Abstract
Background. Bruxism, a repetitive masticatory muscle activity, is increasingly recognized as a behavioral marker with possible systemic implications. While its association with autonomic dysregulation has been proposed, the relationship between bruxism phenotypes and variations in circadian blood pressure (BP) in healthy individuals remains unclear.
Objectives. The aim of the study was to explore whether distinct behavioral bruxism phenotypes (sleep vs. awake, morning vs. evening) are associated with altered diurnal BP profiles, particularly postprandial patterns, in healthy normotensive young adults.
Material and methods. A total of 59 healthy young adults (mean age: 23.4 ±3.8 years) with probable bruxism were classified into 4 phenotypes: sleep bruxism (SB); morning awake bruxism (AB); evening AB; and undefined. The participants underwent 3 standardized BP measurements throughout the day (morning, postprandial and afternoon), alongside assessment using the Pittsburgh Sleep Quality Index (PSQI), the Insomnia Severity Index (ISI) and the Epworth Sleepiness Scale (ESS). Bruxism classification was based on self-reports, clinical signs and timing patterns. Data was analyzed using analysis of variance (ANOVA) and post hoc tests. Confidence intervals and effect sizes were calculated, and boxplots were used to illustrate group differences.
Results. Participants with SB exhibited a significantly steeper postprandial diastolic BP decline compared to other phenotypes (p = 0.045), deviating from the expected parasympathetic post-meal dip observed in healthy profiles. Sleep bruxism was also associated with poorer sleep quality (higher PSQI scores), greater insomnia severity (higher ISI scores) and a lack of significant increase in daytime sleepiness. Individuals with morning AB showed a biphasic BP pattern suggestive of autonomic lability, while participants with evening AB exhibited a blunted profile. Questionnaire data reinforced a chronic hyperarousal profile among SB participants.
Conclusions. Behavioral bruxism phenotypes, particularly SB, may reflect underlying autonomic imbalance and altered circadian BP modulation, even in clinically normotensive individuals. These findings support the hypothesis that bruxism may serve as a behavioral marker of subclinical cardiovascular risk. Further studies incorporating objective autonomic markers and longitudinal data are warranted.
Keywords: bruxism, phenotypes, blood pressure, circadian
Introduction
Bruxism is a repetitive masticatory muscle activity involving clenching or grinding of the teeth and/or bracing or thrusting of the mandible. It is currently understood as a behavior, rather than a disorder, with possible functional or dysfunctional consequences depending on its intensity, duration and systemic context. A recent consensus has emphasized the importance of distinguishing between awake bruxism (AB) and sleep bruxism (SB).1 Interestingly, this classification primarily reflects a state-dependent distinction (i.e., wakefulness vs. sleep) rather than a strict circadian division in the physiological sense. While the timing of bruxism expression may be influenced by circadian processes, referring to AB and SB as circadian profiles may overstate the role of endogenous circadian regulation and should therefore be interpreted cautiously. Beyond the partial synchrony observed between some SB episodes and transient increases in blood pressure (BP),2 it is also possible that moment-to-moment variability in masticatory muscle activity throughout the 24-hour cycle contributes to cardiovascular dynamics. This is particularly relevant given the observed high intraindividual variability in SB behavior and the absence of a consistent correlation between the SB index and total sleep-time masseter muscle activity, as reported in recent electromyographic studies.3 Such findings suggest that bruxism-related motor fluctuations may operate independently of classic circadian markers, yet still exert physiologically significant effects on autonomic and hemodynamic regulation. Moreover, previous studies have proposed that individual chronotype may modulate the systemic impact of bruxism, particularly through its influence on autonomic tone and cardiovascular stress reactivity, further supporting the view that bruxism should be interpreted not only as a motor phenomenon, but as a potential biomarker of chronobiological and cardiometabolic dysregulation.4
In recent years, growing interest has emerged regarding non-pathological autonomic markers in youth, particularly those related to BP variability and circadian patterning, as potential indicators of early cardiovascular and neuroregulatory disturbances. Even in otherwise healthy individuals, daytime and circadian BP variation may reflect subclinical autonomic imbalance or altered sympathetic–vagal tone preceding overt cardiovascular dysfunction.5 It is plausible that behavioral and physiological cues, including sleep-related behaviors, modulate these patterns. Thus, assessing bruxism phenotypes in relation to diurnal BP rhythms may offer novel insights into early dysautonomia, especially in normotensive young adults. Recent investigations have emphasized sex-related and behavioral differences in self-reported bruxism and obstructive sleep apnea (OSA) symptoms, which may further influence the phenotypic expression and clinical relevance of bruxism-related cardiovascular outcomes.6
Blood pressure exhibits a predictable circadian rhythm in healthy individuals, characterized by a morning surge, a parasympathetically driven postprandial dip and afternoon stabilization.5, 7 However, the influence of bruxism phenotypes on this physiological BP pattern remains unexplored. This pilot study aimed to characterize BP variations in young adults with distinct bruxism profiles and to explore whether these variations could reflect behavioral circadian phenotypes (i.e., behavioral expressions of bruxism timing) potentially associated with autonomic imbalance. We hypothesized that different bruxism subtypes, particularly SB, would show altered circadian BP profiles.
Material and methods
Study design and participants
A total of 178 healthy university students (mean age: 21.3 ±1.5 years; 74.6% female) were evaluated. All participants provided informed consent. The inclusion criteria encompassed self-reported tooth grinding or clenching, the presence of at least 1 clinical sign (e.g., tongue indentation, linea alba), and the absence of current medical conditions or use of medications affecting cardiovascular or sleep function. The exclusion criteria included hypertension, diabetes, heavy smoking, inflammatory conditions, and the use of medications influencing the autonomic nervous system. A cross-sectional analysis was conducted among 59 participants (mean age: 23.4 ±3.8 years; mean body mass index (BMI): 26.07 ±2.72 kg/m2) with probable bruxism, as confirmed by diaries and clinical signs.
Bruxism classification
Bruxism was assessed using 2 self-report questionnaires translated into Portuguese, based on the studies by Winocur et al. and Pintado et al.8, 9 In the first questionnaire, bruxism was considered probable when participants answered affirmatively to question 1 and/or question 2 (concerning awareness of grinding or clenching) and reported at least 1 symptom-related item in question 3 (e.g., jaw discomfort or tooth wear).8 In the second questionnaire, bruxism was classified as present when at least 2 items received a positive response.9
Participants were then classified according to different circadian profiles: AB (morning – reported in the first 3 h after awakening; evening – reported in the last 3 h before bedtime); SB (bruxism reported during sleep only); and undefined (bruxism reported inconsistently throughout the day, including overlap among different types or patterns that could not be clearly categorized).
Blood pressure measurement
Blood pressure was measured with a validated oscillometric device (Physiogard TM 910; SCHILLER AG, Baar, Switzerland), according to the European Society of Hypertension (ESH) guidelines.10 Each participant underwent 6 seated BP measurements daily (2 readings at each of the 3 timepoints: morning, postprandial and afternoon) over the course of 3 days. Readings were taken in a quiet, temperature-controlled room (22–24°C) by trained personnel using appropriately sized cuffs after 5 min of rest and in the absence of recent caffeine intake or exercise.
Sleep and lifestyle questionnaires
All participants completed a battery of self-report questionnaires that had been previously validated in Portuguese and widely applied in sleep research and clinical practice.
Chronotype was assessed using the morningness–eveningness questionnaire (MEQ).11 Sleep quality was evaluated using the Pittsburgh Sleep Quality Index (PSQI),12 insomnia symptoms were analyzed with the Insomnia Severity Index (ISI),13 and daytime sleepiness was assessed with the use of the Epworth Sleepiness Scale (ESS).14 The risk of OSA was evaluated using the Berlin Questionnaire.15 These instruments were analyzed descriptively and explored for associations with BP and bruxism profiles.
Statistical analysis
Descriptive statistics were computed for all variables, including mean (M) and standard deviation (SD). The Shapiro–Wilk test was applied to assess normality, and Levene’s test was used to evaluate the homogeneity of variance.
Group comparisons for continuous variables were performed using one-way analysis of variance (ANOVA) or Kruskal–Wallis tests, as appropriate, followed by post hoc analyses. Categorical variables were analyzed using the χ2 test. Effect sizes (Cohen’s d) were calculated for two-group comparisons, and 95% confidence intervals (95% CIs) were reported to better evaluate the clinical relevance of the findings. A post hoc power analysis indicated sufficient power (0.78) to detect medium effect sizes (f = 0.25).
All statistical analyses were conducted using the IBM SPSS Statistics for Windows software, v. 24.0 (IBM Corp., Armonk, USA). A two-tailed p-value of <0.05 was considered statistically significant.
Results
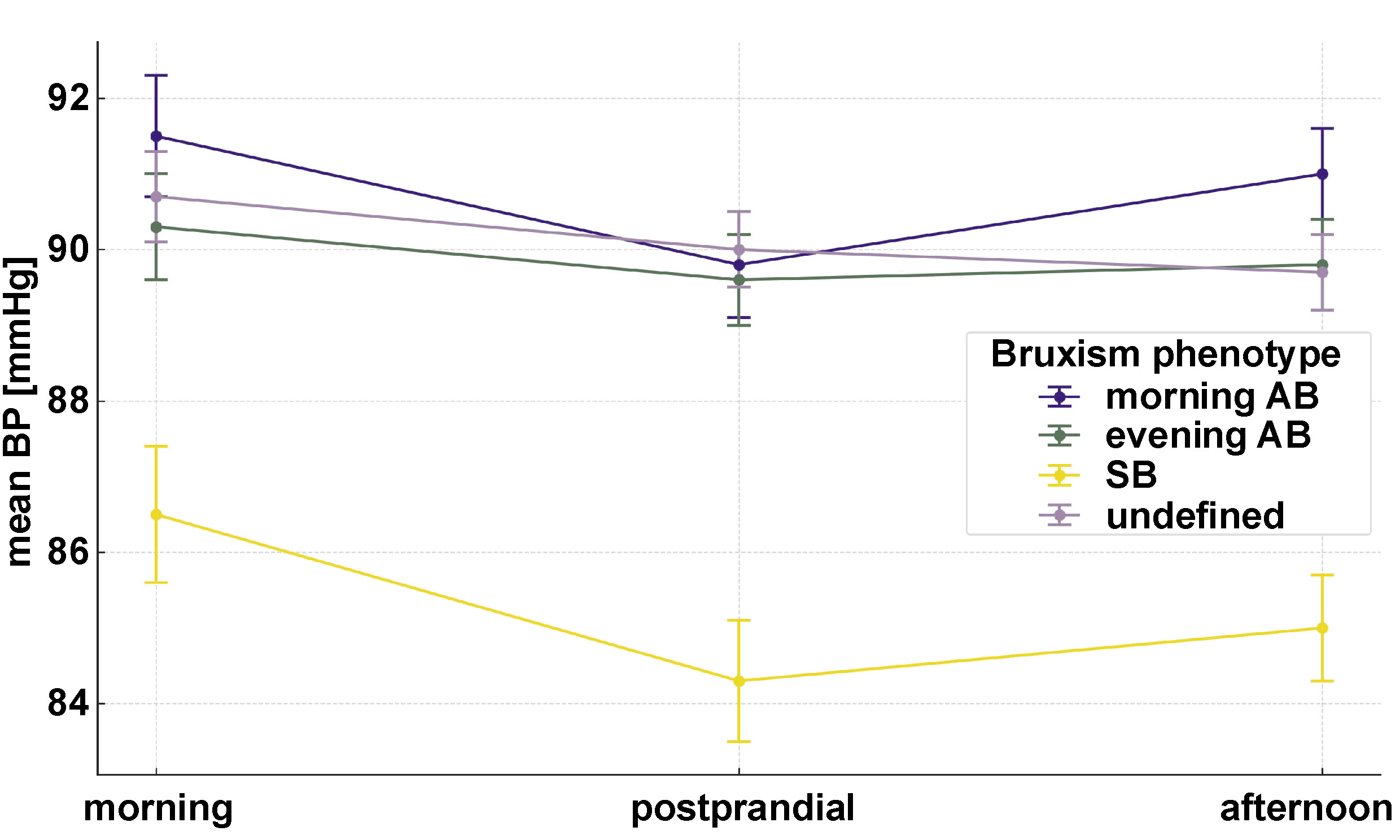
Among the 59 individuals with probable bruxism, 20 were classified as having SB, 15 with morning AB, 12 with evening AB, and 12 as undefined. While none of the participants met the criteria for hypertension during the standardized BP assessments, distinct BP variation patterns emerged across phenotypes. None of the bruxism subgroups displayed the expected physiological circadian BP pattern, characterized by a morning surge, a postprandial dip and afternoon stabilization. Instead, each phenotype exhibited a deviant trajectory (Figure 1).
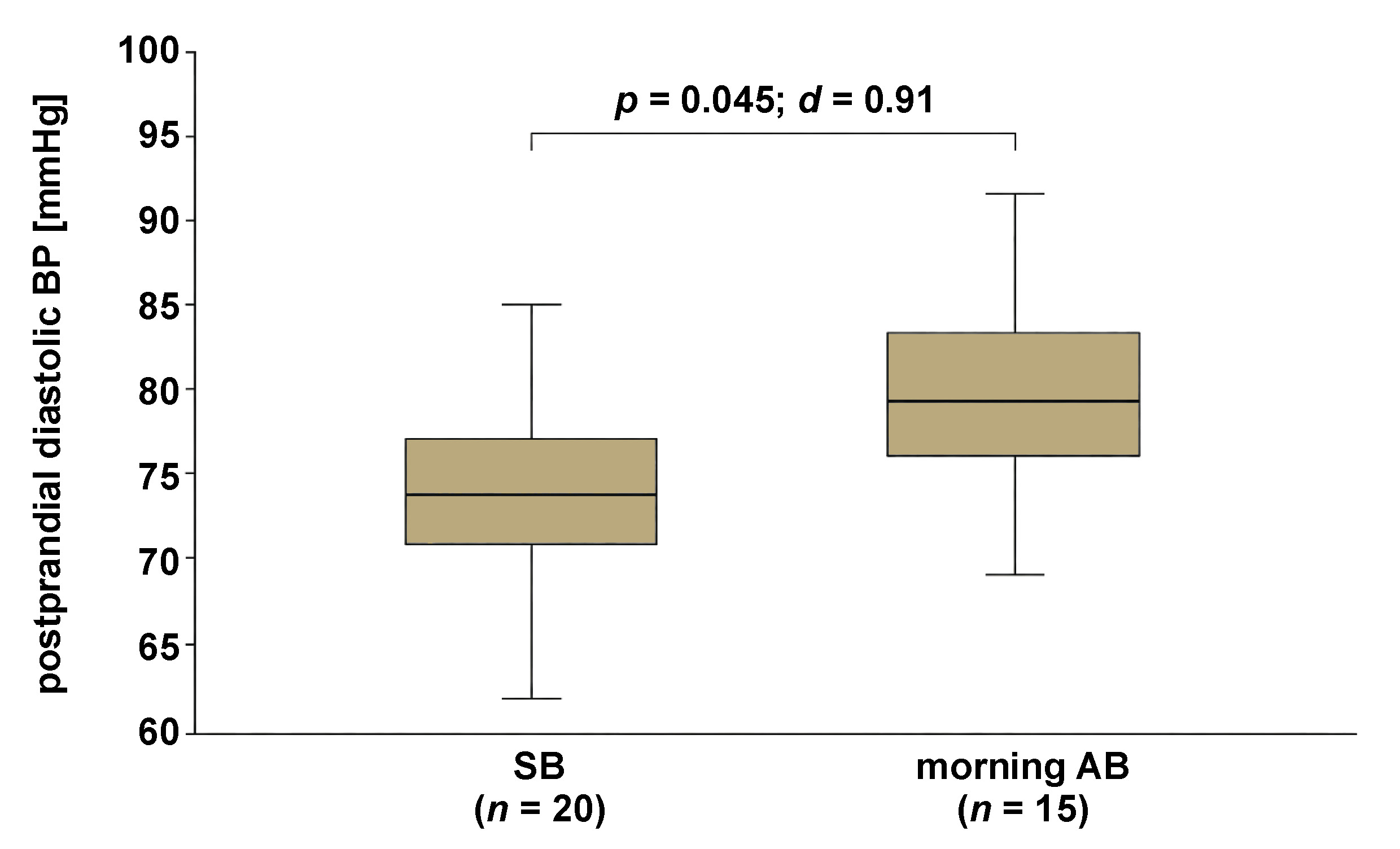
The SB group showed a significantly lower mean postprandial diastolic BP (74.1 ±6.2 mmHg) compared to the morning AB group (79.6 ±5.8 mmHg; p = 0.045), with a Cohen’s d of 0.91 (95% CI: 0.10–1.72), indicating a large effect size (Figure 2). Morning systolic BP values were as follows: SB – 113.4 ±9.2 mmHg; morning AB – 117.1 ±8.7 mmHg; evening AB – 114.6 ±9.1 mmHg. Postprandial systolic BP averaged 110.3 ±8.9 mmHg in SB, 114.5 ±9.6 mmHg in morning AB and 113.0 ±8.4 mmHg in evening AB. Afternoon systolic BP values were 112.7 ±9.4 mmHg in SB, 118.0 ±10.1 mmHg in morning AB and 112.8 ±9.8 mmHg in evening AB.
In a complementary analysis comparing participants with probable bruxism (n = 59) to those without (n = 119), no significant differences were found in morning or afternoon systolic and diastolic BP values. However, participants with probable bruxism showed a non-significant trend toward lower postprandial diastolic BP (76.2 ±6.9 mmHg vs. 78.4 ±6.5 mmHg; p = 0.071, Cohen’s d = 0.33, 95% CI: −0.5–0.02). No significant differences were observed in systolic BP at any timepoint (all p > 0.10). These results support the phenotypic distinctions observed across subgroups rather than a global bruxism-related BP alteration.
Participants with SB also showed significantly higher insomnia severity scores (ISI = 10.4 ±3.3) and poorer sleep quality (PSQI = 7.8 ±2.1), further supporting the presence of sleep-related vulnerability.
In terms of sleep parameters, the SB group exhibited significantly higher scores for insomnia severity (ISI = 10.4 ±3.3) compared to the morning AB group (ISI = 7.6 ±2.9; p = 0.021, Cohen’s d = 0.91, 95% CI: 0.12–1.70) and the evening AB group (ISI = 6.8 ±2.7; p = 0.008, Cohen’s d = 1.18, 95% CI: 0.35–2.01). Sleep quality assessed using the PSQI was also poorer in the SB group (7.8 ±2.1) compared to the morning AB group (5.3 ±1.8; p = 0.009, Cohen’s d = 1.28, 95% CI: 0.40–2.16) and the evening AB group (5.1 ±1.7; p = 0.007, Cohen’s d = 1.40, 95% CI: 0.49–2.31). No statistically significant differences were observed for excessive daytime sleepiness (ESS) or OSA risk (Berlin Questionnaire). The SB group tended to show higher risk classifications in the Berlin Questionnaire, although without reaching statistical significance.
Discussion
This pilot study suggests that distinct clinical bruxism phenotypes may be associated with altered circadian BP variation in healthy normotensive young adults. While all participants were clinically normotensive during baseline assessment, none of the bruxism subgroups displayed the expected physiological circadian BP pattern, characterized by a morning surge, a postprandial dip and afternoon stabilization. The absence of a normal rhythmic profile across all phenotypes suggests a systemic alteration of autonomic regulation rather than isolated or subgroup-specific anomalies, highlighting the potential role of subclinical dysautonomia even in healthy individuals.
The lower postprandial BP observed in the SB group, when interpreted in conjunction with poor sleep quality and higher insomnia scores, may point toward a maladaptive autonomic response rather than robust vagal tone. Previous studies have shown that SB is associated with sympathetic surges during sleep,2 and these nocturnal events may disrupt daytime vascular regulation through impaired baroreflex sensitivity or increased arterial stiffness.16 Furthermore, the higher ISI and PSQI scores among SB individuals reinforce the hypothesis of a chronic hyperarousal state, which could contribute to both nocturnal motor activity and diurnal hemodynamic rigidity. While one might interpret lower postprandial BP as a marker of preserved or even increased parasympathetic tone, the co-occurrence of poor sleep quality and elevated insomnia severity supports the view of a maladaptive or dysregulated response rather than a protective physiological adaptation. The lack of differences in daytime sleepiness suggests that these alterations occur despite preserved subjective daytime alertness.
The biphasic BP response observed in individuals with morning AB may represent a more labile autonomic profile, potentially driven by psychological hyperarousal or stress anticipation.17 Individuals with evening AB, in turn, showed a rigid BP profile, which may be associated with decreased autonomic adaptability, a phenomenon observed in both late chronotypes and individuals at higher risk for hypertension and cardiometabolic dysfunction.18 However, these mechanistic hypotheses, though plausible, remain speculative due to the absence of objective autonomic or endocrine measures. As such, these interpretations should be framed cautiously and validated in future studies using physiological or neuroendocrine biomarkers.
Importantly, however, when comparing all participants with probable bruxism to those without, no significant differences in overall systolic or diastolic BP were found. This suggests that the presence of bruxism per se may not be associated with broad alterations in BP profiles. However, the distinct circadian BP patterns observed across bruxism phenotypes support the notion that behavioral timing and subtype may be more informative than the binary classification of bruxism presence or absence. These findings reinforce the need for more granular phenotyping in sleep and autonomic research.
The results of the present study support the notion that bruxism, far from being a purely local orofacial activity, may reflect broader autonomic and circadian dysregulation. This is consistent with research reporting associations between bruxism, cardiovascular stress load and allostatic overload,19 and aligns with evidence indicating that markers of systemic physiological rhythm, such as circadian and autonomic indicators, are increasingly relevant even in complex critical contexts.20 This is not a diagnostic sign, but rather a signal of altered regulation worthy of further study. In fact, circadian clock disruption has been proposed as a contributor to cardiometabolic dysfunction in both acute and chronic settings,21 while bruxism-related dysautonomia may represent an early behavioral signal of such disruption.21, 22 Beyond the autonomic nervous system, other key physiological systems involved in BP regulation, such as the renin–angiotensin–aldosterone system (RAAS), endothelial nitric oxide signaling, vascular reactivity, and low-grade inflammation, may contribute to the BP variation patterns observed across bruxism phenotypes. Although not directly measured herein, their relevance is well-established and supports a broader framework for interpreting our findings.23 Additionally, external behavioral and environmental variables (e.g., caffeine intake, smoking, stress exposure, and light–dark cycle alignment) were not controlled for, potentially contributing to interindividual BP variability. This underscores the exploratory nature of the study, which is not confirmatory but hypothesis-generating.
Mechanistically, circadian clock gene dysregulation and sleep fragmentation, which may occur in patients with high-frequency SB, can disturb cardiometabolic status,24 eventually affecting autonomic sensitivity and the expected diurnal BP decline.25 These findings align with the broader literature on chronobiology and provide a relevant foundation for future investigations.
On the other hand, the multidimensional nature of bruxism, including its potential origins in central sensitization, social context and biopsychosocial vulnerability, underscores the relevance of integrated phenotyping approaches that go beyond surface-level behavioral classification. Notably, while self-reported bruxism may lack polysomnographic precision, its integration with validated questionnaires can provide valuable behavioral insight, particularly in populations with sleep complaints or risk factors, as demonstrated in large-scale survey studies.6, 26
Apart from the cardiovascular and autonomic implications, bruxism phenotypes may also present with associated somatic symptoms, such as headaches, jaw muscle pain and dental clenching behaviors, which further reflect dysregulated neurosensory processing. Evidence indicates that individuals with SB often report tension-type or temporomandibular-related headaches, potentially mediated by sustained muscle hyperactivity or trigeminal sensitization.27 Moreover, behavioral features such as diurnal clenching may signify an expression of stress-coping strategies or emotional dysregulation, consistent with findings linking bruxism to central sensitization and somatization syndromes.28 These overlapping mechanisms confirm that bruxism is not solely a local motor event but may represent a systemic neurobehavioral condition influenced by affective, neuroendocrine and circadian factors.
From a clinical standpoint, recognizing bruxism phenotypes as potential early indicators of abnormal BP regulation could inform preventive strategies in sleep medicine and cardiovascular care. Patients presenting with bruxism, particularly SB and evening AB profiles, may benefit from additional screening for sleep fragmentation, stress exposure and circadian misalignment. Such integrative approaches could be further strengthened by considering the co-occurrence of bruxism and OSA, especially in light of emerging endotypic models and pathophysiological overlaps.29 Still, bruxism may become a valuable behavioral marker in future models of cardiovascular risk assessment.
Limitations
This is a preliminary study with several limitations. The sample size was modest, particularly for subgroup analyses. Bruxism was not confirmed with polysomnography or electromyography. Additionally, we did not use 24-hour ambulatory BP monitoring, which limits the interpretation of full circadian variation and nocturnal dipping profiles. The cross-sectional design prevents causal inferences between bruxism phenotypes and BP alterations. Moreover, potential confounding factors such as perceived stress, anxiety, caffeine consumption, and lifestyle-related variables were not assessed. These are known to influence both bruxism expression and BP variability and may have impacted the observed associations. Future studies should control for these elements to better delineate the specific contribution of bruxism-related mechanisms.
Nevertheless, the standardized methodology, repeated BP measurements under controlled conditions and the use of validated sleep and chronotype questionnaires contribute to the robustness of our observations. On the other hand, although self-reported bruxism showed limited correlation with laboratory-based measurements of masticatory muscle activity, it should not be dismissed outright. Subjective complaints often reflect the patient’s perceived burden and may capture broader psychophysiological disturbances, including stress sensitivity, arousal patterns and sleep fragmentation. These factors may be omitted when using objective indices alone. Thus, incorporating self-reported bruxism remains relevant, especially in the assessment of behavioral phenotypes with potential cardiovascular implications. These findings should serve as a basis for further investigations using larger samples, more standardized criteria30 and objective autonomic measures.
To the best of our knowledge, this pilot study is one of the first to investigate behavioral phenotypes of bruxism as potential markers of altered circadian BP profiles in a healthy young population. By integrating a multidimensional assessment, including time-specific bruxism subtypes, structured BP measurements and validated sleep-related questionnaires, this research presents a novel perspective on how seemingly benign oral behaviors may reflect broader autonomic and chronobiological dysregulation. The findings support the growing paradigm that bruxism should be evaluated not only in dental or musculoskeletal contexts but also as a systemic indicator with potential cardiometabolic implications. When validated in larger samples using objective physiological markers, this approach could contribute to early screening and preventive strategies targeting at-risk individuals before the onset of overt cardiovascular disease.
Conclusions
Distinct circadian BP patterns across bruxism phenotypes may reflect subtle autonomic differences, even in healthy individuals. While these findings are exploratory and based on a limited sample without objective confirmation of bruxism, they raise the hypothesis that behavioral phenotypes may offer a novel window into circadian–cardiovascular interactions. These observations should be interpreted cautiously but may nonetheless support future research using larger cohorts and objective physiological methods to clarify whether self-reported bruxism can serve as an early marker of autonomic dysregulation and cardiovascular risk.
Ethics approval and consent to participate
The study was approved by the Ethics Committee of the Faculty of Medicine, University of Coimbra, Portugal (reference No. CE-012/2019). All participants provided written informed consent prior to participation.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
AI-assisted tools were used for language editing and manuscript organization. The authors are responsible for all scientific content, interpretation and final approval.