Abstract
This systematic review and meta-analysis aimed to evaluate the association between periodontitis and rheumatoid arthritis (RA) in middle-aged populations.
The study followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 guidelines. A comprehensive search of major electronic databases was conducted for studies published between 2013 and 2023. In addition, a manual search was performed to identify relevant studies examining an association between these 2 conditions. The Newcastle–Ottawa scale was used to assess the risk of bias for the included cross-sectional and case–control studies. The certainty of evidence was evaluated using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) analysis, and a meta-analysis of eligible studies was conducted.
A total of 11 articles were included in the systematic review, with 9 incorporated into the meta-analysis. A statistically significant positive association was observed between periodontitis and RA for clinical attachment loss (CAL). The GRADE assessment indicated low to moderate level of certainty across studies, indicating strong evidence regarding clinical parameters. The meta-analysis showed a high overall odds ratio (OR) (OR = 11.37; 95% confidence interval (95% CI): 4.22–30.61; p < 0.01), suggesting that patients with RA have a significantly higher risk of developing periodontitis.
In conclusion, this systematic review and meta-analysis identified a positive association between periodontitis and RA. However, the GRADE analysis highlights the need for clinical and longitudinal studies with extended follow-up periods to further clarify this relationship and account for potential confounding factors.
Keywords: periodontitis, meta-analysis, rheumatoid arthritis, rheumatoid factors, GRADE analysis
Introduction
Periodontitis is a chronic inflammatory disease resulting from a bacterial infection that can potentially initiate and increase systemic levels of various cytokines.1 Recent advancements in periodontology have discovered an association between periodontitis and systemic diseases such as diabetes, myocardial infarction, stroke, arteriosclerosis, Alzheimer’s disease, osteoporosis, and rheumatoid arthritis (RA) in adults.
Rheumatoid arthritis and periodontitis are chronic inflammatory conditions that share similar inflammatory mediators, including interleukin (IL)-1β, IL-6 and tumor necrosis factor-alpha (TNF-α).2 Moreover, both diseases are known to impact connective tissue degradation. Rheumatoid arthritis is a systemic autoimmune condition characterized by persistent joint inflammation, resulting in joint destruction and functional loss. Studies have reported that globally, around 1.0% of adults suffer from this condition, with a higher predisposition observed in females (male:female ratio of 1:3). In the United States, around 2% of adults suffer from RA.3, 4, 5 Studies have suggested 3 types of disease manifestation among RA patients: self-limited – patients with self-diagnosed RA who do not have symptoms 2–3 years after diagnosis6; easily controlled – conditions managed with non-steroidal anti-inflammatory drugs (NSAIDs)7; and progressive – conditions that typically require second-line therapy and may not fully resolve despite treatment.8
Numerous hypotheses have been developed regarding the correlation between periodontitis and systemic diseases. An intriguing one centers around paraoxonase-1 (PON1), an enzyme with established antiatherogenic and antioxidant activities. Current research investigates the potential role of PON1 in mitigating both dental biofilm formation and periodontitis.9 Many studies have investigated the association between periodontitis and RA.10, 11, 12 While some studies have indicated that periodontitis could be a potential risk factor for RA, others have demonstrated a notable increase in tooth and alveolar bone loss in individuals with longstanding RA.1, 13, 14, 15 Patients diagnosed with periodontitis exhibit a four-fold increase in the likelihood of self-reported RA, which may be related to the beneficial outcomes of non-surgical periodontal therapy (NSPT) in reducing the severity of RA.2, 16, 17 In RA, the synovial membrane produces proinflammatory mediators due to systemic immunological failure, leading to synovitis, joint pain and bone damage.18, 19 The correlation between RA and periodontitis may be attributed to the association of both conditions with environmental and genetic risk factors, as well as comparable pathobiology.
Periodontitis and RA are characterized by chronic inflammation that leads to increased infiltration of lymphocytes of the T and B cell types, neutrophils, and monocytes.8, 12 The elevated production of proinflammatory cytokines leads to the destruction of joint and alveolar bone tissues in RA and periodontitis, respectively.1, 14 Fibroblasts and lymphocytes increase the expression of receptor activator of nuclear factor-κB ligand (RANKL) during osteoclast formation in both conditions. Autoimmunity to citrullinated proteins has been suggested to contribute to the relationship between RA and inflammation.20 Porphyromonas gingivalis is a significant periodontopathogen found in the subgingival plaque. It demonstrates the distinctive capability of citrullinating proteins, thereby accelerating the autoimmune response in RA.21, 22
Both conditions share a common etiology, pathology, immunogenetic background, and pathways of bone cartilage destruction. Additionally, RA and severe periodontal disease are associated with lower oral health-related quality of life (OHRQoL) scores.23 Various studies have also proposed NSPT for these conditions.16, 18, 19 This may be evidenced by the ability of NSPT to reduce disease activity score-28 with C-reactive protein (DAS28-CRP), erythrocyte sedimentation rate (ESR) and anticitrullinated protein antibody (ACPA) levels in serum.24 Nonetheless, very limited literature shows this bidirectional association, especially in middle-aged adults. The National Health and Nutrition Examination Survey-I (NHANES-I) showed that individuals with periodontitis or missing teeth presented increased odds of prevalent or incident RA.25 However, most of the results were not statistically significant and lacked dose–response relationships. The observed variations may stem from inconsistent criteria for defining the 2 illnesses. The association between these 2 conditions can be explained in various forms: 1) the role of periodontal pathogens (P. gingivalis, anticyclic citrullinated peptide (anti-CCP)); 2) common immunogenetics; 3) common risk factors (smoking, age-related factors, psychological issues).1, 12, 13, 26
Several studies have reported discrepancies regarding the correlation between periodontitis and RA. However, recent reports indicate a significant link (biological and immunological) between these prevalent chronic inflammatory conditions.8, 11, 15 Nonetheless, a potential correlation between the severity of RA and periodontitis cannot be established due to inconclusive evidence. Hence, this systematic review aims to evaluate an association between periodontitis and RA among middle-aged populations.
Material and methods
Focus question
Based on the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines 2020, a specific question was structured according to the PECOS (Participants, Exposure, Control, Outcomes, and Study design) framework. The focus question for this systematic review was as follows: Among middle-aged populations (P), is there an association between periodontitis (E) and rheumatoid arthritis (O), compared to healthy individuals (C), in observational studies (S)?
Protocol and registration
The research problem, focus question and criteria for inclusion and exclusion were identified after a preliminary literature review. A protocol was prepared and registered prospectively with PROSPERO (registration No. CRD42023490679).
Eligibility criteria
Studies fulfilling the following criteria were included: participants aged ≥30 years; observational studies; studies reporting risk estimates as odds ratios (ORs) or hazard ratios (HRs) with corresponding 95% confidence intervals (95% CIs) for the association between RA and periodontitis; inclusion of a control group (healthy individuals); diagnosis of periodontitis and RA according to accepted diagnostic criteria; adjustment for potential confounding factors; studies with ≥15 patients per group; mean RA duration of ≥5 years; articles published between 2013 and 2023.
The exclusion criteria were as follows: letters to the editor; commentaries; reviews; case reports; case series; animal studies; in vitro studies; and articles published in languages other than English. If more than 1 paper from the same study was retrieved, both were included when different outcomes were reported. However, if the same result was reported in different studies, the one with the larger sample size and/or non-overlapping cohort analyses was selected for the meta-analysis.
Literature search protocol
The search strategy included published and unpublished articles, and this review employed a two-step procedure for selecting studies. An initial search of PubMed®/MEDLINE was conducted, followed by screening of titles, abstracts and keywords.
The second search utilized keywords and index terms across different databases. PubMed®/MEDLINE, Embase, Scopus, Web of Science, and ProQuest were searched from 2013 to 2023 using various combinations of keywords and Medical Subject Headings (MeSH) terms related to periodontitis and RA. Unpublished articles were searched in the OpenGrey database. Moreover, a manual search and citation chasing were performed in various dental and medical journals. The PubMed® search strategy is available from the corresponding author upon reasonable request.
Selection of articles
The retrieved articles were imported into EndNote 20 (Clarivate, Philadelphia, USA), and duplicates were removed. The relevant articles were entered into a Microsoft Excel (Microsoft Corp., Redmond, USA) sheet, and the final articles were selected by 2 independent reviewers (SeA, BJ), who examined the titles, abstracts and full texts according to the eligibility criteria. Disagreements between the reviewers were resolved through discussion with a third reviewer (SuA). Intraobserver reliability was assessed, and the value of K-alpha between the reviewers was 0.9.
Data extraction
The data was extracted using tools predesigned for research questions. The following details were extracted: 1) authors/year/country; 2) number of males and females included in the test and control groups; 3) mean age of participants; 4) exposure assessment of periodontitis; 5) outcome assessment of RA; 6) RA clinical parameters; 7) periodontal clinical measures; 8) risk estimates (crude and adjusted): ORs, relative risks and HRs with 95% CIs and p-values, if available; 9) number of RA patients with a history of periodontitis; 10) factors adjusted for in the analysis, e.g., age, smoking status and other inflammatory conditions; and 11) conclusions. The reviewers resolved discrepancies through discussion, and the authors were contacted if any data from the primary study was missing.
Assessment of methodological quality
The methodological quality of the included articles was assessed using the Newcastle–Ottawa quality assessment scale for case–control27 and cross-sectional studies.28 A scoring system was used to evaluate the quality of articles, with 17–18 points indicating high, 12–16 indicating moderate, and <12 suggesting low quality. Eligible studies were assessed for quality by 2 reviewers, and any disagreements were resolved through discussion or by the third reviewer.
Data synthesis and assessment of the quality of evidence
A meta-analysis of the included case–control and cross-sectional articles was conducted, as the included studies possessed similar designs, and the pooling of statistical data yielded a concise outcome. Moreover, the quality of evidence was assessed using the GRADE (Grading of Recommendations Assessment, Development and Evaluation) system.29
Results
Study selection
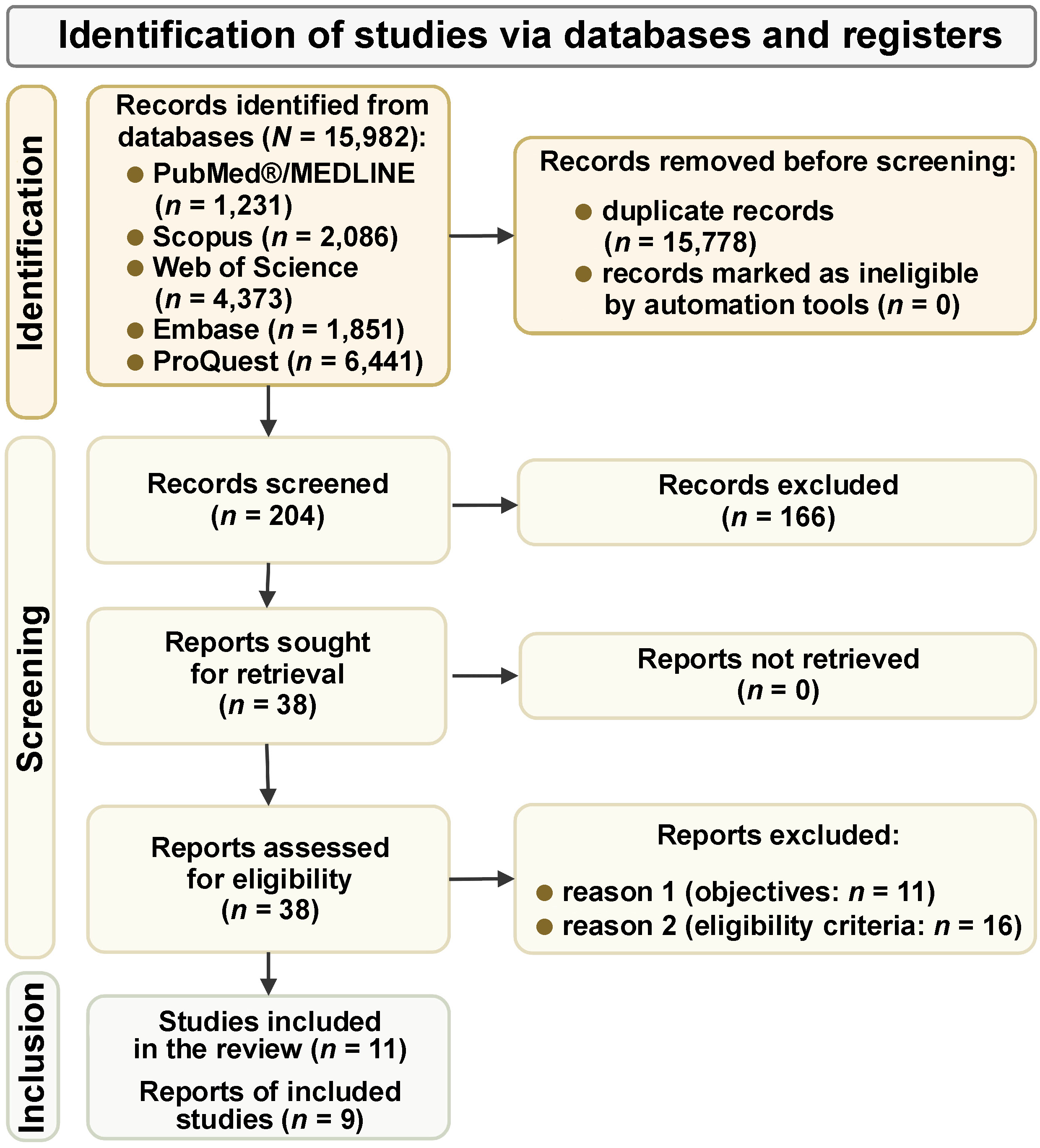
The primary search identified 15,982 relevant articles, out of which 15,778 papers were found to be duplicates and were removed. The titles and abstracts of the remaining 204 articles were screened based on the eligibility criteria, and 166 were excluded after careful evaluation. The full texts of the remaining 38 articles were examined, and 27 articles were removed based on their objectives or eligibility criteria. Finally, 11 articles were considered eligible for this systematic review. Figure 1 illustrates the study selection process.
Characteristics of the included studies
This review included 11 primary studies, consisting of 5 case–control and 6 cross-sectional studies comprising 4,055 participants (1,396 males and 2,659 females) (Table 1). The included papers were published between 2013 and 2023 and, originating from different countries (India, USA, China, South Korea, Sweden, Spain, Brazil, and Lithuania), represented various ethnic backgrounds. In most of the included studies, the majority of the participants were females aged ≥40 years. Out of the 11 studies, only 2 studies excluded smokers,11, 30 and 1 study did not mention this criterion.17 Only 5 included studies reported medications used by the patients.17, 31, 32, 33, 34 Most of the studies evaluated periodontal health using validated indices, and RA was diagnosed based on the 1987 (revised) American Rheumatism Association (ARA) criteria and 2010 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) criteria for RA.
Clinical parameters defining periodontitis
Ten of the 11 included studies evaluated CAL,11, 12, 17, 30, 31, 33, 34, 35, 36, 37 either alone or in combination with other periodontal indices; 1 study did not assess CAL and recorded only PPD and BOP.32 Five studies evaluated PPD and BOP in combination with CAL.11, 12, 30, 34, 35 The odds of developing periodontitis were higher in patients with RA. However, no significant differences were reported regarding the severity of periodontitis in relation to RA. Secondary parameters recorded included the plaque index, the gingival index, tooth loss, and tooth mobility. Only 5 studies evaluated interexaminer calibration reports.12, 30, 32, 34, 35
Clinical parameters defining rheumatoid arthritis
All the included articles diagnosed RA clinically based on the DAS28 criteria as low, moderate or high. Eight papers reported RA treatment, while others did not mention the therapy. Disease duration was evaluated as a factor associated with the outcome in 6 publications, whereas 5 did not assess disease incidence. Eight studies examined ESR and posterior-anterior hand and wrist radiographs,17, 30, 31, 32, 33, 35, 36, 37 4 reports assessed visual analog scores and tender joint counts to measure the occurrence of RA,12, 30, 34, 35 and 5 studies recorded the CRP levels.12, 30, 34, 35, 36 All the included papers utilized validated measures to record RA clinical parameters.
Association between rheumatoid arthritis and periodontitis
Case–control studies
Moura et al. reported a high frequency of periodontitis among individuals with high DAS28 scores (adjusted odds ratio (aOR): 3.12; 95% CI: 1.47–4.26).36 Additionally, a significant correlation between periodontitis, RA and smoking was noted (p < 0.01).36 Adjusted risk estimates considered older age, female sex, smoking, and the protective effect of alcohol use. Renvert et al. found that high DAS28-ESR was linked to a composite index for periodontitis (OR: 2.5; 95% CI: 1.5–4.2; p < 0.001).32 Rodríguez-Lozano et al. demonstrated that the DAS28-ESR and DAS28-CRP scores were significantly associated with periodontal clinical measures (aOR: 20.57; 95% CI: 6.02–70.27; p < 0.001) when adjusted for sex, smoking status, socioeconomic status, annual dental prophylaxis, and osteoporosis.33 Zhao et al. also found DAS28-ESR outcomes to be associated with periodontal clinical measures, revealing significant results (aOR: 10.26; 95% CI: 4.67–22.58).17 Similarly, Joseph et al. found that the DAS28-ESR scores were correlated with CAL, with a relatively significant OR when smokers were excluded.30
Cross-sectional studies
Posada-López et al. reported that periodontitis was not associated with RA.37 This study adjusted for confounders such as sex, age, P. gingivalis, diabetes, smoking, osteoporosis, NSAIDs, corticosteroids, and antihypertensive medication. All periodontal variables and P. gingivalis were negatively correlated with RA biochemical markers (p < 0.05). However, Punceviciene et al. reported a high prevalence of severe periodontitis in RA patients.31 This relationship was significantly associated with higher RA disease activity and lower vitamin D levels in the RA–periodontitis group.31 Similarly, Eriksson et al. found that RA parameters correlated with periodontal clinical measures in a study that included non-smokers.12 Kim et al. reported that DAS28 outcomes were associated with CAL in a cohort that included individuals who smoked.35 Furthermore, Choi et al. noted that DAS28-ESR outcomes were correlated with CAL and significantly elevated ORs.34 Dev et al. also documented that the American Rheumatism Association (ARA) 1988 criteria were associated with periodontal clinical measures in a study in non-smokers, where periodontitis was evaluated using the community periodontal index (CPI) and CAL was assessed based on the World Health Organization (WHO) guidelines.11
To summarize, the increased risk of periodontitis was observed in RA patients in 10 studies, and 1 study showed no correlation between the 2 conditions.37 Additionally, 10 studies demonstrated an association between moderate to severe forms of periodontitis in RA patients. Six papers mentioned smoking, vitamin D deficiency and alcohol consumption as risk factors associated with periodontal health and RA.17, 32, 33, 35, 36, 37 Three studies demonstrated anti-P. gingivalis antibody titers and reported a positive association with CAL, PPD and BOP in patients with RA.12, 30, 35 One study noted a significantly higher risk of periodontitis (p = 0.01) among obese females with RA.36 However, 1 report showed no association between the severity of periodontitis in RA patients.37 Table 1 and Table 2 illustrate the relevant findings of the included studies.
Risk of bias analysis
The Newcastle–Ottawa scale was employed to evaluate the risk of bias in the included case–control (Table 3) and cross-sectional studies (Table 4), analyzing case selection, comparison and outcome criteria. Out of the 5 case–control studies, the case and control selection domains scored low, while the comparison and outcome domains achieved higher scores. Accordingly, 1 study was identified as having a high risk of bias,32 and 4 studies had a low risk of bias.17, 30, 33, 36 Similarly, in cross-sectional studies, one study was of poor quality,11 2 were of moderate quality,34, 37 and 3 studies were classified as having a low risk of bias.12, 31, 35
GRADE evaluation
The GRADE analysis reported low certainty of evidence in the analyzed case–control studies on the association between periodontitis and RA (Table 5). Meanwhile, cross-sectional studies demonstrated moderate certainty of evidence. The findings of the GRADE analysis indicate that more clinical and longitudinal studies are required to establish an association between both conditions.
Meta-analysis results
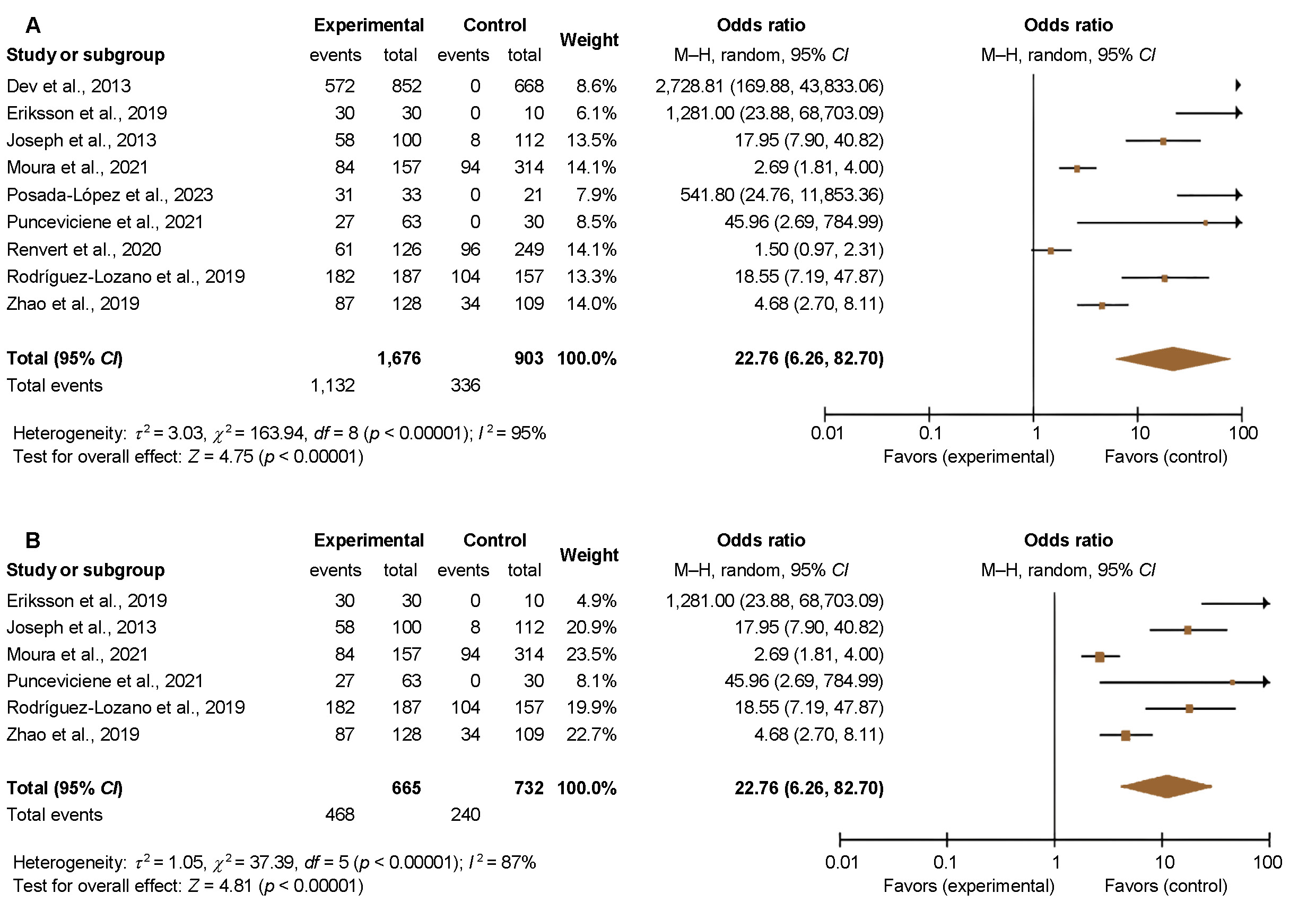
The results of the meta-analysis revealed high heterogeneity among the included studies (I2 = 95%), and a high overall OR between the groups (OR = 22.76, 95% CI: 6.26–82.70; p < 0.001) (Figure 2A). Sensitivity analysis of the included studies also showed a high OR for the development of periodontitis in RA patients (OR = 11.37, 95% CI: 4.22–30.61) (Figure 2B). Figure 3A represents the overall analysis of cross-sectional studies, which revealed high heterogeneity (I2 = 91%). The overall OR between the groups was 5.34 (95% CI: 2.28–12.51), which was statistically significant (p < 0.001). Overall, sensitivity analysis of the included cross-sectional studies yielded an OR of 7.52 (95% CI: 2.95–19.14), demonstrating a 3 times higher risk of developing periodontitis in patients with RA (Figure 3B). In the context of the 5 studies that were considered in this analysis, only 1 study37 concluded that the effect in question was not significant. The subgroup analysis was not performed, as the authors’ primary focus was on assessing the overall association.
Discussion
To the best of our knowledge, this is the first systematic review to critically analyze and synthesize the available literature on the association between periodontal disease and RA. The results of this study indicate a statistically significant positive association between periodontal disease and RA. According to the results of the meta-analysis, there is an 11.37-fold higher risk of developing periodontitis in patients with RA. However, the GRADE analysis reported low to moderate certainty of evidence, suggesting that more research is needed on this association.
Previous studies have systematically evaluated the association between periodontitis and RA.1, 10, 11, 38, 39 Based on the selection criteria, 11 articles (5 case–control and 6 cross-sectional studies) were included in this systematic review, with 9 articles being incorporated into the meta-analysis. The studies showed a positive association between periodontitis and RA, as 10 out of 11 papers demonstrated a strong correlation. The meta-analysis of cross-sectional studies revealed similar findings. A systematic review and meta-analysis by Kaur et al. showed a significant association between the conditions in 17 out of 19 studies (examining various RA-related factors and periodontitis).40 Another systematic review conducted by Kriauciunas et al. found a link between oral bacterial growth and RA.41 Agnihotri and Gaur reported significantly more severe CAL in their systematic review of elderly patients with RA.42 In a recent scoping review, Nik-Azis et al. found that seropositive RA patients had higher odds of developing chronic periodontitis than the control group.43
The meta-analysis of cross-sectional studies indicated that there is a 5-fold increased risk for RA in patients with moderate to severe periodontitis (95% CI: 2.28–12.35; p = 0.01). The results also indicate that an inverse relationship may exist between the risk ratio of RA and periodontitis. The results of this review support the relationship between these 2 variables. However, given the small number of point estimates available in this analysis, there was a lack of statistical significance rather than an absence of an association. Similarly, in their meta-analysis, Del Rei Daltro Rosa et al.reported a reduction in the RA score index (mean difference = −1.81) in patients treated for periodontitis.44 The risk estimate was lower than that reported in the current study. In the present review, we considered the studies included in the paper of Del Rei Daltro Rosa et al., although some of them could not be quantitatively synthesized. Moreover, the mentioned review included prospective and cross-sectional studies, whereas the current review focused primarily on cross-sectional evidence.
Rheumatoid arthritis is a risk factor for periodontal disease.40 This relationship can be attributed to a possible link between systemic and concurrent alveolar bone resorption in RA and periodontitis. As systemic bone mineral density declines, for instance in RA, a simultaneous decrease occurs in the density of the maxillary and mandibular arches.43 This increases bone fragility, inflammation and fracture risk. The majority of studies conducted on middle-aged adults have shown a positive association between RA and periodontal disease, which could be attributed to estrogen-related bone remodeling that increases with age.42 Additionally, estrogen deficiency plays a mediating role in this association, contributing to inflammation and increasing the risk of both periodontitis and RA.12, 44
The clinical presentation of periodontitis may not accurately indicate the presence of P. gingivalis, as not all cases are associated with this bacterium. In some instances, the administration of antibiotics in conjunction with mechanical debridement does not result in substantial improvement for the treatment of chronic periodontitis.45 The presence of various periodontal pathogens, such as Aggregatibacter actinomycetemcomitans, highlights the need for improved study designs that consider the specific bacteria present in the subgingival microbiota.20, 26, 39, 46 Using an objective measurement of periodontal disease, such as quantifying the percentage of inflamed or ulcerated surface area, would address the issue of inconsistent definitions of periodontitis.15, 47, 48
Despite promising results, heterogeneity was observed among the included studies regarding the prevalence and severity of periodontal disease in RA-positive patients. In a cohort study of US veterans, periodontitis patients with RA were associated with the presence of ACPAs.49 However, no significant association was found between periodontal disease, ACPA-positive RA patients and healthy controls.50 In a Korean study, the authors indicated a positive association between periodontal inflammation and ACPA levels.35 In a Japanese population cohort study designed to investigate this association, increased periodontal inflammation was reported in patients with seropositive RA as the level of ACPA rose above 2.34.51, 52 Choi et al. reported increased ACPA levels in patients with severe periodontitis.34 By contrast, 2 studies on cohorts from Sweden and Malaysia found no association between ACPA levels and periodontal health in RA patients.39, 50
The fundamental involvement of periodontal disease with the presence of salivary biomarkers is the basis for the hypothesized relationship between periodontitis and RA. Similar relationships have been studied using novel salivary adipokine levels (e.g., omentin-1). These molecules have the potential to serve as diagnostic tools to assess the progression of periodontal disease and treatment effectiveness.53 However, the epidemiological evidence supporting this association is currently equivocal. These conflicts could be attributed to differences in study design and the selection of comparison groups (healthy controls, osteoporosis, osteoarthritis patients). Most of the included studies investigating this relationship did not specify the type and subsets of RA, even though these are important criteria for establishing an association between both conditions. The need for more specific and standardized criteria for defining periodontal disease and RA, inadequate information on confounding factors, and differences in eligibility criteria can also contribute to the conflicting evidence. Three included studies used data from hospital-based registries, while 2 studies employed national registries as the sample population. Such data provides concrete results due to larger sample sizes but may lack detailed information on confounding factors and associated diseases.
Limitations
The validity of the meta-analysis reported in this review is contingent upon the strength of the association between the 2 conditions – periodontitis and RA. Some studies have noted statistically significant associations between these 2 conditions, while others showed no significant correlations. Including such studies in our meta-analysis increases the validity of the findings and provides a more robust estimate of the association. However, the results of the meta-analysis should be interpreted carefully, as the inclusion of observational studies increases the risk of bias. The studies included in our review varied in methodological quality, resulting in differences in the strength of evidence. Well-controlled, population-based and clinical (molecular epidemiology) studies are needed to confirm the immunological and biological links between RA and periodontal disease. Future studies on this topic should follow the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines to facilitate the assessment of study strengths and limitations, as well as the generalizability of findings. Secondly, the review did not specifically consider severe periodontitis, as it is challenging to recruit patients with this condition. The majority of the included studies used convenience sampling methods, which pose a high risk of bias. Furthermore, although sex, age, smoking status, and RA treatment were considered in many studies, these parameters were not reported in detail. Hence, it was challenging to draw definitive conclusions on the role of potential confounding factors.
Conclusions
The current systematic review and meta-analysis found a positive association between periodontitis and RA. Moreover, some studies reported that patients diagnosed with RA present higher levels of salivary biomarkers and microbial load than healthy controls. The results of the GRADE analysis indicate the need for longitudinal clinical studies with longer follow-up durations to comprehensively evaluate this association and elucidate the potential role of confounding factors. Overall, the findings indicate that individuals diagnosed with RA demonstrate an increased risk of developing periodontal disease when compared to the general population. However, significant heterogeneity was observed across the included studies with respect to study populations, definitions of periodontal disease and RA assessments. Further research using standardized disease criteria and measurements is warranted. Understanding the interrelationship between periodontitis and RA may facilitate the identification of shared risk factors and disease mechanisms. Ultimately, clarifying this association has implications for the early identification of at-risk patients, preventive strategies and integrated treatment approaches that bridge oral health and chronic inflammatory disease management. The results of this review must be interpreted with caution, given the high heterogeneity among the included studies. Further research is necessary to clarify the extent and underlying nature of the periodontitis–RA relationship, as suggested by this initial evidence synthesis.
Ethics approval and consent to participate
Not applicable.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.