Abstract
This systematic review aimed to assess the effectiveness of stabilization splints in the treatment of myogenous temporomandibular disorders (TMD).
The review was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. An electronic search was conducted in 2 databases – MEDLINE via PubMed and the Web of Science. The final search was conducted in May 2022.
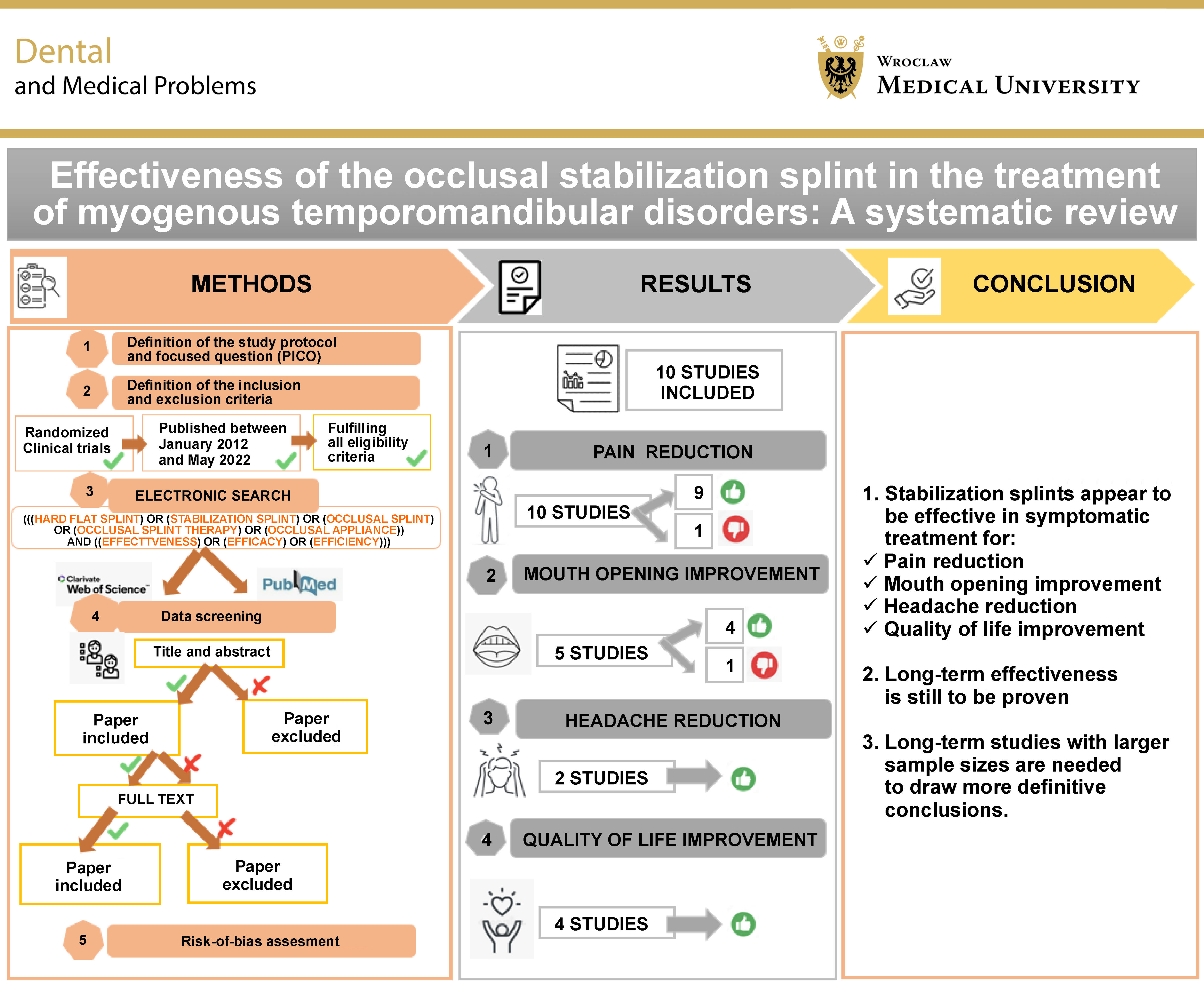
Ten randomized clinical trials (RCTs) were included. The total sample size was 539 participants, with a mean follow-up of 6 months. Four outcomes were assessed: pain reduction (10 studies); mouth opening improvement (5 studies); headache reduction (2 studies); and quality-of-life (QoL) improvement (4 studies). Most trials reported improvement in TMD symptoms in comparison with the baseline measures. Nevertheless, the overall quality of evidence was low due to moderate to high risk of bias and the small sample sizes.
Given the limitations of the systematic review, occlusal stabilization splint therapy appeared to be effective in reducing the signs and symptoms of TMD. However, further large-scale prospective studies are needed to evaluate its long-term effectiveness.
Keywords: systematic review, effectiveness, stabilization splint, TMJ disorders, myogenous
Introduction
Temporomandibular disorders (TMD) comprise a group of neuromuscular and musculoskeletal conditions affecting the masticatory muscles, temporomandibular joints (TMJs), and/or associated structures.1, 2 The prevalence of TMD is estimated to range from 5% to 12% in the general population, with rates reaching up to 30% among young adults.3 This dysfunction is commonly characterized by pain in the TMJs or masticatory muscles, restricted or deviated mandibular movement, and joint sounds, such as clicking or crepitus, during mandibular function. Additional symptoms may include headaches, earaches, poor sleep quality, and depression.4 The etiology of TMD is complex and multifactorial. Contributing factors include trauma, parafunctional habits, stress, postural abnormalities, neuromuscular dysfunction, and psychosocial factors.5, 6, 7
Temporomandibular disorders represent a prevalent condition with substantial effects on quality of life (QoL), often characterized by chronic pain and limitations in daily activities.8, 9, 10 Given the multifactorial nature of TMD, a wide range of treatment approaches has been proposed. Current evidence supports prioritizing the most conservative and reversible interventions aimed at relieving pain, restoring normal function, and improving the patient’s physical and psychological well-being.6 Accordingly, therapeutic approaches are generally classified into 3 categories: non-invasive; semi-invasive; and invasive.
Non-invasive and reversible treatment, also referred to as conservative therapies, may be applied alone or in combination. These include splint therapy, manual therapy, pharmacotherapy, counseling, therapeutic education, postural training, acupuncture, LED therapy, low-level laser therapy (LLLT), and therapeutic ultrasound. More advanced categories involve semi-invasive and surgical interventions.6, 11, 12
There are 2 main categories of dental splints used in splint therapy: occluding splints; and non-occluding splints.13 The most commonly used types include stabilization splints, anterior repositioning splints and anterior occlusal splints.14 Each type is intended to address specific clinical symptoms. Stabilization splints, also referred to as hard acrylic splints, are fabricated from rigid acrylic resin.13, 15 These appliances present a flat and smooth occlusal surface that allows the opposing teeth to contact evenly and simultaneously in centric relation.16, 17 In maximum intercuspation, occlusal contacts are designed to be simultaneous and symmetrical. During lateral mandibular movements, canine guidance is maintained. When necessary, additional occlusal adjustments may be performed during follow-up visits.13 Although the exact mechanism of action of stabilization splints remains unclear, they are believed to reduce masticatory muscle fatigue, promote stable occlusion, minimize occlusal interferences, and decrease neuromuscular activity.
The effectiveness of occlusal stabilization splints in reducing the signs and symptoms of myofascial pain, particularly masticatory muscle pain, has been reported by numerous authors. However, the mechanisms underlying these effects have not been fully elucidated. The literature reports inconsistent findings, which may be attributed to sample heterogeneity, the absence of standardized diagnostic criteria, such as the Research Diagnostic Criteria (RDC) for TMD, and differences in follow-up duration. Only a limited number of studies have demonstrated superior clinical outcomes associated with stabilization splint therapy in the management of TMD.11 In addition, few investigations have examined the role of stabilization splints in reducing temporalis and masseter muscle activity. Several studies have also reported that the effects of stabilization splints on TMD are comparable to those achieved with non-occluding control splints. Consequently, the literature presents conflicting evidence regarding the effectiveness of stabilization splint therapy, despite promising results reported for muscle energy techniques in the management of TMD.11, 18
Therefore, this systematic review aimed to evaluate published randomized controlled trials (RCTs) investigating the efficacy of occlusal stabilization splints in the management of orofacial myalgia and myofascial pain in comparison with no treatment or alternative interventions.
The objective of this study was to assess the effectiveness of stabilization splints in reducing the most common myogenic symptoms associated with TMD, including pain, limitation in mouth opening, headaches, and impaired QoL. The null hypothesis was that stabilization splints promote muscle relaxation and are effective in managing these symptoms.
Methodology
Protocol and focused question
This systematic review was conducted according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) statement.19
The main objective of this research was to answer the following question: Are stabilization splints effective at treating myogenous TMD?
Criteria for considering studies for the systematic review
The review included trials involving participants diagnosed with myogenous TMD according to the Research Diagnostic Criteria for Temporomandibular Disorders (RDC/TMD) or the updated Diagnostic Criteria for Temporomandibular Disorders (DC/TMD).20 Participants were eligible if they were older than 18 years, had no history of TMJ surgery, and had no significant comorbidities, such as neurological, rheumatologic or malignant diseases. Individuals with bruxism or sleep apnea were excluded.
The review included clinical trials in which participants received a specific type of occlusal splint – namely stabilization splints – and were compared or not with a control group.
Four outcomes were assessed: (1) pain reduction; (2) mouth opening improvement; (3) headache reduction, and (4) QoL improvement. The maximum follow-up duration was 6 months, and only studies with a minimum follow-up of at least 1 month were included.
Only RCTs were included in this systematic review.
Study selection
An electronic search was carried out in the MEDLINE/PubMed and Web of Science databases, using the following search formula: (((hard flat splint) OR (stabilization splint) OR (occlusal splint) OR (occlusal splint therapy) OR (occlusal appliance)) AND ((effectiveness) OR (efficacy) OR (efficiency))). Randomized clinical trials published between January 2012 and May 2022 were identified. The final electronic search was conducted in May 2022.
The search strategy is presented in Table 1.
Data screening
Article selection was performed by consensus between 2 authors (YB and HBM), based on the predefined and mutually agreed inclusion and exclusion criteria. Both reviewers independently screened the titles and abstracts of all identified studies. When the title or abstract did not provide sufficient information to determine eligibility, the full text was retrieved and assessed prior to making a final decision on inclusion or exclusion. Only studies that fulfilled all eligibility criteria of this systematic review were included.
Inter-rater reliability was assessed using percent agreement between the 2 reviewers, and was estimated at approx. 82%.
Data extraction and management
Data extraction was performed independently by the 2 previously mentioned reviewers. The extracted information included study characteristics such as authors’ names, study design (sample size, sex distribution, mean age, and study protocol), TMD diagnostic criteria used, type of intervention, total follow-up duration, comparison, outcomes assessed, and main results. Any discrepancies in data extraction were resolved through consensus between the reviewers.
Inclusion and exclusion criteria
Only studies meeting the following inclusion criteria were considered eligible:
– randomized prospective clinical trials evaluating the efficacy of stabilization splints, with or without comparison to a control group;
– participants were predominantly patients diagnosed with myogenous TMD, aged over 18 years, with no history of prior TMJ surgery or significant comorbidities, including neurological, rheumatologic or malignant diseases, and without bruxism or sleep apnea.
The exclusion criteria were as follows:
– non-randomized or other study designs, including cohort studies, observational studies, and case reports;
– articles not available in English full text;
– inadequate or imprecise diagnostic criteria, where TMD classification was not based on either RDC/TMD or the updated DC/TMD20;
– studies with unreliable or inadequately reported outcome measurements;
– combination of stabilization splint therapy with another conservative therapy in the treatment group.
Quality of studies
Version 2 of the Cochrane Risk of Bias tool (RoB 2) was used to evaluate the reliability of the results of the included studies.21 Risk-of-bias and quality assessments were conducted independently by the 2 previously mentioned reviewers as part of the data extraction process. Any discrepancies or disagreement were resolved through discussion with a third reviewer (HB).
Results
Study selection and description
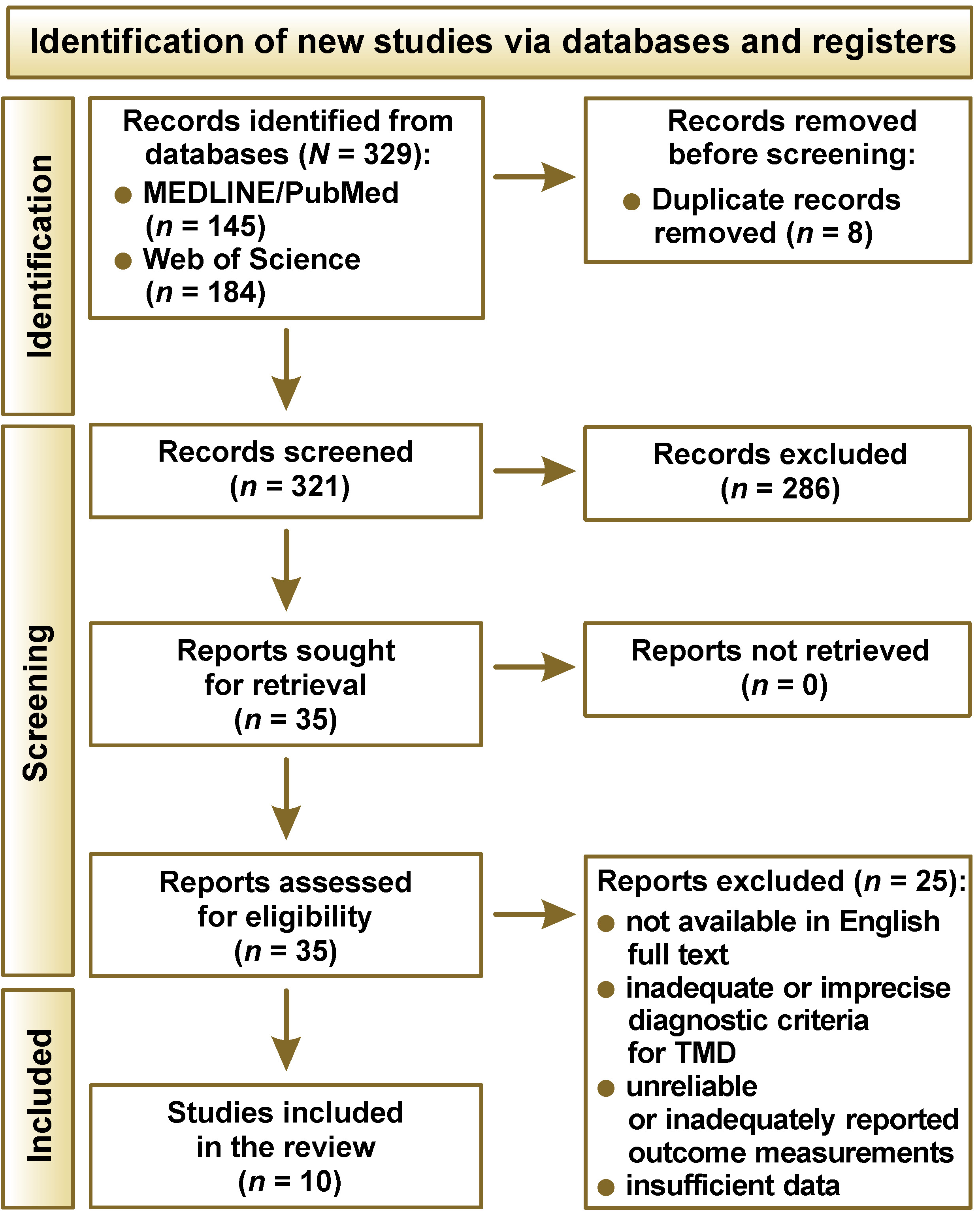
From the initial electronic search conducted in May 2022, 321 articles were identified, of which 10 were ultimately included in this systematic review, as illustrated in the PRISMA flow diagram (Figure 1).
The main characteristics of the included studies are presented in Table 2. Data extraction and analysis revealed considerable heterogeneity among the RCT samples. In total, 539 patients were included across the studies. Eligible participants were diagnosed with TMD based on RDC/TMD or the updated DC/TMD, including either Axis I or Axis II assessments. Not all clinical trials reported sex distribution. The maximum follow-up duration across the included studies was 6 months.
Risk-of-bias assessment
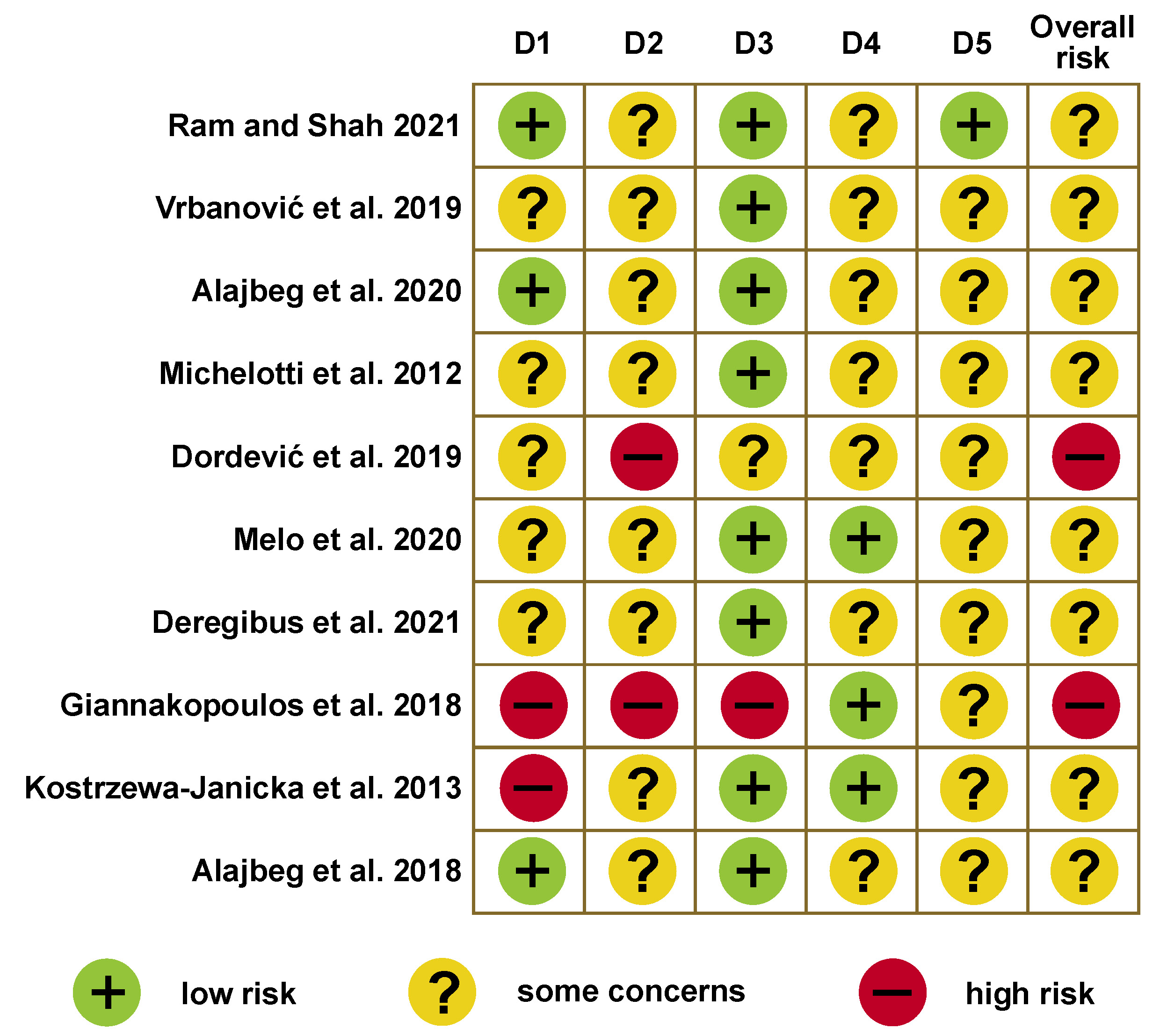
Risk-of-bias assessment using the Cochrane criteria indicated a moderate risk of bias in most of the included studies, while 2 studies were judged to have a high risk of bias (Figure 2).
Effectiveness of stabilization splints
The effectiveness of stabilization splints was assessed through four outcomes: improvement in pain, mouth opening, quality of life, and headaches. The findings of this systematic review were presented below.
Pain reduction
Pain is the most prevalent symptom reported by patients with TMD.1, 22 It is commonly described as a dull, persistent pain that may be aggravated by jaw function, particularly chewing. In the present systematic review, 10 studies evaluated pain-related outcomes.4, 16, 17, 23, 24, 25, 26, 27, 28, 29 Pain severity was primarily assessed using the visual analog scale (VAS),16, 23, 24, 25, 29 the numerical rating scale (NRS)27, 28 and/or the Graded Chronic Pain Scale (GCPS).16, 17 In one study, surface electromyography (sEMG) was used.26 The pain outcomes assessed varied among the included studies. Although pain intensity was the most frequently evaluated parameter, some clinical trials also assessed spontaneous pain, pain during chewing, muscle tenderness, average pain, and the worst pain. Most studies reported that stabilization splints were effective in reducing pain, with significant decreases in the VAS or NRS scores as compared to the baseline values. Michelotti et al. reported significant improvement in pain during chewing.23 Kostrzewa-Janicka et al. observed that, after a 2-month follow-up period, the NRS scores for orofacial pain decreased below 3 points in 77.5% of patients.28 According to Giannakopoulos et al., chronic pain intensity decreased by 40% after 3 months of splint therapy.27 In addition, Alajbeg et al. demonstrated a significant reduction in the worst pain scores.17 Vrbanović et al.16 and Dordević et al.24 in 2019, followed by Ram and Shah4 and Melo et al.,25 also concluded that stabilization splints were effective in reducing pain. However, despite the general trend toward pain reduction, Deregibus et al. concluded that stabilization splints were not significantly effective in reducing pain over a 6-month period, regardless of whether the splints were applied to the maxillary or mandibular arch.26
Mouth opening improvement
Temporomandibular disorders are frequently associated with impaired jaw function. Patients commonly report restricted or asymmetric mandibular movements, including limitations in mouth opening. This systematic review sought to evaluate the evidence regarding the effectiveness of stabilization splints in improving mouth opening. Five studies assessed improvement in mouth opening.16, 17, 23, 26, 29 Various measurement methods were used, the most common being maximum comfortable mouth opening (MCO) or pain-free maximum mouth opening (MMO).16, 17, 23, 29 This parameter corresponds to the maximum distance a patient can open their mouth without experiencing additional pain or discomfort. The measurement is obtained between the maxillary and mandibular incisal edges, with the overbite value added.17, 23, 29 All included studies, except that of Deregibus et al.,26 reported that stabilization splint produced significantly greater improvement in mouth opening. Most measurements, particularly pain-free MMO, showed significant increases when post-treatment outcomes were compared with the baseline values.
Headache reduction
In addition to pain and impaired jaw function, headaches are among the most common conditions associated with TMD.1, 30, 31 Headaches related to TMD are typically localized in the temporal region, preauricular area, and/or masseter muscles.30, 31 Although these headaches may be unilateral, they are often bilateral when both TMJs are involved. Two studies evaluated headache reduction.23, 28 The assessment methods varied, and included VAS, NRS and headache frequency. Overall, stabilization splints appeared to contribute to headache reduction. Kostrzewa-Janicka et al. reported a 3-point reduction in headache intensity in 61.8% of patients after 6 months of treatment.28 Furthermore, patients suffering from recurrent tension-type headaches reported a significant decrease in headache frequency following stabilization splint therapy.28
Quality of life improvement
Chronic TMD may significantly impair the patient’s QoL.29 They can affect social and emotional functioning, and may contribute to various psychological disorders.9, 25, 29 In addition, chronic pain may reduce independence in activities of daily living and negatively impact overall health-related quality of life (HRQoL).16 Consequently, one of the objectives of occlusal splint therapy in TMD management is to improve oral health-related quality of life (OHRQoL). Four studies evaluated this outcome using different questionnaires.16, 17, 25, 29 Vrbanović et al.16 and Alajbeg et al.29 assessed QoL using the Oral Health Impact Profile-14 (OHIP-14) questionnaire, and reported significant improvement following stabilization splint therapy. Improvement in QoL also involves reducing the psychological symptoms associated with TMD. Two clinical trials evaluated changes in anxiety and depression using various instruments, including the Generalized Anxiety Disorder-7 (GAD-7) questionnaire, the Patient Health Questionnaire-9 (PHQ-9),17 the Hospital Anxiety and Depression Scale (HADS), the Beck Anxiety Inventory (BAI), and the State-Trait Anxiety Inventory (STAI).25 According to these reports, stabilization splint therapy was effective in reducing depressive symptoms associated with TMD. Finally, the effectiveness of stabilization splints in improving QoL was also investigated through stress reduction. Alajbeg et al. assessed stress-related biochemical markers, including the uric acid levels, and reported a significant reduction in salivary oxidative stress index ratios among patients treated with stabilization splints.17
Discussion
Occlusal splints are among the most widely used conservative therapies for alleviating symptoms associated with myogenous TMD. The findings of this review suggest that stabilization splints represent a valuable and effective treatment option for the management of TMD symptoms.
Although the precise mechanism of action of stabilization splints remains unclear, their therapeutic effectiveness is thought to result from several factors. Stabilization splints may reduce electromyographic activity, modify the condylar position or increase the vertical dimension of occlusion. These changes may promote muscle relaxation and reduce stress on TMJS.26, 32 In addition, the adjustment of the splint surface to eliminate occlusal interferences may decrease sensory input to periodontal receptors and relieve pressure on the compromised retrodiscal tissues.
Despite its effectiveness, splint therapy presents several limitations. First, the fabrication of occlusal splints is a time-consuming and costly process for dental technicians, clinicians and patients, which may delay the initiation of treatment.13, 14, 23, 33 In addition, splints must possess adequate mechanical properties, particularly hardness and flexural resistance, to withstand excessive occlusal forces.13, 34 They must also demonstrate sufficient resistance to degradation within the oral environment. Although the conventional fabrication method remains the gold standard for achieving successful clinical outcomes, especially for long-term splint use, there is increasing demand for more efficient manufacturing techniques that reduce fabrication and management time. Advances such as tree-dimensional (3D) printing and thermoforming technologies have made this possible. However, further research is still required to improve the properties of the materials used in these techniques and to ensure long-term clinical success.34
The additional drawbacks of splint therapy include higher treatment costs and potential complications, such as caries and gingivitis.24 Moreover, several studies suggest that the effectiveness of stabilization splints is primarily limited to short-term outcomes. Alajbeg et al. found that stabilization splints demonstrated superiority over amitriptyline and placebo splints in improving limited mouth opening during the first 2 weeks.17, 29 Kostrzewa-Janicka et al. suggested that a 2-month observation period was generally sufficient to evaluate the effectiveness of occlusal splint therapy; if satisfactory improvement is not achieved within this timeframe, other contributing factors, such as stress or the underlying systemic conditions, should be investigated.28 In this regard, Olchowy et al. reported that patients who failed to improve were affected by tetany.32
The findings of the present review suggest that occlusal splints mainly provide symptomatic relief. Once TMD symptoms are alleviated, it is essential to identify the underlying etiological factors in order to establish and implement appropriate etiological treatment strategies.
Limitations
Several limitations of the present systematic review should be acknowledged, including heterogeneity among study samples, variability in follow-up periods and differences in the objectives of the included clinical trials. In addition, the absence of an untreated control group in several studies may have limited the ability to more precisely isolate the effects of stabilization splints. Furthermore, the findings cannot be considered definitive or fully generalizable due to the moderate to low methodological quality of the included studies. Most results should therefore be interpreted with caution, as outcome measures are partly subjective and may be influenced by individual pain tolerance thresholds. Consequently, further studies including non-treatment control groups are needed to allow a more rigorous evaluation of treatment effects.
Taking these limitations into account, the possibility that stabilization splints may have a superior therapeutic effect as compared to other treatment modalities cannot be excluded. Larger-scale studies with longer follow-up periods are required to clarify this uncertainty. In the included trials, the maximum overall follow-up duration was 6 months, which is insufficient to draw conclusions regarding the long-term effects of stabilization splint therapy.
Conclusions
This systematic review concluded that occlusal stabilization splint therapy met expectations in terms of effectiveness in reducing signs and symptoms in patients with myogenous TMD. Further large-scale, long-term prospective studies are needed to clarify these findings. Evidence-based conclusions are essential to improve the understanding and management of these and other common orofacial pain disorders.
Ethics approval and consent to participate
Not applicable.
Data availability
The datasets supporting the findings of the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.