Abstract
Orthodontically induced inflammatory root resorption (OIIRR) is a common complication of orthodontic treatment. Clear aligners (CA) are thought to deliver lighter, intermittent forces than fixed appliances (FA), potentially reducing the extent of root resorption. However, comparative evidence remains limited, particularly from studies using cone-beam computed tomography (CBCT).
This meta-analysis aimed to compare anterior tooth root resorption following treatment with CA vs. FA in patients with similar malocclusions, using CBCT-based linear measurements.
A systematic search of MEDLINE/PubMed, Embase and the Cochrane Library was conducted in accordance with the PRISMA guidelines. Studies were eligible if they included patients older than 14 years with fully developed anterior roots and comparable malocclusion severity, and if they used CBCT to assess changes in the root length before and after treatment with either CA or FA. The random-effects meta-regression model was used to estimate the weighted mean difference (WMD) in root resorption. Subgroup analyses were performed according to tooth type and extraction status.
Four high-quality cohort studies, comprising a total of 1,204 anterior teeth, met the inclusion criteria. Root resorption was significantly lower in the CA group than in the FA group (WMD: –0.47 mm; 95% CI: –0.55 to –0.40 vs. WMD: –0.54 mm; 95% CI: –0.75 to –0.33; p < 0.01). The difference was most pronounced in non-extraction cases involving the maxillary central incisors.
Clear aligners are associated with significantly less anterior root resorption than FA in patients with comparable malocclusions. Although the absolute difference is modest, CA may represent a favorable treatment option for patients at increased risk of OIIRR.
Keywords: orthodontic treatment, root resorption, fixed appliances, clear aligners, orthodontically induced inflammatory root resorption
Introduction
Orthodontically induced inflammatory root resorption (OIIRR) is one of the most common complications of orthodontic treatment, posing risks to tooth vitality and long-term periodontal health. As the global demand for orthodontic treatment continues to rise – particularly among adults – understanding and minimizing OIIRR has become increasingly important. Mild to moderate root resorption affects approx. 40–60% of patients, whereas severe resorption (>5 mm) occurs in 1–5% of cases and may compromise tooth stability and function.1, 2, 3 Orthodontically induced inflammatory root resorption most commonly affects the maxillary and mandibular incisors, as well as the maxillary canines, due to the extensive tooth movement often required during treatment.4, 5
Orthodontically induced inflammatory root resorption results from the breakdown of cementum and dentin, typically initiated when excessive orthodontic forces exceed capillary pressure within the periodontal ligament, leading to localized ischemia and necrosis.5, 6 When reparative processes are insufficient to counteract tissue damage, irreversible root resorption may occur. Several factors have been associated with increased susceptibility to OIIRR, including force magnitude and duration, root morphology, occlusal trauma, pre-existing conditions, and genetic predisposition, particularly polymorphisms in the IL-1β gene.3, 4, 5, 6, 7 Teeth with incomplete root formation or a history of endodontic treatment are generally considered more resistant to resorption.3, 4, 5, 6, 7 Importantly, the loss of 3 mm of the apical root structure is estimated to correspond to 1 mm of marginal bone loss in terms of periodontal support, while root loss exceeding 6 mm is regarded as a sign of severe structural compromise.6, 7, 8
Contemporary orthodontic treatment modalities include both fixed appliances (FA), which remain the standard for managing complex malocclusions, and clear aligners (CA), which are increasingly favored for their esthetics and patient comfort. Although CA therapy has been associated with reduced root resorption, likely due to lighter forces and shorter periods of force application,9 direct comparisons with FA must account for malocclusion severity to avoid biased conclusions.10
The radiographic assessment of root resorption remains challenging. Traditional two-dimensional (2D) imaging modalities, including panoramic and periapical radiographs, are limited by image distortion, magnification errors, and an inability to adequately detect buccal or lingual resorption.11, 12 In contrast, cone-beam computed tomography (CBCT), with its three-dimensional (3D) imaging capabilities, provides greater accuracy, repeatability and sensitivity for detecting subtle changes in root morphology.4, 5, 13, 14 Nevertheless, CBCT is associated with a substantially higher radiation dose, reported to be up to 33 times greater than that of panoramic radiography, depending on the field of view used.10
Previous meta-analyses comparing CA and FA have often lacked standardized imaging protocols and did not adequately control for differences in malocclusion severity.4, 9, 15, 16, 17 The present study aimed to directly compare the extent of root resorption associated with CA and FA using CBCT in cohorts matched for baseline malocclusion severity, thereby providing more robust and clinically relevant evidence.
Objectives
This meta-analysis aimed to determine whether the root resorption of the maxillary and mandibular anterior teeth in patients treated with CA is comparable to that observed in patients treated with FA, as assessed by CBCT in cases with similar malocclusions. The analysis was based on the root length measurements obtained from CBCT performed before and after active orthodontic treatment.
The null hypothesis was that no statistically significant difference exists in root resorption between the maxillary and mandibular anterior teeth treated with CA and those treated with FA, as measured by CBCT.
Methodology
The study was registered in The International Prospective Register of Systematic Reviews – PROSPERO (CRD42023471622), and conducted in accordance with the guidelines outlined in the Cochrane Handbook for Systematic Reviews of Interventions. The preparation of the systematic review and meta-analysis followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) framework, and included a systematic literature search, removal of duplicates, screening of titles and abstracts, and full-text assessment of selected studies.
Eligibility criteria (PICO framework)
To address the question of which treatment modality is associated with greater root resorption of anterior teeth, a search strategy based on the PICO framework was applied:
– Population: patients undergoing orthodontic treatment with fully developed anterior tooth roots;
– Intervention: treatment with CA;
– Comparison: treatment with FA;
– Outcome: root resorption measured in millimetres on CBCT images as the difference in the root length before and after the completion of orthodontic treatment.
Studies were considered eligible if they included patients older than 14 years with fully developed anterior tooth roots and comparable malocclusion severity. Eligible studies were required to use CBCT to assess changes in the root length before and after orthodontic treatment with either CA or FA.
The exclusion criteria were as follows: animal studies; study designs other than randomized controlled trials (RCTs), prospective or retrospective clinical studies, or single-group studies; the assessment of the root length using 2D radiographic methods (panoramic or periapical imaging); measurements performed before the completion of orthodontic treatment; studies involving patients with incomplete development of anterior tooth roots; the lack of comparability between groups in terms of malocclusion type or severity; patients with a history of dental trauma; and patients with endodontically treated anterior teeth.
Literature search and study selection
The MEDLINE/PubMed, Embase and Cochrane Library databases were searched (Table 1). The search was further expanded to include gray literature and reference lists. All publications were independently screened, selected and assessed by two authors (RS and MM). Following title and abstract screening, full-text articles were retrieved and evaluated for eligibility based on the inclusion criteria. Studies meeting the criteria were included in the final analysis. Any disagreement was resolved through consultation with a third author (BG).
Assessment of study quality and risk of bias
The quality of non-randomized studies was assessed using the Newcastle–Ottawa Scale (NOS), which evaluates 3 domains: the selection of study groups (case and control representativeness); the comparability of groups at baseline; and outcome assessment with adequate follow-up and independent or blinded evaluation. One point was awarded for each criterion indicating high methodological quality.18 The overall score was interpreted as follows: 7–9 points indicated grade A (good quality); 4–6 points indicated grade B (satisfactory quality); and 3 points or fewer indicated grade C (poor quality).19
The risk of bias was additionally evaluated using the ROBINS-I (Risk Of Bias In Non-randomized Studies – of Interventions) tool, which provides a structured framework for assessing bias across 7 domains that may occur before, during or after intervention implementation. These include: confounding (baseline differences between groups); the selection of participants; the classification of interventions; deviations from the intended interventions; missing outcome data; outcome measurement; and selective reporting. The ROBINS-I tool classifies studies into 4 levels of overall risk of bias: low; moderate; serious; and critical. A low risk of bias indicates that all or nearly all domains are at low risk, with only minor concerns regarding confounding. A moderate risk of bias is assigned when at least one domain raises moderate concerns, but none are serious or critical. A serious risk of bias indicates at least one domain with serious concerns or multiple domains with moderate concerns. A critical risk of bias reflects at least one domain with critical concerns, or multiple serious issues, and such studies are generally not recommended for inclusion in evidence syntheses.20
The risk of bias and methodological quality of all included studies were independently assessed by two authors (RS and MM). Any disagreement was resolved through discussion, and unresolved cases were adjudicated by a third author (BG).
Statistical analysis
Statistical analysis was performed using the R software, v. 3.6.1 (R Core Team, 2021; https://www.r-project.org). To evaluate differences in anterior tooth root resorption between the patients treated with FA and CA, the random-effects meta-regression model was applied. This approach combines meta-analysis and linear regression to assess the potential influence of study-level covariates on the effect size.
The treatment effect was expressed as a weighted mean difference (WMD) in millimetres, with corresponding 95% confidence intervals (CIs). Study weights were assigned using the inverse-variance method, thereby giving greater influence to studies with more precise estimates. The random-effects model was chosen a priori due to the anticipated clinical and methodological heterogeneity across the included studies.
Heterogeneity was assessed using the I2 statistic, with values above 50% considered indicative of substantial heterogeneity and prompting additional subgroup analyses. Subgroup analyses were performed to compare extraction vs. non-extraction cases, as well as according to tooth type and location (incisors, canines, the maxilla, and the mandible), which were considered potential effect modifiers.
In contrast, malocclusion severity and treatment duration were not included in the meta-regression model, as these variables were comparable across the included studies, and therefore unlikely to account for between-study differences in the effect size.
Given the limited number of included studies, sensitivity analyses and the formal assessment of publication bias (e.g., funnel plots or Egger’s test) were not performed, in accordance with methodological recommendations for low-powered datasets. A p-value <0.05 was considered statistically significant for all analyses.
Results
PRISMA flow of study selection
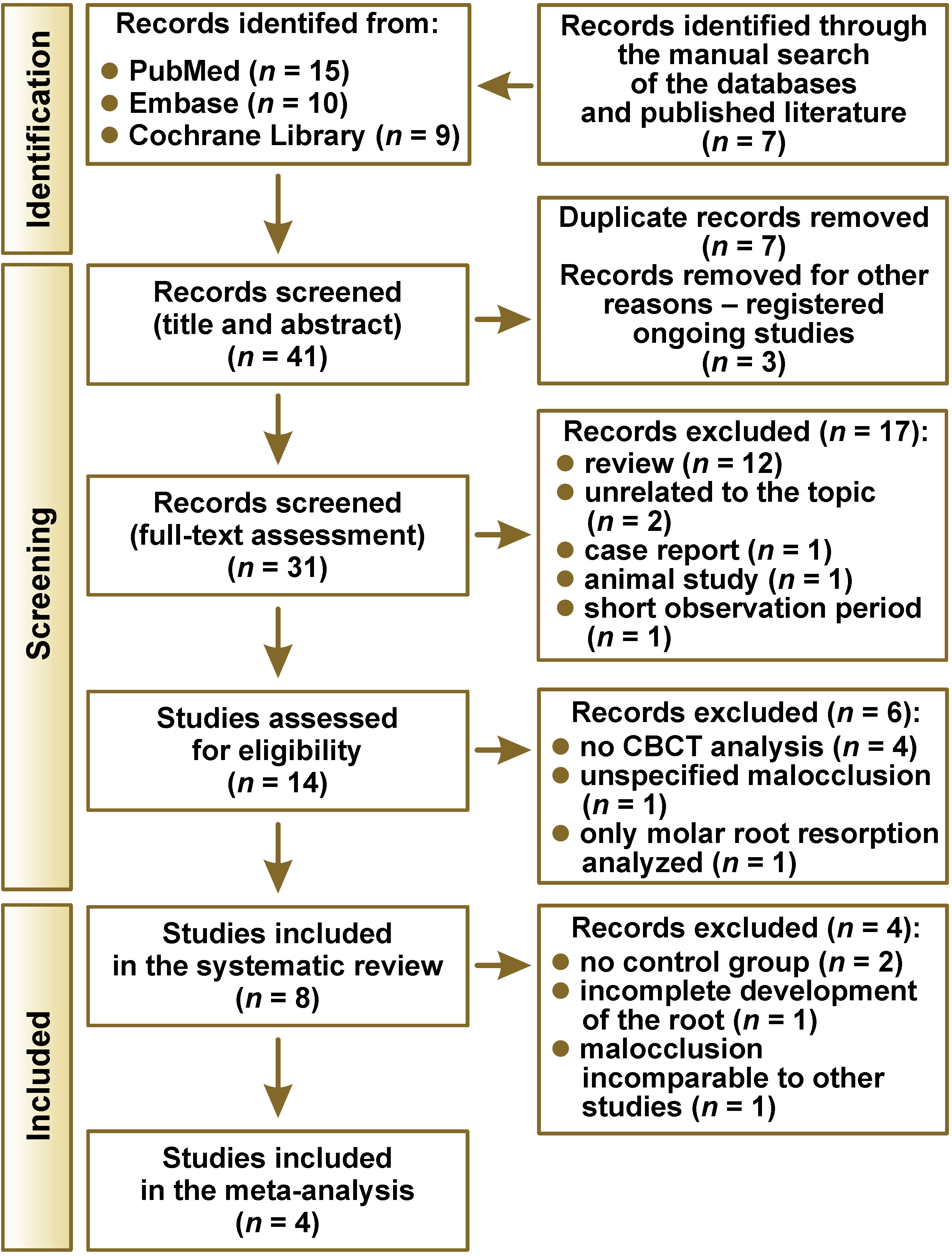
A total of 41 records were initially identified. After the removal of duplicates and the registered ongoing studies, 31 publications remained. Following title and abstract screening, 17 studies were excluded as review articles, or due to irrelevance to the topic, case report design, animal studies, or short observation periods. This resulted in 14 publications eligible for full-text assessment. Of these, 8 studies were included in the systematic review. Studies were excluded at this stage due to the absence of CBCT analysis,21, 22, 23, 24 the lack of specification of malocclusion type,25 or exclusive focus on molar root resorption.26 Ultimately, 4 studies qualified for the meta-analysis.10, 27, 28, 29 Additional exclusions were made for studies lacking a control group,8, 13 those involving teeth with incomplete root development,30 and to ensure a more homogeneous study population. Specifically, only cases of crowding in Class I malocclusion with comparable discrepancy index (DI) scores according to the American Board of Orthodontics (ABO) were retained, leading to the exclusion of a further 3 studies (Figure 1).8, 13, 31
Included studies
Eight studies were included in the qualitative synthesis (Table 2),8, 10, 13, 27, 28, 29, 30, 31 all of which were classified as high quality according to NOS (Table 3). However, the risk of bias varied among the included studies (Table 4). The majority were rated as having a moderate risk of bias,8, 10, 28, 29, 30, 31 while 2 studies were judged to have a low risk of bias.13, 27 In contrast, the study by Wang et al. was assessed as having a serious risk of bias, mainly due to the concerns related to confounding and outcome measurement.30 Importantly, only studies with a low27 or moderate risk of bias10, 28, 29 were included in the meta-analysis to ensure the validity and reliability of the quantitative synthesis.
Regarding outcome assessment, most studies measured root resorption using linear CBCT measurements comparing the root length before and after orthodontic treatment. However, Liu et al.13 and Chen et al.31 employed volumetric CBCT analysis, reporting changes in the root volume [mm3] rather than the linear root length. Although volumetric measurements may provide a more comprehensive representation of root resorption, only studies using linear CBCT measurements were included in the meta-analysis. This was not defined as a standalone inclusion criterion; rather, the studies applying volumetric analysis were excluded, as they did not meet other essential eligibility requirements, including the need for comparable malocclusion severity,13, 31 and the presence of both treatment and control groups.13
The study groups consisted of patients treated with CA, including Invisalign®, SmartTrack™ and Inman/In-line aligners, while the control groups comprised patients treated with FA, such as Victory Series™ and Damon Q™ systems. Notably, 2 studies did not include a FA control group.8, 13
With regard to malocclusion characteristics, the study by Aman et al. included a heterogeneous range of malocclusion types,8 whereas Liu et al.13 and Chen et al.31 focused specifically on Class II malocclusion treatment. In contrast, Almagrami et al.,27 Eissa et al.28 and Wang et al.30 and investigated patients with Class I malocclusion presenting anterior crowding. In the studies by Li et al.10 and Jyotirmay et al.,29 the specific malocclusion type was not explicitly stated; however, DI was reported to characterize baseline severity.
Most studies assessed the root length changes of the maxillary incisors8, 10, 13, 27, 28, 30, 31 and the mandibular incisors.10, 13, 29, 30 Additionally, Li et al.10 and Jyotirmay et al.29 included canines in their analyses.
Meta-analysis
Four cohort studies were included in the meta-analysis.10, 27, 28, 29 These studies evaluated patients older than 14 years with fully developed anterior tooth roots. In total, 1,204 teeth were assessed, including 602 in the CA group and 602 in the FA group.
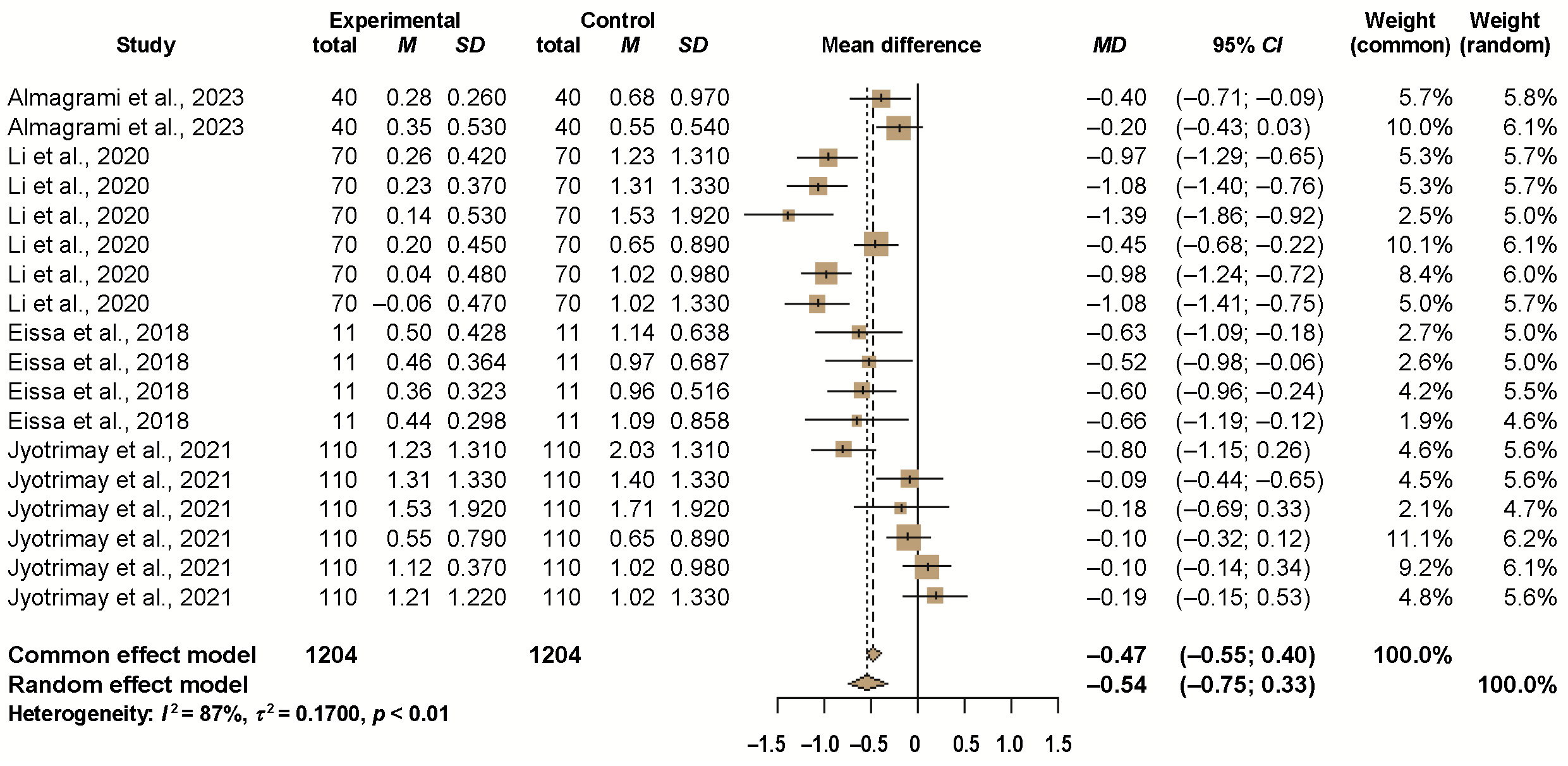
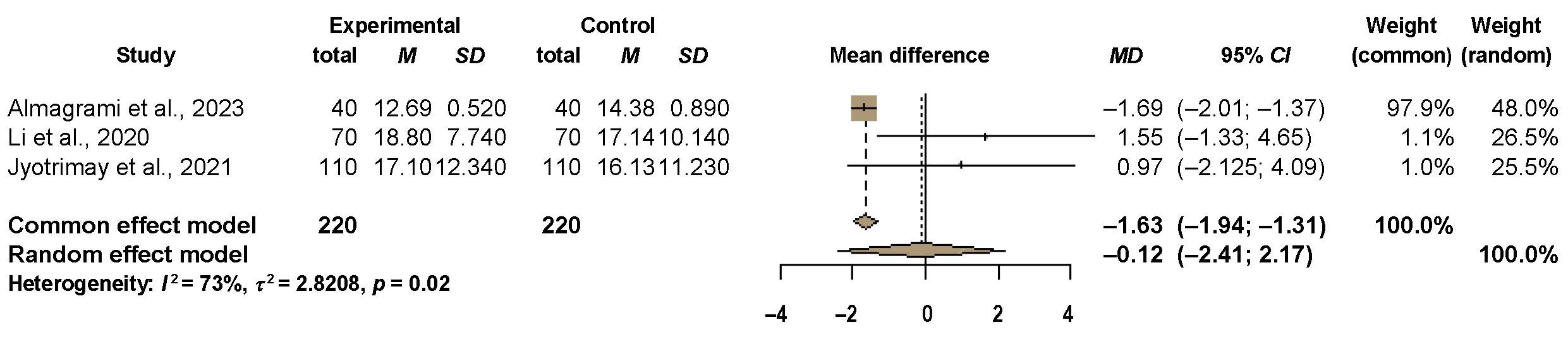
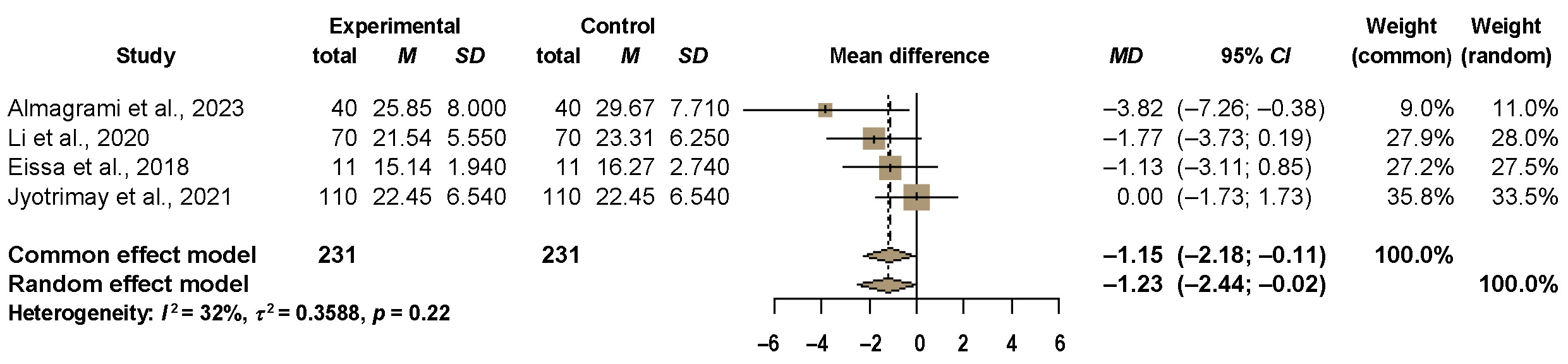
The studies included in the meta-analysis used matched groups based on the type of treated malocclusion. In 2 studies, patients presented with moderate anterior crowding,27, 28 whereas in the remaining studies, malocclusion was not explicitly defined10, 29; however, the DI, assessed according to ABO, was reported. No significant differences in the DI values were observed between groups. Neither DI nor treatment duration differentiated the study groups (Figure 2, Figure 3, Figure 4).
All included studies performed blinded CBCT-based assessments of root resorption, ensuring that evaluators were unaware of treatment allocation. In the study by Eissa et al., radiographic measurements were performed by a single blinded investigator,28 whereas in the remaining studies, assessments were conducted independently by two blinded examiners.10, 27, 29 To evaluate measurement reproducibility and reliability, Eissa et al. repeated assessments after a 4-week interval and analyzed agreement using the κ statistic for the systematic error and the Dahlberg formula for the random error, both confirming acceptable measurement accuracy.28 Li et al.10 and Almagrami et al.27 assessed inter- and intra-operator reliability using intra-class correlation coefficients (ICCs) based on repeated measurements performed at 2–4-week intervals. Both studies demonstrated excellent agreement, with the ICC values exceeding 0.97.10, 27 Among the 4 studies, the report by Jyotirmay et al. provided the least detailed methodology regarding reliability assessment.29 Although concordance between the two investigators was reported, the study did not describe the statistical approach or provide a quantitative analysis to support this claim.29
Root resorption in meta-analysis
Root resorption was statistically significantly lower in the CA group as compared to the FA group (WMD: –0.47 mm; 95% CI: –0.55 to –0.40 vs. WMD: –0.54 mm; 95% CI: –0.75 to –0.33; p < 0.01).
Subgroup analyses demonstrated that, in non-extraction cases,27, 28 the root resorption of the maxillary central incisors was significantly lower in patients treated with CA. In contrast, no statistically significant differences between the treatment modalities were observed for the maxillary lateral incisors. Similarly, in extraction cases,10, 29 significantly lower root resorption of the maxillary central incisors was observed in the CA group. No statistically significant differences between the treatment modalities were identified for the lateral incisors or canines (Table 5).
The WMD values further confirmed a statistically significant reduction in root apex resorption in the CA group as compared to the FA group. The greatest reduction was observed for the maxillary central incisors in non-extraction cases (p < 0.01).
Discussion
The present meta-analysis evaluated differences in the extent of anterior tooth root apex resorption between clear aligner therapy (CAT) and fixed appliance therapy (FAT) in comparable malocclusions, using CBCT examinations performed before and after treatment. Both CAT and FAT were associated with apical root resorption. However, the mean root loss was slightly lower in the CAT group (−0.47 mm) than in the FAT group (−0.54 mm). The confidence intervals for CAT (95% CI: −0.55 to −0.40) were narrower than those for FAT (95% CI: −0.75 to −0.33), which may indicate greater homogeneity of results within the CA group. The limited overlap between CIs suggests a potentially meaningful difference between the 2 treatment modalities. Although the inter-group difference reached statistical significance (p < 0.01), its absolute magnitude (0.07 mm) was small. Consequently, the clinical relevance of this difference may be limited, particularly if it remains within the range considered biologically harmless to tooth vitality. Nevertheless, these findings suggest that CAT may constitute a more conservative alternative with respect to the risk of root resorption, which could be particularly relevant in patients predisposed to OIIRR.
Both extraction and non-extraction cases were included in the analysis. In all studies included in the meta-analysis,10, 27, 28, 29 root resorption in the CA group was statistically significantly lower than in the FA group. The greatest difference in root apex resorption observed in this meta-analysis concerned the central incisors, which was consistent with the findings reported in 3 of the included studies.27, 28, 29 In contrast, Li et al. reported the greatest degree of resorption in the maxillary canines and lateral incisors.10 Previous literature has identified the maxillary lateral incisors as the teeth most susceptible to OIIRR, with an average root loss ranging from 1.2 to 1.6 mm. This increased vulnerability may be associated with the damage caused by the erupting canines. Both the maxillary lateral and central incisors appear particularly predisposed to resorption, likely because of their root morphology. Teeth with short, pointed, pipette-shaped, dilacerated, distorted, or curved roots are considered to be at greater risk.32, 33 Root resorption is generally more pronounced in the maxillary incisors than in the mandibular incisors, primarily due to the greater extent of tooth movement and overjet reduction during space closure, particularly in extraction cases. Therefore, carefully controlled orthodontic tooth movement remains essential for minimizing the risk of resorption.13
The type of malocclusion influences the extent of tooth movement, treatment mechanics, and, consequently, the risk of root resorption. Class II malocclusions and open bites are associated with a higher risk, as they often require greater ranges of tooth movement.3, 5 Accordingly, extraction cases appear to be particularly susceptible to this complication.5 In contrast, the influence of crowding correction on root resorption remains unclear.3, 8 Root resorption has been most strongly associated with intrusive movements, retraction,5 translation, lingual root torque,6 round tipping, and the use of interarch elastics.3 Increased resorption has also been reported when the root apex comes into contact with the palatal cortical plate, highlighting the importance of sagittal root positioning and careful radiographic monitoring throughout treatment. Proper torque control and carefully managed retraction mechanics are particularly important in Class II cases to minimize excessive root displacement.8, 13 A multivariate analysis conducted by Liu et al. demonstrated that approx. 51% of the variability in root resorption could be explained by factors such as the tooth type, the sagittal root position, extraction treatment, and the extent of intrusion and extrusion movements.13
Age is generally not considered a significant risk factor for root resorption,5, 13 with the exception that teeth with incomplete root development appear to be more resistant to this process.3 Longer treatment duration and the application of high orthodontic forces are associated with an increased risk of resorption.5, 6 However, treatment duration should be interpreted in relation to the active phases of orthodontic mechanics. The prolonged overall treatment time resulting from the extended intervals between appointments or poor patient compliance does not necessarily increase the risk of root resorption.5 The more favorable resorption outcomes observed in CAT may be related to the fact that CA are most commonly used in less complex malocclusions, which typically require shorter treatment times and allow for more controlled tooth movements.5, 13 Since root resorption has been reported to be greater in Class II malocclusions than in Class I malocclusions,5, 9 the studies by Liu et al.13 and by Chen et al.31 were excluded from the meta-analysis. Similarly, as teeth with incomplete root development are considered more resistant to resorption,5 the study by Wang et al., which included patients aged 11 years and older, was also excluded.30
In the present meta-analysis, the potential influence of malocclusion type and treatment duration on root resorption was minimized, as the included studies demonstrated statistical comparability for these parameters. To account for anatomical variability and differences in the tooth position within the dental arch, subgroup analyses were performed for individual teeth.
The radiographic assessment of root resorption using 2D imaging techniques is considered less reliable because of image distortion and superimposition. More accurate evaluation can be achieved using CBCT; therefore, studies employing imaging methods other than CBCT were excluded from the analysis.21, 22, 23, 24 Since the assessment of root resorption should ideally be performed after the completion of orthodontic treatment, studies evaluating resorption before the end of treatment were also excluded.24, 34 Additionally, studies were excluded if the type of malocclusion was not specified25 or if only CAT was evaluated without a control group.8, 13, 22, 25
This meta-analysis demonstrated that root resorption in CAT is statistically significantly lower than in FAT when assessed using CBCT imaging. Nevertheless, root resorption was observed in both the CAT and FAT groups across all analyzed studies, indicating that treatment with CA does not eliminate the risk of resorption, but rather significantly reduces its extent. Our findings support the hypothesis that the relatively lower and more intermittent forces generated by CA reduce ischemic pressure within PDL, thereby limiting osteoclast and odontoclast activity.35 Clear aligners apply intermittent forces that activate receptor activator of nuclear factor kappa-B ligand (RANKL) activity through interleukin-1 beta (IL-1β) expression, while minimizing damage to PDL cells.36 The magnitude of orthodontic force is influenced by the elastic modulus of the appliance material. Steel archwires are highly rigid and possess a high elastic modulus, whereas nickel-titanium archwires exhibit substantially lower stiffness. In comparison, aligners demonstrate an elastic modulus approx. 40–50 times lower than that of nickel-titanium archwires.37 Consequently, aligners generate lower orthodontic forces. Higher orthodontic forces may induce ischemia within the periodontal capillaries, contributing to root resorption.22 Fixed appliances typically exert continuous forces of greater magnitude over prolonged periods, potentially intensifying the local inflammatory response and leading to more pronounced root resorption.38, 39, 40 In contrast, the forces applied during CAT are inherently lower, as tooth movement occurs at an average rate of approx. 0.2 mm every 10–14 days as compared to about 1 mm per month during FAT.9
Despite its recognized advantages, CAT remains subject to biomechanical limitations that may restrict its effectiveness in the treatment of complex malocclusions. In particular, CAT has demonstrated reduced predictability in achieving certain types of tooth movement, including significant root torque, bodily translation, extrusion, and the derotation of cylindrical teeth. Unlike FAT, which benefits from the fixed anchorage provided by brackets and archwires, CAT offers less precise control over the application of multidirectional orthodontic forces. As a result, treatment outcomes with CA may be less predictable in more demanding clinical situations. Consequently, cases involving severe crowding, deep bite, anterior open bite, impacted teeth, skeletal discrepancies, or significant transverse deficiencies often require the use of auxiliary devices or hybrid treatment approaches to achieve satisfactory clinical results. Furthermore, CAT in extraction-based treatment should be undertaken with caution, and is generally considered unsuitable for patients with severe skeletal malocclusions or pronounced craniofacial anomalies.41, 42
The design of CA considerably influences the risk of OIIRR. Key factors such as staging protocols, attachment design, aligner thickness, and trimline morphology determine both the magnitude and direction of the forces applied to the teeth. Small incremental movements (0.2–0.3 mm per aligner) generate lighter, intermittent forces, thereby reducing PDL stress and the risk of resorption, whereas accelerated staging protocols may increase apical loading.43 Attachments further modify aligner biomechanics. Optimized attachment design intended to facilitate torque, intrusion and rotational movements may improve movement control, but attachments can also concentrate stress at the root apex, particularly when improperly designed or positioned. For example, horizontal rectangular attachments have been associated with greater root stress than beveled or ellipsoidal forms.44, 45 Trimline morphology also affects force delivery. Straight and extended trimlines enhance aligner retention and improve force transmission, especially during intrusive and torque movements.46 In addition, excessive aligner thickness (>0.95 mm) may increase force magnitude, and consequently elevate the risk of root resorption.47 Therefore, individualized aligner protocols based on digital treatment planning and the careful evaluation of the root-to-bone relationship are essential for minimizing OIIRR and optimizing treatment outcomes.
Another important advantage of CAT is the precise digital pre-programming of tooth movements, which enables clinicians to sequence individual tooth displacements in a controlled and predictable manner. This approach reduces the need for repeated or overlapping movements, and limits undesirable jiggling forces that may exacerbate apical stress. Furthermore, the intermittent force application characteristic of CAT, resulting from regular appliance removal and reinsertion, may facilitate reparative processes within PDL and cementum, thereby contributing to a lower risk of root resorption.44, 45 Moreover, aligners are digitally engineered to optimize force delivery, including force distribution at the root apex, allowing for more biologically compatible orthodontic mechanics that may support the preservation and healing of the root structure during treatment.9, 10, 29
From a clinical perspective, these findings highlight the potential advantages of selecting CAT for patients at increased risk of root resorption, such as individuals with a thin periodontal biotype or a history of dental trauma. The ability to individualize force application and stage tooth movements more gradually may reduce mechanical stress at the root apex and help preserve long-term tooth integrity. Furthermore, digital workflows and 3D treatment planning enable more precise control of force vectors and tooth movement patterns, thereby minimizing undesirable jiggling or uncontrolled tipping forces that may contribute to root resorption.
Our findings are consistent with those of the meta-analysis conducted by Fang et al., who reported significantly lower root resorption in the CAT group (standardized mean difference (SMD): −0.65, 95% CI: −0.74 to −0.55; p < 0.01).9 In contrast to our results, which demonstrated the greatest root loss in the maxillary central incisors, Fang et al. identified the maxillary lateral incisors as the teeth most affected by resorption. Nevertheless, both analyses consistently showed lower levels of resorption in all anterior teeth treated with CAT as compared to FAT. The authors attributed these findings to the intermittent nature of orthodontic forces and the digitally planned, controlled tooth movements characteristic of CAT, which reduce undesirable jiggling effects – mechanisms that are also supported by our interpretation. Conversely, Gandhi et al. reported no statistically significant differences between CAT and FAT in their meta-analysis, except for the right maxillary lateral incisor.4 However, their analysis included studies based on both 2D and 3D imaging modalities, which may have introduced measurement variability. Indeed, their subgroup analysis demonstrated that the root resorption values obtained from 2D imaging were, on average, 0.2 mm greater than those measured using CBCT.4 By including exclusively CBCT-based studies, the present meta-analysis provides a more standardized and accurate assessment of root resorption. In a meta-analysis focusing exclusively on cases treated with CAT, Butsabul et al. reported that the least resorption occurred in the anterior teeth, with the greatest resorption observed in the maxillary central incisors,15 which is consistent with our findings. Collectively, these results highlight the clinical relevance of anatomical variability and imaging methodology in the assessment of root resorption, as well as the importance of using standardized CBCT protocols in future research.
A key strength of this meta-analysis is its explicit focus on patients older than 14 years with fully formed root apices and matched malocclusion severity, thereby reducing a major potential source of bias in comparisons between CAT and FAT.
Limitations
This meta-analysis has several limitations:
– the small number of included studies, which limited the ability to perform robust publication bias analyses, such as the funnel plot assessment;
– the absence of RCTs, as studies evaluating root resorption are predominantly retrospective in design;
– the inclusion of relatively uncomplicated malocclusions, with no assessment of more complex cases;
– the use of linear measurements of root resorption, despite the spatial nature of this phenomenon, whereas volumetric assessment of the lost root structure (e.g., in cubic millimetres) would provide a more accurate evaluation;
– the overall moderate risk of bias among the included studies.
Looking ahead, well-designed RCTs incorporating standardized CBCT imaging, uniform force application protocols and a broader range of outcome measures, including the volumetric assessment of root changes and biomarker analyses, are needed to provide more definitive evidence. In addition, the inclusion of patient-centered outcomes, such as treatment satisfaction, pain and discomfort, and long-term periodontal health, would enable a more comprehensive evaluation of CAT vs. FAT, allowing clinicians to balance potential benefits and risks in a more holistic manner.
Conclusions
This meta-analysis demonstrates that, for comparable malocclusion severity and treatment duration, the use of CA is associated with a statistically significantly lower extent of root resorption in anterior teeth as compared with FA. However, given the small absolute difference in resorption between the treatment modalities, it is not appropriate to stratify or preferentially select CAT based on this parameter alone. Further studies are required to confirm these findings across broader and more diverse populations and treatment contexts.
While both CAT and FAT are capable of achieving effective orthodontic outcomes, the ability of aligners to deliver lighter and more intermittent forces may confer a protective effect on the integrity of the root apex. Accordingly, clinicians may consider CAT particularly in patients presenting with increased risk factors for OIIRR. Future research incorporating standardized imaging protocols and comprehensive biological markers will be essential for refining these observations and further supporting evidence-based orthodontic treatment planning.
Trial registration
The study was registered in The International Prospective Register of Systematic Reviews – PROSPERO (CRD42023471622).
Ethics approval and consent to participate
Not applicable.
Data availability
The datasets supporting the findings of the current study are openly available from https://zenodo.org at doi:10.5281/zenodo.20338555.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.