transient inflammatory response triggered by the sensitization of the periradicular tissues. In this regard, calcium hydroxide-based sealers, such as Sealapex and Apexit Plus, are reported to be better tolerated than epoxy resin-based sealers, such as AH Plus and Resino Seal, which have been shown to release cytotoxic amines, epoxy resin components, and trace amounts of formaldehyde (3.9 ppm).14
A clinical study compared 2 calcium silicate-based bioceramic sealers – Bio-C Sealer and BC Sealer – with the epoxy resin-based sealer AH Plus in molar teeth diagnosed with asymptomatic irreversible pulpitis and obturated using the vertical compaction technique.15 A relatively similar extrusion rate (1–2 mm, approx. 12%) was observed among all groups. Using a visual descriptor scale ranging from 0 to 10, the 330 patients reported no significant differences in post-obturation pain among the groups at 6, 12 and 48 h, as well as at 7 days postoperatively. The study concluded that the gradual reduction in pain symptoms over time might be attributed to the progressive decline in inflammatory activity within the tissues, along with the transition of the irritating components of the sealer into an inert state, following complete setting.15
Bonding of the sealer to radicular dentin is governed by the degree of adhesion, which in turn largely depends on 2 principal parameters – the intrinsic properties of the sealer material and the surface characteristics of intracanal dentin, following debridement and disinfection during chemo-mechanical instrumentation. The properties of root canal sealers that influence adhesion include surface tension, wettability, hydrophilicity, and the setting behavior (expansion or contraction) of the material when used in conjunction with obturating core materials. On the other hand, the dentinal wall factors affecting adhesion are not only related to dentin topography and intermolecular surface energy, but also to the degree of surface cleanliness with respect to the smear layer generated during instrumentation, residual traces of irrigants and intracanal medicaments (ICMs) used for disinfection, and the surface modifications induced by laser-assisted photo-activated disinfection (PAD).16
The hydrophobic behavior is primarily attributed to the resin component of epoxy resin-based sealers such as AH Plus, which also tend to undergo polymerization shrinkage during setting. Both factors contribute to reduced adaptation and potential detachment from the radicular dentin walls. In contrast, hydrophilic non-resin sealers based on zinc oxide–eugenol, calcium hydroxide, calcium silicate, and their combinations – such as GuttaFlow Bioseal –exhibit superior flowability, as well as a slight expansion upon setting.17 A study by Uzunoglu-Özyürek demonstrated greater dentinal tubule penetration with the calcium silicate–based bioceramic sealer BioRoot RCS as compared to the epoxy resin-based sealer AH Plus.18
Bioceramic sealers are composed of fine fillers that enhance their flowability, while their hydrophilic nature enables the utilization of the inherent moisture within the dentinal tubules. They also exhibit slight expansion during setting without polymerization shrinkage, thereby contributing to the formation of a relatively gap-free interface between the dentinal wall, the root canal sealer and the GP filling material.19
Routinely used intracanal irrigants, such as sodium hypochlorite (NaOCl), ethylenediaminetetraacetic acid (EDTA) and chlorhexidine (CHX), among others, alter the surface energy of dentin. Similarly, ICMs, such as calcium hydroxide and a triple antibiotic paste (TAP), when applied for extended periods, may leave residual deposits on the canal walls. These remnants can interfere with the wettability, flow and adaptation of sealers, thereby compromising the adhesion even of hydrophilic root canal sealers.20
Intracanal medicaments are stable, biocompatible temporary therapeutic and antimicrobial agents that provide enhanced canal disinfection through prolonged contact during the inter-appointment period in multi-visit non-surgical endodontic therapy. Following the use of various intracanal irrigants, these medicaments are employed to address multifactorial and challenging clinical scenarios, including long-standing large periapical pathologies, weeping canals, traumatic dental injuries, complex root canal anatomy, and patients with compromised immune responses.21, 22, 23, 24
Several ICMs with diverse therapeutic properties and formulations, like calcium hydroxide, antibiotic-based pastes, CHX, and various natural alternatives, have been introduced into endodontic practice.
Calcium hydroxide is one of the oldest materials (Hermann, 1920) used as ICM in endodontics and is regarded as the gold standard, as it fulfils the majority of the requirements proposed by Grossman,25 with a reported success rate of 73.8–80.8%.26 When calcium hydroxide comes into contact with aqueous fluid, it slowly dissociates into calcium and hydroxyl ions, creating an alkaline root canal environment with highly reactive free radicals that exert a potent antimicrobial effect against most common endodontic microorganisms.26 However, several studies have also reported its limited inhibitory effect against highly resistant microorganisms, such as Enterococcus faecalis, a Gram-positive facultative anaerobic bacterium known for its ability to form biofilms and its association with post-endodontic periradicular lesions, which account for 22–77% of endodontic failures.27, 28, 29 Long-term application of calcium hydroxide has also been shown to exert a structural weakening effect on radicular dentin,30 with a progressive decrease in microhardness – an indicator of mineral gain or loss – which may negatively affect the sealing ability. In comparison, propolis demonstrated a progressive increase in microhardness over a period of 7 days.31
For the utilization of relatively newer calcium silicate-based bioceramic sealers in both single- and multiple-visit endodontics, it is essential to evaluate their performance following the use of routinely employed ICMs, including calcium hydroxide-based preparations, antibiotic pastes and the emerging natural agents. However, given the limitations associated with calcium hydroxide-based ICMs, there is a need to compare alternative medicaments, such as antibiotic paste-based formulations with broad-spectrum antimicrobial activity and natural agents with improved biocompatibility, better tissue and tolerance fewer adverse effects. Accordingly, the present study aimed to evaluate the influence of various ICMs – calcium hydroxide (CH), a modified triple antibiotic paste (mTAP) and propolis (Pr) – on the push-out bond strength (POBS) of a calcium silicate-based bioceramic sealer BioRoot™ RCS to radicular dentin.
Material and methods
Eighteen extracted single-rooted human permanent teeth were selected after excluding specimens with surface defects or crack lines, developmental anomalies, calcified roots, internal or external resorption, open apices, severe root curvatures, or previous endodontic treatment.
Sample preparation
Decoronated root specimens were subjected to biomechanical preparation using ProTaper Gold files (Dentsply Maillefer, Ballaigues, Switzerland) up to F4 (size 40, 6% taper), with irrigation using 3% NaOCl and 17% EDTA solution. Following the final irrigation with distilled water, the root canal samples were blot dried using paper point cones and randomly allocated into 3 groups of 6 samples each to receive intracanal dressings delivered with a Lentulo spiral, as follows: group 1 (G1) – CH (calcium hydroxide and distilled water)23; group 2 (G2) – mTAP (a modified triple antibiotic paste prepared by combining approximately equal amounts of ciprofloxacin, metronidazole and cefaclor powders with distilled water in a 3:1 proportion)32; and group 3 (G3) – Pr (200 mg propolis powder (Hi-Tech Natural Products (India) Ltd., Delhi, India) mixed with 0.3 mL saline).33
The access cavities were sealed with a zinc oxide–eugenol-based filling material and stored at 37°C under 100% relative humidity for 2 weeks. The intracanal dressing was removed by sequential irrigation with 5 mL each of 3% NaOCl and 17% EDTA, followed by the final irrigation with distilled water activated by sonic agitation using the EndoActivator® system (Dentsply Tulsa Dental Specialties, Tulsa, USA) for 30 s (18,000 cycles per minute). The root canals were obturated with a single GP cone, size F4, coated with the BioRoot RCS endodontic sealer (Septodont, Saint-Maur-des-Fossés, France), restored coronally with a zinc oxide–eugenol-based material and allowed to set for 1 week.
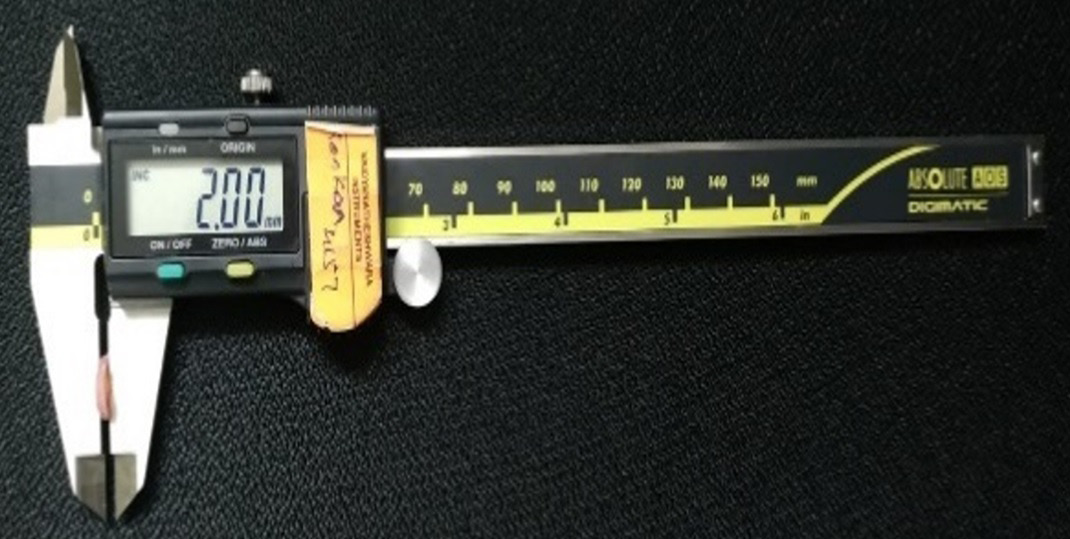
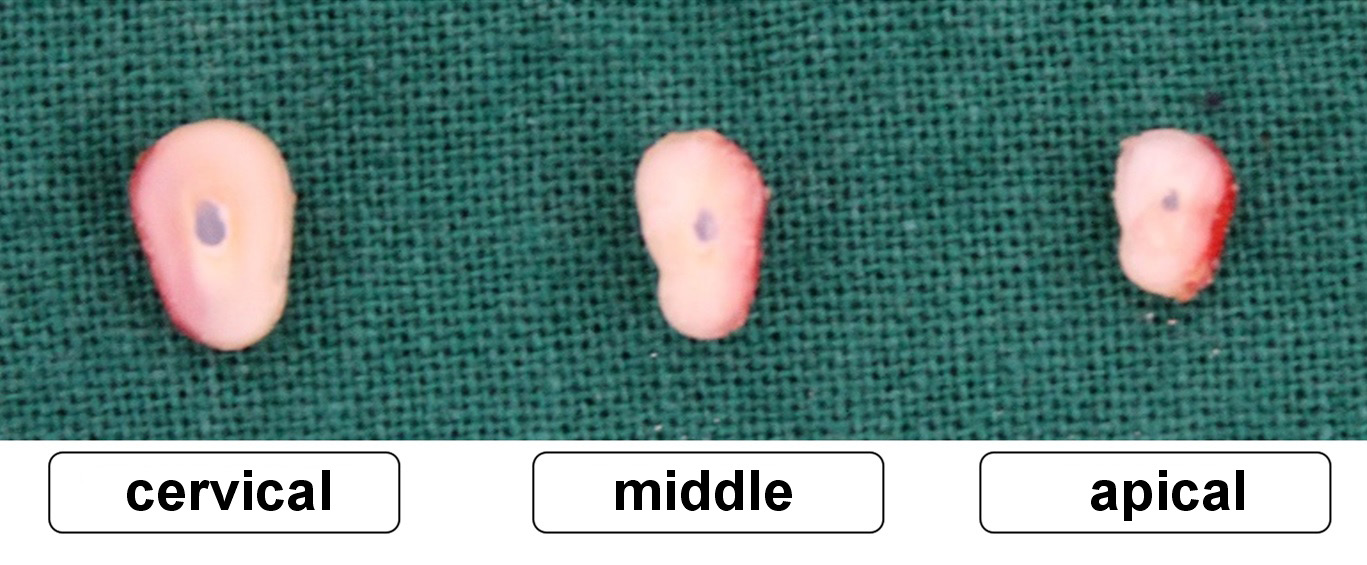
The roots were horizontally sectioned into slices approx. 2 mm thick, as verified using a digital caliper (Figure 1), with a diamond disc to obtain apical, middle and cervical sections at 3, 7 and 11 mm levels, respectively (Figure 2).
Push-out bond strength (POBS) assessment
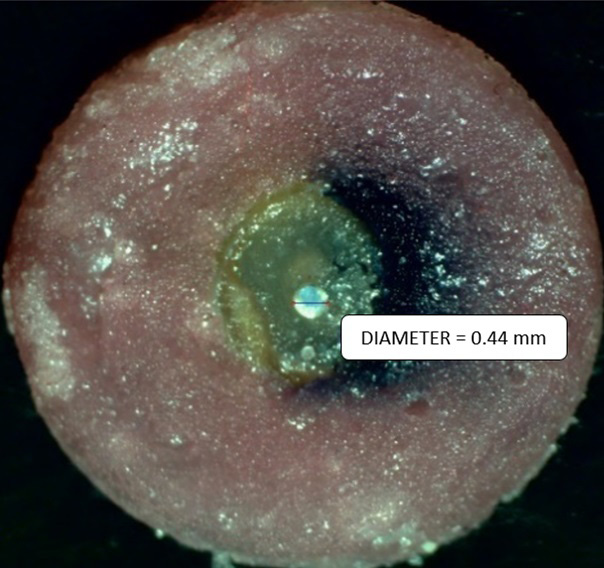
Root specimens mounted on a custom-made acrylic mold with a central opening to facilitate the push-out of the obturation material were subjected to compressive loading in a corono-apical direction, using a universal testing machine. Pluggers of varying tip diameters (0.3–0.8 mm) were used at a crosshead speed of 2 mm/min; they were positioned to cover most of the surface of the root-filling material without contacting the adjacent canal walls.
Failure/debonding was identified by a steep drop on the load–time graph generated by the computer software and/or by the complete dislodgement of the root-filling material. The maximum failure load was recorded in newtons and subsequently converted to megapascals. The recorded peak load was divided by the bonded surface area, estimated using a stereomicroscope (Figure 3), to calculate bond strength using the following formula (Equation 1)34, 35:
where:
F – maximum force [MPa];
A – bonded surface area [mm2];
A = πh × (r1 + r2);
h – specimen thickness [mm];
r1 – apical aspect radius;
r2 – coronal aspect radius.
Statistical analysis
Statistical analysis was performed using the two-way analysis of variance (ANOVA), followed by Tukey’s post hoc test, using the nMaster Software, v. 2 (https://nmaster.software.informer.com), and the results were considered statistically significant at p < 0.05.
Results
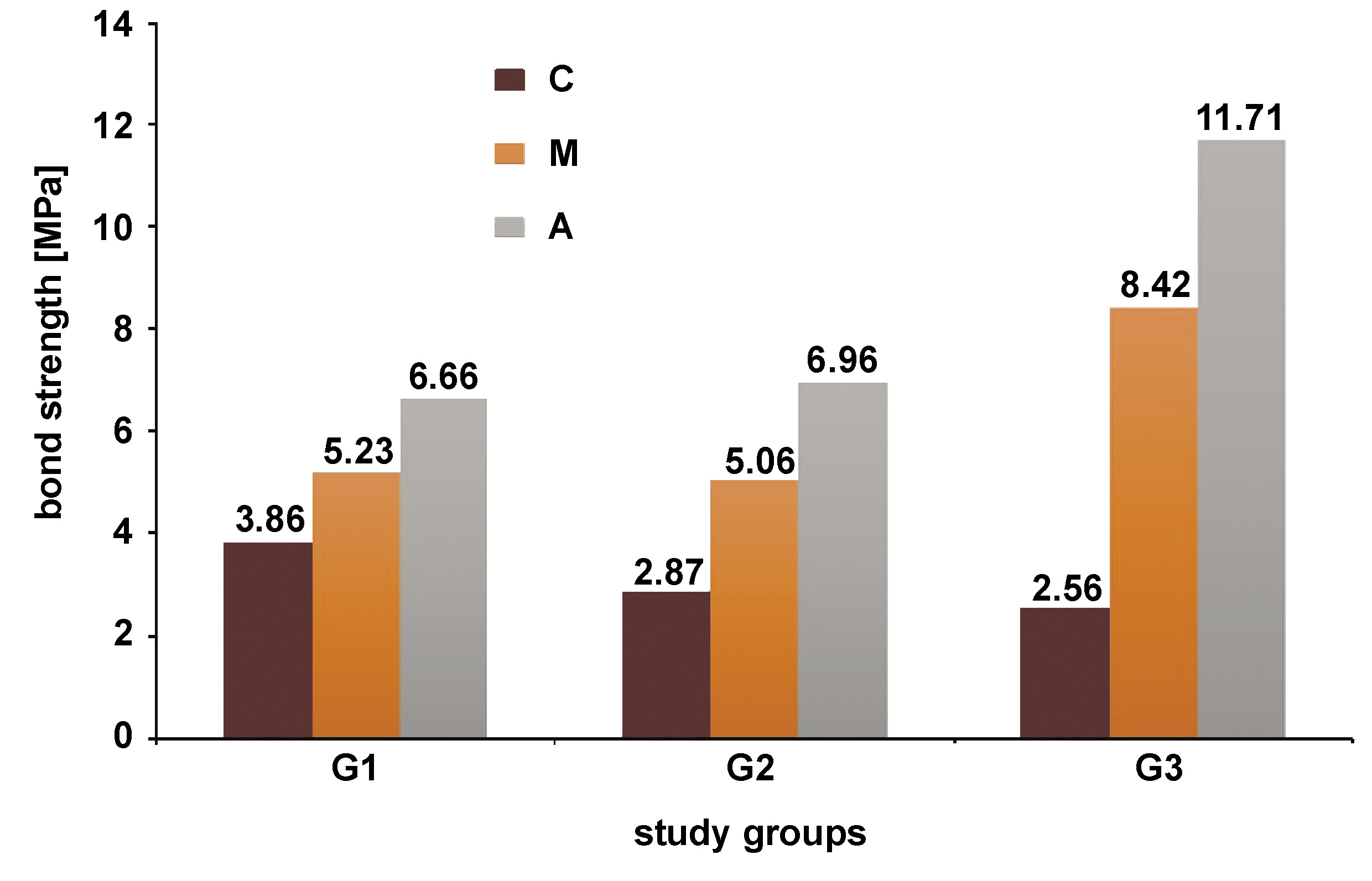
BioRoot RCS demonstrated higher POBS in the middle and apical sections when used following propolis, whereas calcium hydroxide showed better results in the cervical third (Table 1, Figure 4). While the difference in the POBS values between G2 (mTAP) and G3 (Pr) was non-significant at the cervical level, G1 (CH) and G2 (mTAP) demonstrated non-significant differences at the middle and apical levels (p > 0.05) (Table 2).
Discussion
Obturation constitutes the final step in the triad of non-surgical endodontic treatment, following adequate access opening and biomechanical preparation of the root canal space. Traditionally, root canal obturation is most commonly accomplished using GP-based filling materials, considered the gold standard owing to their inert, thermoplastic, retreatable, and radiopaque nature, along with their wide availability. However, these materials unfortunately lack the ability to adhere to the radicular dentin walls.
Ideally, a root filling material should intimately bond to intracanal dentin and resist the dislodging forces by achieving strong adhesion. This objective is accomplished through the use of endodontic sealers at the interface, along with GP. Sealers, applied in a thin, tacky consistency, act as a luting medium for the core filling material during obturation, filling voids and entombing residual bacteria, thereby creating a fluid-tight seal. Over the years, several advancements have been made to improve the type, quality and properties of endodontic sealer materials, with the aim of establishing a continuum “the core material–the sealer–radicular dentin” as a single cohesive entity.36
Bioceramic materials are ceramic-based materials used in both medicine and dentistry. The newer bioceramic materials introduced into dentistry primarily consist of bioactive glass, calcium phosphate, calcium silicate, hydroxyapatite, bioinert alumina, zirconia, and other components. In dentistry, they have been applied for various purposes, including as dentin substitutes, pulp-capping agents, pulpotomy materials, apexification agents, root repair materials, retrograde filling materials, perforation sealing agents, endodontic sealers, for filling bony defects, and as adjuncts in regeneration during periradicular surgeries. These materials offer several advantages, including excellent biocompatibility, superior mechanical properties that provide a strengthening effect to the tooth structure, antimicrobial activity, intrinsic osteoinductive potential, a superior sealing ability, chemical bonding to the tooth structure, and radiopacity.37, 38
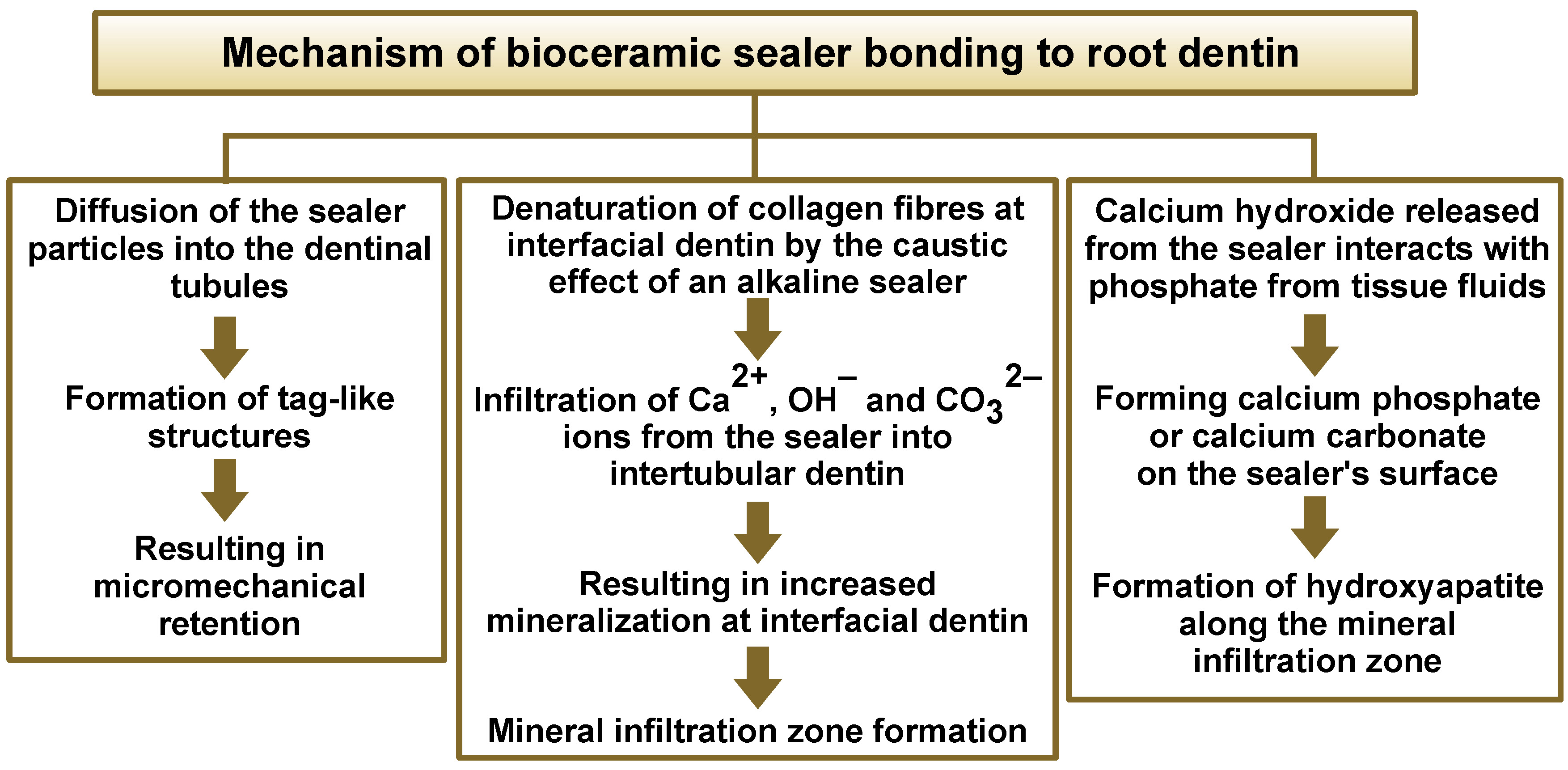
Bioceramic sealers have been used in endodontics for the past 30 years, and are classified based on their composition into MTA-based, calcium phosphate-based and calcium silicate-based sealers. These sealers possess 2 key properties that distinguish them from other sealers – bioactivity and a superior sealing ability to radicular dentin through the formation of a distinct mineral infiltration zone (Figure 5).3, 39, 40, 41
BioRoot RCS, an alkaline calcium silicate-based bioceramic sealer with a pH of approx. 11–12, is a relatively new material comprising components such as tricalcium silicate and calcium chloride (Table 3). BioRoot RCS was used in the present study, as it has been reported to release nearly twice the amount of calcium ions and form a greater calcium phosphate phase as compared to EndoSequence BC Sealer.42, 43 In addition, it has been shown to stimulate human periodontal ligament cells to express angiogenic and osteogenic growth factors.44 BioRoot RCS has also been associated with lower cytotoxicity than conventional endodontic sealers, along with antimicrobial properties and the ability to promote hard tissue deposition.45, 46, 47 An SEM study comparing the sealing ability of Sealapex, BioRoot RCS, MTA Fillapex, and zinc oxide–eugenol-based sealers demonstrated that BioRoot RCS exhibited the best marginal adaptation, with the least number of gaps at the cervical, middle and apical root interfaces, which was attributed to its hydraulic sealing capability.48
As a variety of intracanal irrigants and medicaments based on chemical and natural formulations are routinely employed for root canal disinfection in contemporary endodontic practice, it is imperative to evaluate and understand their influence on the sealing ability of newer bioceramic sealers. Since ICMs remain in contact with radicular dentin for relatively prolonged durations, the present study was conducted to evaluate the influence of 3 different ICMs – calcium hydroxide (gold standard), a modified triple antibiotic paste (mTAP) and propolis (a natural bee-derived product) – on the sealing ability of the bioceramic sealer BioRoot RCS to radicular dentin at different root levels.
Calcium hydroxide, a commonly used ICM, possesses antimicrobial and anti-inflammatory properties, an alkaline pH of approx. 12.5, as well as the ability to dissolve tissue, inhibit root resorption and promote hard tissue formation with periradicular healing. However, owing to variable reports regarding its antimicrobial efficacy, alternative medicaments based on CHX, antibiotic paste combinations and natural agents such as propolis have been investigated as potential options.22, 49
Triple antibiotic paste is a biocompatible ICM composed of the bactericidal agents ciprofloxacin and metronidazole, along with the bacteriostatic agent minocycline. TAP is effective against Gram-negative, Gram-positive and anaerobic microbiota, and helps create a favorable environment for subsequent endodontic procedures. In a microbiological study, TAP demonstrated a larger zone of inhibition against E. faecalis as compared to calcium hydroxide, which is considered the gold standard among ICMs.50 However, minocycline in TAP has been associated with tooth discoloration, anti-angiogenic effects and the chelation of root dentin, leading to the demineralization and weakening of the root structure. Therefore, it has been replaced with alternatives such as cefaclor, a second-generation cephalosporin, to formulate mTAP, which was used in the present study. The mTAP formulation consisting of ciprofloxacin, metronidazole and cefaclor is effective in managing polymicrobial endodontic infections.51
Propolis is a well-established natural antibiotic agent derived from beeswax and consists of a complex blend of resinous substances collected by bees from plants. It contains flavonoids as its principal biologically active constituents, along with other organic compounds, such as aromatic and fatty acids, which contribute to its recognized antimicrobial efficacy as ICM against polymicrobial colonies isolated from necrotic root canals.52, 53 The chemical composition of propolis includes aromatic acids, fatty acids and their esters, flavonoids, such as naringenin, pinocembrin, phenols, and 5-methoxy-3,7-dihydroxyflavonone, as well as ketones, alcohols, terpenes, such as chrysophanol and 1-ethanone, and other trace components. In addition to its antimicrobial activity, propolis also exhibits antioxidant and anti-inflammatory properties. Besides its application as ICM, it has been used as an anticaries agent, a canal irrigant, a pulp-capping agent, a desensitizing agent, and as a transport medium for avulsed teeth.33
The present in vitro study evaluated the POBS of radicular dentin obturated with a calcium silicate-based sealer (BioRoot RCS), following treatment with a natural ICM (propolis), an antibiotic-based medicament (a modified triple antibiotic paste – mTAP) and a calcium hydroxide-based ICM in the cervical, middle and apical thirds of the root canal. In the cervical third, the highest bond strength was observed in G1 (CH), followed by G2 (mTAP) and G3 (Pr). In the middle third, the highest bond strength was recorded in G3 (Pr), followed by G1 (CH) and G2 (mTAP), whereas in the apical third, bond strength was highest in G3 (Pr), followed by G2 (mTAP) and G1 (CH), respectively. Statistically, no significant differences were observed between G2 and G3 in the cervical third, or between G1 and G2 in the middle and apical thirds (p > 0.05).
In the cervical third, G1 (CH) demonstrated higher POBS than G2 (mTAP) and G3 (Pr) (Table 1), which could be attributed to the interaction between the primary components of BioRoot RCS sealer, namely calcium silicate and calcium phosphate, and the residual calcium hydroxide.23 In the middle and apical thirds, G3 (Pr) exhibited the highest POBS, possibly facilitated by the preferentially strong interaction of the aromatic and fatty acids present in propolis with the hydrophilic components of the dentin surface22 and BioRoot RCS, which warrants further investigation to better understand this chemical interaction.
Group G2 (mTAP) demonstrated only moderate POBS at all root levels, which may be attributed to the reduced dislodgement resistance resulting from the significant erosion of the dentinal tubule orifices by the residual medicament. Similar findings were observed in an SEM study by Akman et al., which evaluated mTAP and double antibiotic paste (DAP) dressings used with BioAggregate apical plugs and Biodentine.36
The POBS recorded in all 3 groups was highest in the apical third, followed by the middle and cervical thirds, respectively. This finding is consistent with the observations of Mannocci et al., who reported an association between higher bond strength and lower densities of the dentinal tubules.54 In addition, Cimpean et al. suggested that the precise adaptation of the GP cone in the middle and apical sections of the prepared canals contributes to improved sealer diffusion into the dentinal tubules.55
While ICMs have been implicated in both negatively and positively influencing the dislodgement resistance of root-filling materials, some studies have also reported negligible effects. Nagas et al. demonstrated the detrimental impact of residual traces of ICMs on cement adhesion, with the exception of calcium hydroxide,56 whereas Topçuoğlu et al. reported that calcium hydroxide might positively enhance bonding strength by chelating with calcium in dentin.57 In the latter study, the residues of mTAP appeared to interfere with chemical bonding between radicular dentin and the sealer by acting as a physical barrier, whereas the removal of the sticky propolis-based ICM by the circulating irrigants was relatively limited in the apical and middle thirds as compared with the cervical third.22, 57
As the presence of residual medicaments plays a significant role in sealer adhesion, their effective removal must be considered during POBS evaluation. Although ultrasonic-activated irrigation has shown insufficiency in removing calcium hydroxide remnants from root canals,18 it has been found to be effective when used in combination with NaOCl for the removal of TAP from artificial grooves.58 Several researchers have reported EDTA as the most effective agent for eliminating calcium hydroxide from the canal space55; hence, a combination of NaOCl and EDTA with ultrasonic irrigation was employed as the final debridement and cleansing protocol in this study. The NaOCl–EDTA irrigation protocol prior to the use of a bioceramic sealer (TotalFill BC) has been shown to yield higher POBS values than etidronic acid and NaOCl alone, as EDTA roughens the dentin surface, thereby enhancing the micromechanical interlocking of the sealer with the dentinal tubules.59 However, the delivery and activation methods used in the irrigation protocol may also influence POBS outcomes.
A study by Bogari et al. evaluated the bonding ability and adaptation of a bioceramic sealer (TotalFill BC), using a POBS test and SEM following irrigation with 3 protocols – conventional syringe-needle irrigation, ultrasonic activation, and neodymium-doped yttrium aluminum garnet (Nd:YAG) laser activation at a wavelength of 975 nm in the pulsed mode.60 The highest POBS values were observed in the Nd:YAG laser group (6.46 ±0.5 MPa), which was statistically significant in comparison with the ultrasonic (4.21 ±2.2 MPa) and conventional syringe-needle irrigation (3.33 ±1.8 MPa) groups. The SEM analysis of the radicular wall–GP/sealer interface demonstrated the largest gaps in the conventional syringe-needle group (~61 µm), followed by the ultrasonic group (~58 µm), while the least gaps were observed in the Nd:YAG laser group (~25 µm), which also produced a smoother, cleaner dentin surface conducive to sealer penetration.60 These findings indicate that the irrigation protocols combined with different activation methods not only enhance canal debridement and smear layer removal, but also influence the bonding performance of bioceramic sealers to the canal walls. Similarly, a pilot study by Esteves-Oliveira et al. investigating the effects of lasers on the permeability and morphology of radicular dentin reported that the Nd:YAG laser significantly reduced dentin permeability as compared to the erbium-doped yttrium aluminum garnet (Er:YAG) and diode lasers.61 Hence, it can be concluded that although different lasers exhibit varying properties, they show promising potential as adjuncts for disinfection and debridement in endodontic treatment.60, 61, 62, 63, 64 Accordingly, the future scope of the present study includes evaluating different ICMs in combination with various irrigation activation methods, including laser-assisted protocols, to further assess their impact on the POBS of bioceramic sealers to radicular dentin.
The POBS assessment tests are widely employed to evaluate the effectiveness of bonding between dental materials and radicular dentin,24 as dislodgement resistance during restorative procedures, post-space preparation and tooth flexure not only helps prevent corono-apical leakage, but also enhances resistance to root fracture.65 A material exhibiting high POBS contributes to improved longevity and a better prognosis of endodontically treated teeth.24, 65
Two-millimeter-thick root sections were used for bond strength assessment in this study to minimize early debonding and sealer detachment during slicing. The plugger-to-specimen diameter ratio is an important parameter, as ratios below 55% may reduce bond strength values, whereas ratios between 70% and 90% do not significantly influence the results.66 Since the plugger diameter is required to be approx. 0.85 times smaller than the diameter of the obturation filling while still being broad enough to avoid scoring the material surface,67 pluggers of varying diameters (0.3–0.8 mm) were used in this study.
As obturation with lateral condensation has inherent disadvantages, including the lack of GP homogeneity, poor adaptation to the canal walls, a higher proportion of the sealer in the apical region, and an increased risk of vertical root fracture,68 and as warm vertical compaction is unsuitable for bioceramic sealers due to the potential heat-induced alteration of their adhesive properties, single-cone GP obturation was employed in this study.69 Although the use of a core material with a sealer as a root canal filling may present limitations, such as voids at the sealer–core interface and the lack of homogeneity, it remains the accepted standard in contemporary endodontics. Accordingly, a single GP cone (size F4) was used as the core material in combination with the calcium silicate–based sealer. In addition, previous studies have reported that endodontic sealers used in conjunction with a core material exhibit lower POBS as compared to the sealer-only obturation techniques,56 while other investigations have suggested that dislodgement resistance testing may yield inaccurate values due to the deformation of GP.70 Hence, further studies are warranted to evaluate the influence of prior application of ICMs on the POBS of calcium silicate-based materials to radicular dentin when bulk sealer obturation is used.
Limitations
As an intracanal medicament, propolis shows promising potential; however, further in vivo and long-term clinical studies are required to evaluate its sustained clinical performance. Another limitation of this in vitro study is the lack of assessment of residual medicament traces on the radicular dentin surface following the completion of the irrigation protocol. The presence of residual ICMs within the root canal should be considered when interpreting the final results.
Conclusions
Within the limitations of this in vitro study, all tested ICMs affected the bonding ability of the calcium silicate-based bioceramic sealer (BioRoot RCS) to radicular dentin; however, the least adverse effect was observed with calcium hydroxide in the cervical third and with propolis in the middle and apical thirds.
Calcium hydroxide demonstrated the highest POBS of BioRoot RCS to root canal dentin, followed by mTAP and propolis, with no statistically significant difference between mTAP and propolis in the cervical third. In contrast, propolis exhibited the highest bond strength, followed by calcium hydroxide and mTAP in the middle and apical thirds, with no statistically significant differences between calcium hydroxide and mTAP in these regions. Overall, the POBS of BioRoot RCS to radicular dentin increased from the cervical to the apical third across all 3 study groups.
Future perspectives
Further research may be conducted to evaluate the following parameters: the detailed interaction between propolis ICM residues and calcium silicate-based bioceramic sealers; the effect of prior application of various ICMs, such as calcium hydroxide, mTAP and propolis, on the POBS of bulk-fill bioceramic sealers without GP cones to root canal dentin; and the influence of propolis residues on the POBS of bioceramic sealers, with particular emphasis on comparing the efficacy of different irrigation protocols for their removal.
In addition, studies may assess the effect of these ICMs on the POBS of other commercially available bioceramic-based sealers apart from BioRoot RCS. Scanning electron microscopy analysis may be employed to evaluate adhesion at the sealer–dentin interface, along with the characterization of the type of bond failure between bioceramic sealers and radicular dentin, using advanced analytical techniques. These investigations may provide valuable insights that could enhance material performance in clinical settings.
Ethics approval and consent to participate
The Institutional Ethics Committee at the AB Shetty Memorial Institute of Dental Sciences (ABSMIDS), NITTE (Deemed to be University), Mangaluru, India, approved and granted clearance to this study (ABSM/EC/102/2021). Written informed consent was obtained from all participants.
Data availability
The datasets supporting the findings of the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.