Abstract
Background. The current treatment for patients with myalgia comprises splint therapy (ST), cognitive-behavioral therapy (CBT), psychological treatment, and education.
Objectives. The aim of the present study was to compare the effectiveness of relax-psycho-breathing therapy (RPB) and ST in women with myalgia, and to evaluate the efficacy of occlusal splint and/or behavioral therapy in the management of muscle pain.
Material and methods. The study, designed as a randomized controlled trial (RCT), involved 105 women aged 25–55 years with pain in the masticatory muscles during the 30 days prior to examination. Myalgia was diagnosed according to the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) Axis I. The clinical examination assessed muscle and temporomandibular joint (TMJ) pain intensity, TMJ sounds, maximum mouth opening (MMO), and deviation in mouth opening and mandibular movement. After an initial assessment, at the 2nd visit (V2), the 25 patients from the 1st group were introduced to RPB: relaxation techniques; breathing patterns; psychological-behavioral instruction; muscle exercise therapy; puffing therapy; and self-massage. The 2nd group of patients received a custom-made, thermoplastic, flat-plane relaxation splint placed on the mandible. The efficacy of treatment in all subjects was evaluated at 2 follow-up visits (V3 and V4).
Results. In cases of muscle pain, pain during function, TMJ and muscle tenderness, and headache attributed to TMD, a statistically significant difference between the RPB and ST groups was observed only at the final follow-up visit. No significant differences between the 2 groups were found for MMO.
Conclusions. The reduction in myalgia following treatment suggests that both RPB exercises and ST are equally effective. However, considering the cost and duration of myalgia therapy, comprehensive care incorporating relaxation techniques may be a preferable first-line approach rather than ST alone.
Keywords: temporomandibular disorders, myalgia, behavioral therapy, splint
Introduction
Masticatory myalgia is the primary source of chronic non-odontogenic orofacial pain, frequently observed in dental practice. The prevalence of temporomandibular disorders (TMD) has been estimated to be 31% for adults and 11% for children and adolescencents.1 About 60–70% of the human population has experienced at least one TMD symptom in their lifetime, but only 5% of cases have been treated.2 In the Polish population, myalgia has been reported to occur in 47.4% of patients, while myofascial pain occurs in 14.1% of patients (in accordance with the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) protocol).3, 4
These problems commonly occur between the age of 27.5 and 50 years, with a predominance in females, and particularly in sedentary individuals.3, 4 Masticatory myalgia originates in the masticatory muscles, and in some cases results in limited mandibular movement.3, 5 The diagnoses of muscle pain are classified into 4 subclasses: myalgia; tendonitis; myositis; and spasm. Within the DC/TMD classification (Axis I), myalgia is subdivided into 3 categories (sub-diagnoses): local myalgia; myofascial pain (with “spreading” pain being its hallmark clinical manifestation); and myofascial pain with referral.6, 7, 8
The etiology of myalgia is multifactorial; the condition may result from trauma, repetitive micro-traumas due to parafunctional habits (PHs), as well as psychological factors (stress, anxiety, tension).6, 8, 9, 10 Patients with myalgia may present with one or more clinical complaints, including pain during the movement of the temporomandibular joint (TMJ), pain in the pre-auricular area and/or the masticatory muscles, and limited and/or deviated mandibular movement. Somatic symptoms that impair function are common and often lead to disability, complicating treatment outcomes and increasing the need for more costly therapeutic interventions.11, 12 It has been noted that patients with myofascial pain are more likely to experience changes in the breathing parameters, as well as fatigue, depression and sleep disruptions.13, 14
The primary goals in the management of masticatory myalgia are to reduce or eliminate pain, increase mouth opening, and improve the overall quality of life (QoL). Therapy should include patient education delivered with understanding and empathy.15 The most widely accepted approaches to managing myalgia and PHs include behavioral interventions, pharmacological treatment, physical therapy, occlusal appliances, and botulinum toxin injections.16, 17, 18
Self-management is widely regarded as a core component in the treatment of TMD and myalgia.19, 20, 21 This typically involves elements of cognitive-behavioral therapy (CBT) combined with patient education, relaxation techniques, the reinforcement of adaptive behaviors, and the reduction of maladaptive habits, alongside home-based physical therapy. The CBT approach has been extensively studied and shown to be effective in the treatment of depression, anxiety, low self-esteem, eating disorders, and other psychological conditions.21, 22, 23
Occlusal splints are among the most commonly used therapeutic approaches for patients diagnosed with myalgia. They promote occlusal disengagement, help restore the vertical dimension of occlusion, facilitate muscle relaxation, reduce joint loading, and may aid in TMJ repositioning.24
There is no clear consensus regarding clinical indications for occlusal splints and their function. Türp et al. reported no significant differences in symptom reduction between the splints placed on the maxilla and those placed on the mandible.25 In patients with myalgia, splints should be used intermittently, primarily during nocturnal wear, provided that PHs are adequately controlled during the day. Their use should generally be limited to a few months, as prolonged wear may lead to patient habituation and the development of undesirable dependence on the appliance.26
The present study compares the effectiveness of relax-psycho-breathing therapy (RPB) and splint therapy (ST) in women with myalgia, aiming to assess the clinical value of occlusal splints and/or behavioral therapy in the management of muscle pain. It also evaluates the relative efficacy of both approaches in reducing myalgia and seeks to identify the most appropriate treatment sequence for optimal outcomes.
The null hypothesis of this study is that relax-psycho-breathing therapy (RPB) and splint therapy (ST) are equally effective in women with muscle pain.
Material and methods
The study was conducted at Poznan University of Medical Sciences, Poland, between 2016 and 2022. Approval from the Institutional Ethics Committee (No. 551/15), as well as written informed consent from all patients were obtained. This study was designed as a randomized controlled trial (RCT).
Study design, inclusion and exclusion criteria
The study involved 105 patients seeking treatment due to orofacial pain.
The inclusion criteria were as follows:
– pain in the masticatory muscles scored ≥3 on a numerical rating scale (NRS) of 0–10 points, present during the 30 days prior to selection; myalgia was diagnosed according to the DC/TMD Axis I;
– other pain conditions, such as pain involving the arm, shoulder and upper back;
– jaw movement disorders with regard to TMJ, e.g., limited and/or deviated mandibular movement;
– eye symptoms of TMD – lacrimation, pain behind the eyes; and
– ear symptoms of TMD – otalgia, tinnitus, vertigo, aural fullness, itching in the ear, subjective hearing impairment.
The exclusion criteria were as follows:
– denture (fixed or removable) wearers;
– patients with arthralgia and/or disc displacement;
– patients with an open bite, a cross-bite, a prognathic relationship, and with pain of dental origin;
– patients with systemic diseases (e.g., rheumatic diseases or degenerative joint disease), serious neurological disorders, cervical spine injuries or postural deformities, the presence of drug abuse, a comorbid malignant disease, psychiatric diseases;
– patients taking medications for neurological problems or medications that could affect equilibrium or cause visual impairment; and
– patients with earlier ST or a masticatory organ injury.
On the 1st day of the study (visit 1 – V1), all patients completed a questionnaire and were subjected to a clinical examination. The questionnaire consisted of several parts: (1) personal details, including age and sex; (2) general health; (3) history of trauma; (4) pain evaluation – the patients were asked to rate their regional pain intensity from 0 to 10 (NRS), with regard to both current pain and maximal pain during the past 6 months; moreover, the presence of pain in other parts of the body (the arm, shoulder and upper back) was reported (yes/no); (5) history of ear-related symptoms – otalgia, tinnitus, vertigo, aural fullness, itching in the ear, subjective hearing impairment; (6) history of eye-related symptoms – lacrimation, pain behind the eyes; (7) the occurrence of physical symptoms of TMD (DC/TMD Axis II – Patient Health Questionnaire-15 (PHQ-15)); (8) the occurrence of depression (DC/TMD Axis II – PHQ-4, PHQ-9, Generalized Anxiety Disorder-7 (GAD-7)); (9) history of headaches during the past 30 days, including the temple areas of the head (DC/TMD Axis II); and (10) PHs (DC/TMD Axis II – Oral Behavior Checklist).
Data collection
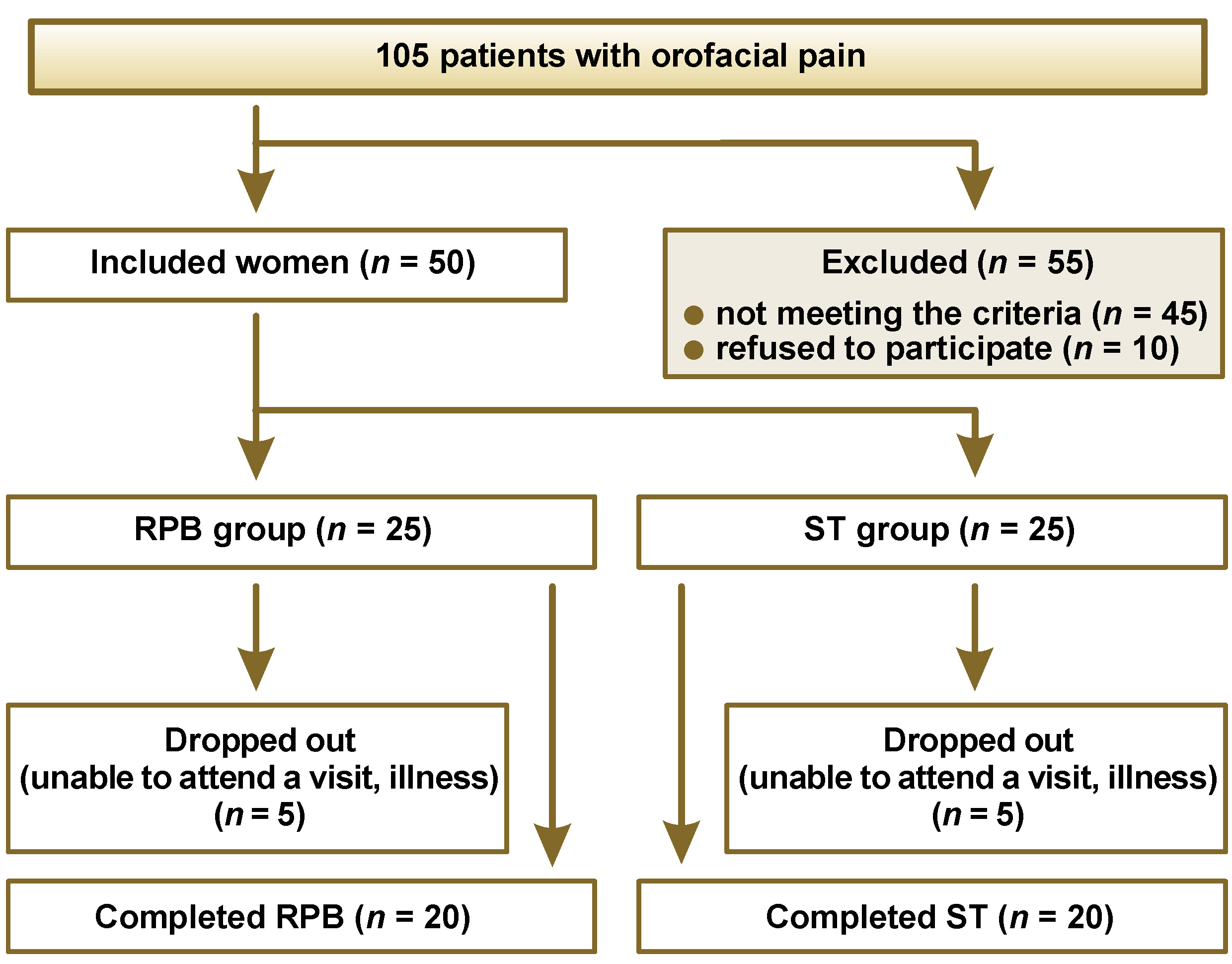
In total, 105 patients with orofacial pain were recruited, from which 55 were excluded for the following reasons: not meeting the criteria (after completing the questionnaire and/or after the clinical examination) (n = 45); refusing to participate (n = 10). The included patients (50 women, aged 25–55 years) were randomly assigned either to the RPB group (n = 25) or the ST group (n = 25). From each group, 5 patients dropped out due to illness or failure to attend a visit. Finally, 20 patients in each group completed the therapy (Figure 1). The patient demographics were recorded.
Clinical examination
The clinical examination focused on the following data: (1) muscle and TMJ pain intensity; (2) TMJ sounds; (3) maximum mouth opening (MMO); (4) mouth opening limitation/deviation; and (5) deviation in mandibular movement (lateral (right and left) and protrusive).
Maximum mouth opening and opening deviation
Maximum mouth opening was measured from the incisal edge of the maxillary central incisors to the incisal edge of the mandibular central incisors at the midline, and did not include the degree of overlap between the teeth.27 The patient was instructed to slowly open their mouth 3 times to allow the visualization of mandibular end-range movement in the frontal plane. Moreover, the presence of deviation during mouth opening, defined as the displacement of the mandible at least 2 mm to the right or left of an imaginary vertical line, was evaluated.
Pain intensity
Jaw muscle pain and tenderness were assessed using an 11-point numerical rating scale (NRS-11). The NRS-11 is a widely used measure of pain intensity in both research and clinical practice.28 The participants were asked to select a single number that best represented their pain intensity on a scale from 0 (“no pain”) to 10 (“worst possible pain”).
The Graded Chronic Pain Scale (GCPS), included in the Axis II screening instruments of the DC/TMD protocol,6 comprises 6 items assessing facial pain experienced over the past 3–6 months. Each item is rated on a scale from 0 to 10.
Moreover, pain intensity during the clinical examination was assessed using the DC/TMD Axis I protocol.6, 7, 29 The examination included standardized palpation of the masticatory muscles (masseter, temporalis, lateral pterygoid, and medial pterygoid) and TMJ, using the index and middle fingers.
Physical symptoms (DC/TMD Axis II – PHQ-15)
Physical symptoms were assessed using the DC/TMD Axis II – PHQ-15. Axis II, which addresses psychosocial and behavioral dimensions, comprises instruments for the evaluation of pain intensity, pain-related disability, the functional limitations of the masticatory system, oral parafunctional behaviors, as well as symptoms of depression and anxiety, and the extent of multiple somatic symptoms throughout the body.
The physical symptoms reflecting somatic complaints (“somatization”) were assessed using a series of psychoanalytic questions (e.g., the presence of chest pain, palpitations, dizziness, or sleep disturbances), with responses recorded as yes/no.
Occurrence of depressive symptoms (DC/TMD Axis II – PHQ-4, PHQ-9, GAD-7)
The occurrence of depressive symptoms was assessed using the following question: “During the past month, have you experienced decreased energy or slowing down, feelings of loneliness or sadness, or indifference?”
Occurrence of parafunctional habits (DC/TMD Axis II – Oral Behavior Checklist)
The occurrence of PHs was assessed using the following questions: “Do you clench or grind your teeth during the day?”; “Do you clench or grind your teeth during sleep, based on any information available to you?”; “Do you bite your fingernails, fingers, pens, pencils, hair, or other objects?”; and “Do you use chewing gum?”
Treatment protocol
The diagnostic impressions of the maxilla and mandible were performed on day 1 (enrollment, V1). The patients were then randomly assigned, using a computer algorithm, to one of the study groups – the RPB group (relax-psycho-breathing therapy) or the ST group (splint therapy). Treatment commenced at the 2nd visit (V2; day 7). The RPB intervention included relaxation (R), self-care techniques (M), psychological and behavioral therapy (P), and breathing exercises (B).30, 31, 32 In the ST group, in addition to the splint, the patients received basic educational and self-care instructions. Treatment outcomes were assessed at the 3rd and 4th follow-up visits (V3 and V4; day 21 and day 49, respectively). In patients with a limitation in mouth opening (<40 mm), the post-treatment deviation in mandibular movement was evaluated, along with the level of muscle pain.
RPB group – relax-psycho-breathing therapy
During V2, 25 patients were instructed to participate in RPB, with care taken to avoid pain or discomfort. The intervention included relaxation techniques, breathing exercises, psychological-behavioral guidance, muscle exercise therapy, puffing therapy, and self-massage (Figure 2).
– Relaxation techniques: Performed at least twice daily for 10 min. The patients were instructed to lie in a supine position, and sequentially tense and relax the designated muscle groups, starting from the head and progressing toward the feet.
– Breathing patterns: Performed 3 times daily for 3–5 min. The patients were instructed to sit comfortably, focus on slow, deep inhalation through the nose and exhalation through the mouth, and maintain the awareness of their breathing without attempting to control it. While performing the exercises with the eyes closed, the patients were encouraged to visualize the outside world. If tension was experienced, inhalation was guided by counting to 5 or 10, followed by slow exhalation.
– Muscle exercise therapy: Performed in a series of 5 repetitions, with 5 series per day. The patients were instructed to look upward with the jaws slightly apart and open their mouths slowly, maintaining the open position for a few seconds before closing gently. Each repetition was followed by inhalation through the nose and exhalation through the mouth.
– Puffing therapy: Performed 5 times daily for 5 min. The patients produced a gentle puffing sound with the lips to relax the cheeks, jaws and lips, exhaling through the mouth, with the lips lightly in contact. They were then instructed to maintain a small gap of a few millimeters between the maxillary and mandibular teeth while the mandible remained in a resting position, keeping this relaxed posture except during eating or speaking. These exercises were also performed following the episodes of tooth clenching.
– Self-massage: Performed in a series of 5 repetitions, with at least 3 series daily, each lasting 3 min. The patients were instructed to habitually relax the facial and jaw muscles throughout the day. During the massage, TMJs and the surrounding muscles were gently treated by placing the fingertips inward, medially from the angle of the mandible, and slowly pushing the skin upward. Proper breathing was incorporated during the exercise, with inhalation through the nose and exhalation through the mouth.
Psychological-behavioral therapy consisted in keeping the jaws apart unless swallowing or eating. Moreover, wide mouth opening was to be avoided.
ST group – splint therapy
The patients received a custom-made, thermoplastic, flat-plane relaxation splint placed on the mandible.19, 33, 34 Occlusal splints were fabricated from a 2.0-mm hard thermoplastic resin sheet (Erkodur; Erkodent Erich Kopp, Pfalzgrafenweiler, Germany), using the thermoforming technique. Occlusal contacts between the teeth and the splint were carefully checked and adjusted as necessary. A smooth occlusal splint with evenly distributed contacts in centric occlusion was designed. The patients were instructed to wear the splint nightly (up to 8 h) and were permitted to use it for an additional hour during the day if pain occurred.
Treatment evaluation
The treatment evaluation was carried out during V3 (day 21) and V4 (day 49). The following parameters were evaluated: pain intensity; TMJ sounds; MMO; mouth opening limitation/deviation; deviation in mandibular movement (lateral – right and left, and protrusive). Maximum mouth opening was measured from the incisal edge of the maxillary central incisors to the incisal edge of the mandibular central incisors at the midline. The presence of deviation during mouth opening was evaluated. Both treatment groups (RPD and ST) were evaluated for the reduction of pain in the masticatory muscles sensitive to touch (NRS). Upon muscular palpation, the patients reported the severity of tenderness. The objective and subjective assessment of symptoms and treatment results was performed by a dentist with 25 years of experience.
Statistical analysis
The results were subjected to statistical analysis using the Statistica software (StatSoft, Krakow, Poland). The distribution of variables was assessed using the Lilliefors and Shapiro–Wilk tests. For normally distributed variables, data is presented as mean ± standard deviation (M ±SD), and parametric tests were applied for group comparisons. Variables that deviated from normality are reported as median (interquartile range) (Me (IQR)). For comparisons between the results before and after the treatment with regard to the whole sample (N = 40), the χ2 test was used, with p-values provided. For the comparisons of nominal variables, the non-parametric χ2 test was used, while the Mann–Whitney U test was applied for ordinal variables. For longitudinal related variables, the Wilcoxon signed-rank test was employed. Statistical significance was set at p < 0.05.
Results
Forty women (mean age: 37 ±9 years) completed either RPB or ST, and were evaluated at all follow-up visits: the RPB group (n = 20; mean age: 37 ±9 years); and the ST group (n = 20; mean age: 35 ±9 years).
The prevalence of TMD symptoms in all patients before and after treatment is presented in Table 1. When comparing the data gathered before treatment (day 1) with that obtained after treatment (day 49), statistically significant improvement was noticed in terms of pain reduction in the masticatory muscles, TMJ and muscle tenderness, arm and shoulder pain, and headache in both groups (RPB and ST). Both the number of patients reporting pain and the mean pain score decreased. The parameter that decreased the most was headache attributed to TMD. Also the number of patients reporting occlusal parafunctions, non-occlusal parafunctions, eye symptoms of TMD, ear symptoms of TMD, physical symptoms of TMD (DC/TMD), depressive symptoms (DC/TMD), and mandibular deviation during mouth opening decreased following the treatment. Regarding the extent of painless MMO, statistically significant improvement was found when comparing the values before and after the treatment in both groups. Significant eye (vision) and ear (hearing) symptom reduction (p = 0.001) was observed within the whole group (RPB and ST).
The comparisons of selected parameters (nominal variables) between and within the study groups with regard to 3 visits (V1, V3 and V4) are presented in Table 2
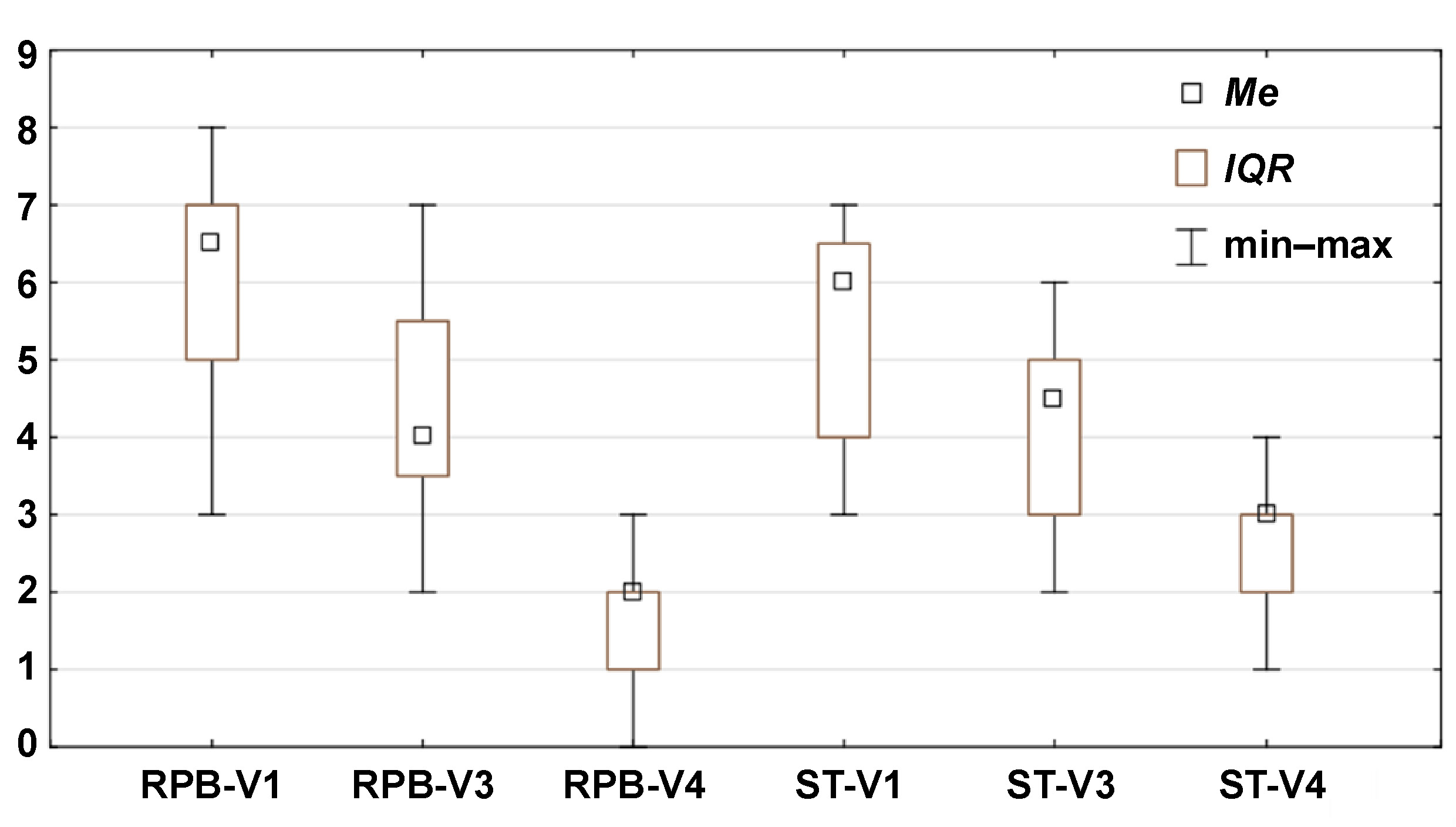
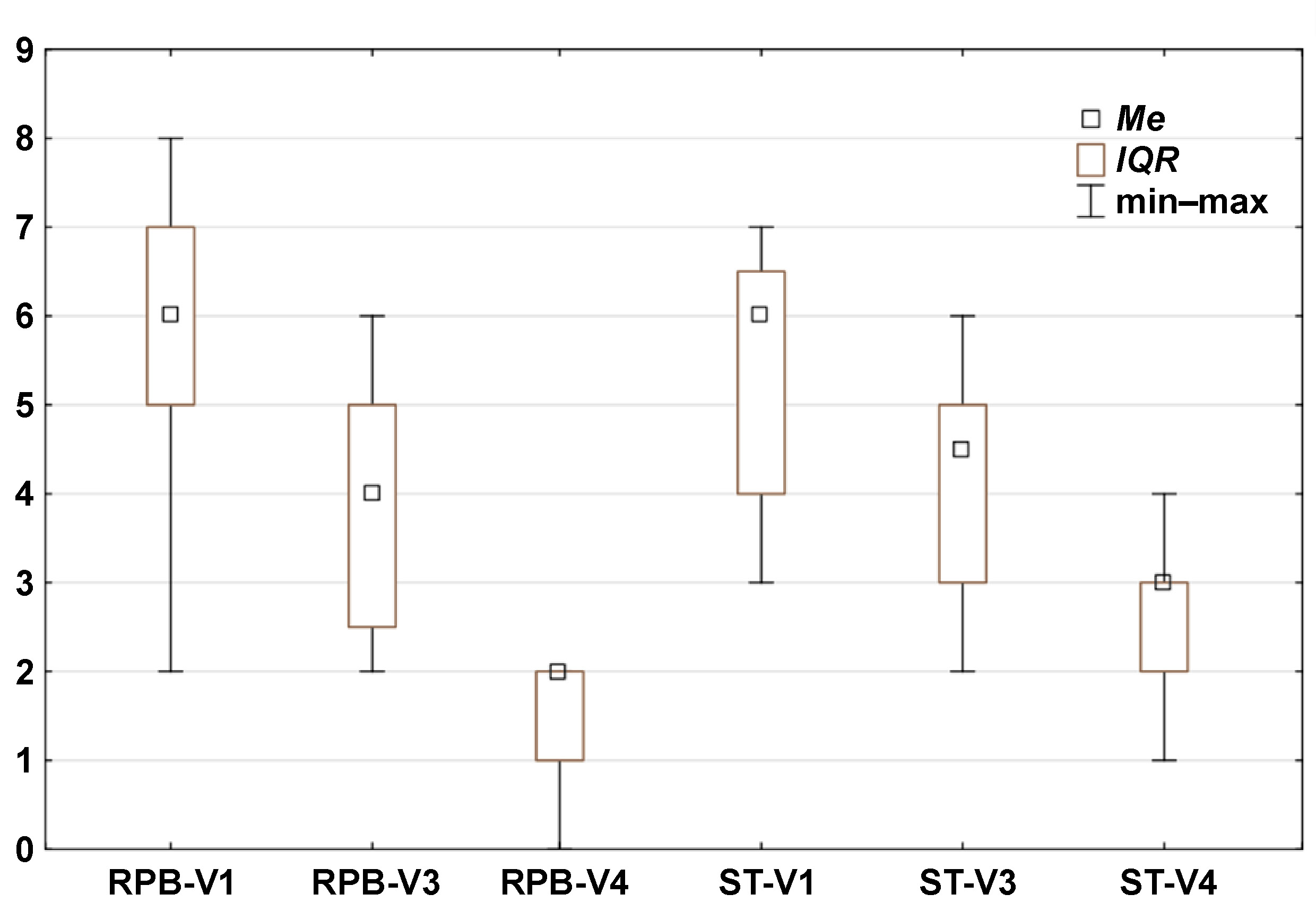
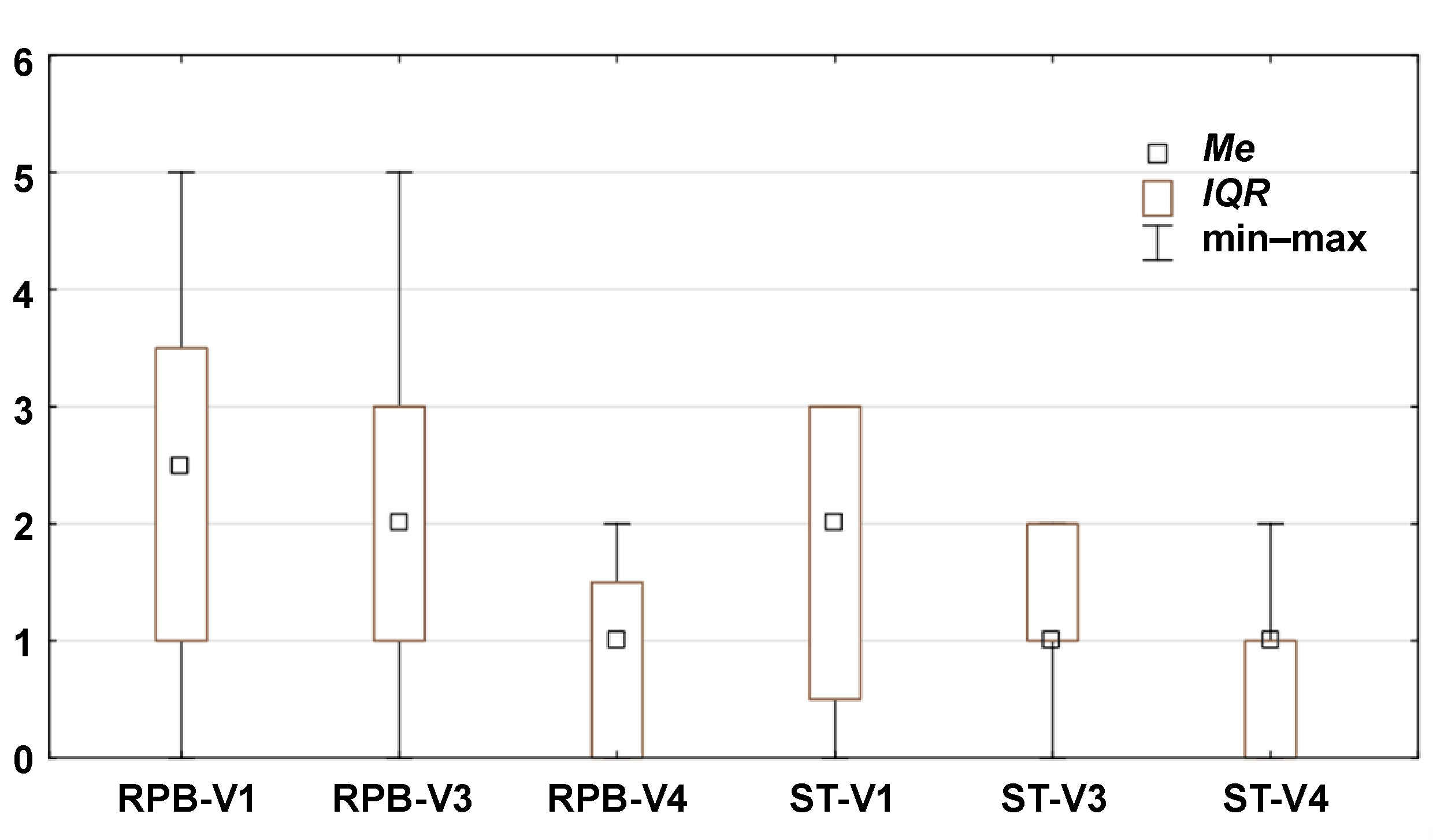
Statistically significant differences in pain reduction during therapy are presented in Figure 3 (pain during function), Figure 4 (TMJ and muscle tenderness) and Figure 5 (arm and shoulder pain). Pain intensity decreased in both groups; however, the reduction was more rapid and more pronounced in the RPB group across all 3 myalgia-related symptoms.
With regard to ordinal variables, differences between the visits within the RPB and ST groups, as well as between-group differences at each time point, are presented in Table 3. Statistical significance was assessed using the Wilcoxon signed-rank test and the Mann–Whitney U test, respectively (p < 0.05).
The statistical significance of differences between and within the 2 groups was as follows:
– a significant difference in pain during function between the RPB and ST groups was observed only at the final visit (V4) (z = −2.64; p = 0.008), while within-group comparisons showed significant differences for both the RPB and ST groups between V1 and V3, as well as between V1 and V4 (z = 3.82; p = 0.000) (Table 3, Figure 3);
– a significant difference in TMJ and muscle tenderness between the RPB and ST groups was observed only at the final visit (V4) (z = −3.10; p = 0.002), while within-group comparisons showed significant differences for both the RPB and ST groups between V1 and V3, as well as between V1 and V4 (z = 3.82; p = 0.000) (Table 3, Figure 4);
– a significant difference in arm and shoulder pain between the RPB and ST groups was observed only at V3 (z = −2.38; p = 0.002), while within-group comparisons showed significant differences for the RPB group between V1 and V3, and for both the RPB and ST groups between V1 and V4 (z = 2.98; p = 0.003, and z = 3.01; p = 0.002; respectively) (Table 3, Figure 5).
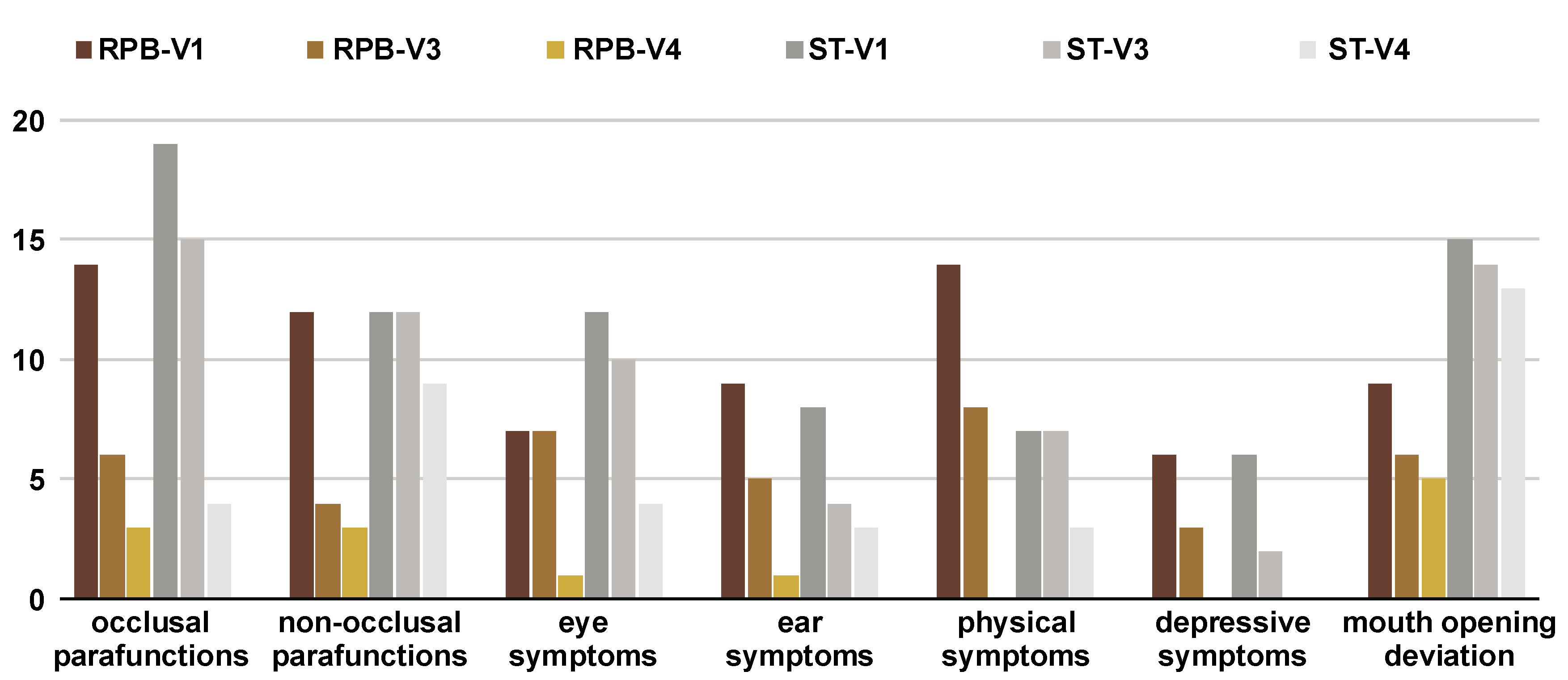
A decrease in the number of patients presenting myalgia symptoms was observed in both therapy groups; however, the reduction was more rapid in the RPB group, particularly with respect to occlusal and non-occlusal parafunctions and mandibular deviation during mouth opening. In the ST group, a statistically significant reduction was observed only at the final visit (V4). A significant reduction in eye- and ear-related symptoms was observed in both the RPB and ST groups (Figure 6).
The effectiveness of therapy on pain intensity was evaluated at V3 and V4. Statistically significant differences between the RPB and ST groups were observed only at the final visit for muscle pain (p = 0.004), pain during function (p = 0.008), TMJ and muscle tenderness (p = 0.002), and headache attributed to TMD (p = 0.014). No significant differences were found between the groups in MMO (Table 3).
Discussion
The study focused on a range of symptoms associated with TMD in women, as well as the effectiveness of various therapeutic approaches in reducing pain severity in the masticatory muscles and/or TMJ, alleviating acoustic symptoms, and improving abnormal mandibular movement. Clinically, masticatory muscle dysfunction is characterized, among other features, by increased muscle tension and tenderness. Tenderness in the TMJ region and joint noises are more common in women than in men.35, 36
More rapid relief and overall reduction of symptoms were observed in the individuals undergoing RPB as compared to those receiving ST. A comparable, statistically significant decrease in pain intensity was noted in the RPB and ST groups, along with a similar increase in MMO. A significant difference between the groups was observed only at the final visit. Symptoms of TMD and headaches were reduced following relaxation exercises.37 The frequency of headaches decreased significantly in the RPB group as compared to the ST group at the last assessment. It appears that most of the accompanying symptoms were stress-related and subsided in the group in which participants learned to consciously control stress or alleviate complaints through muscle relaxation, whereas the use of a splint alone did not result in comparable improvement.
Wieckiewicz et al. concluded that conservative management – including counseling, exercises, occlusal splint therapy, massage, and manual therapy – should be considered the first-line treatment for TMD-related pain due to its low risk of side effects.38 According to Michelotti et al., short-term education was slightly more effective than an occlusal splint provided without education in reducing spontaneous muscle pain in patients with TMD, while no significant differences were observed between the two approaches in terms of pain-free mouth opening, headache or chewing pain.39 A stabilization splint may play a significant role in the short-term management of TMD; however, its effects appear comparable to those of other therapeutic modalities.40 In contrast, findings from an RCT by Wahlund et al. suggest that in adolescents with TMD pain, standardized clinical treatment involving occlusal appliance therapy is more effective than therapist-guided relaxation training in terms of self-reported improvement after a 6-month follow-up.41 Furthermore, a systematic review and meta-analysis of RCTs demonstrated that well-adjusted hard stabilization appliances are more effective in reducing joint and muscle pain in comparison with no appliance, soft stabilization appliances, anterior bite appliances, and non-occluding appliances.42
Population-based studies have previously examined the associations between TMD and psychological variables, pain conditions and oral PHs.43 The findings of the cited study suggest the presence of a shared central mechanism underlying both TMD and headache.43 Therefore, healthcare providers should not consider these disorders in isolation, but rather adopt a broader perspective to better understand the complexity of the diagnostic and therapeutic process.44
In the present research, the RPB group patients, who were aware of their PHs and performed exercises, achieved improvement (in eye- and ear-related as well as physical symptoms) comparable to that observed in the ST group. A reduction in the number of patients presenting with myalgia was noted in both groups; however, this decrease occurred more rapidly in the RPB group, particularly with respect to the reduction of both occlusal and non-occlusal parafunctions.
Makino et al. compared a combination of jaw exercises and psychological interventions aimed at reducing parafunctional activities, demonstrating that this approach is more effective than jaw exercises alone in reducing craniocervical pain in the absence of organic abnormalities.45 Patients with TMD and myalgia often present with a combination of psychological and somatic components.11, 12 Kalamir et al. evaluated the efficacy of self-care in comparison with manual therapy and splint therapy, reporting similar effectiveness across these approaches.46 In contrast, Michelotti et al. investigated a combination of self-care with other modalities, such as manual and exercise therapy, and found that combined treatment strategies were more effective than self-care alone.47
According to various authors, the effectiveness of relaxation occlusal splints with a minimal standard vertical dimension in reducing TMD symptoms of muscular origin ranges from 70% to 90%.48, 49 These effects include, among others, a reduction in face and head pain, improvement in the range of mandibular movement, and decreased tenderness on palpation of the masticatory muscles and TMJ. Kurita et al. reported a reduction in dysfunction symptoms in 84% of patients and complete resolution in 41% of cases following the use of standard-height splints.50 According to the guidelines of the American Academy of Orofacial Pain (AAOP), the purpose of a stabilization appliance is to “provide joint stabilization, protect the teeth, redistribute the occlusal forces, relax the elevator muscles, and decrease bruxism.” Additionally, “wearing the appliance increases the patient’s awareness of jaw habits and helps alter the rest position of the mandible to a more relaxed, open position.”51 The occluding surface of the appliance should contact the opposing dentition uniformly, evenly and simultaneously.
Alqutaibi and Aboalrejal proposed a broad range of management strategies for bruxism and TMD, including conservative and reversible approaches, such as occlusal devices (splints), behavioral techniques, as well as pharmacological and physical therapies.52
Self-care therapy, in contrast to pharmacological treatment, is free from side effects, drug interactions and the risk of overdose. Its efficacy is favorable, and the results remain stable provided that the patient consistently adheres to self-management practices. Our study suggests that maintaining a free space between the jaws (puffing therapy) combined with muscle relaxation may be an effective method for treating TMD, particularly when performed regularly. These exercises may also serve as an initial preparatory phase prior to the implementation of the main therapy.37 It is essential to educate patients about the underlying mechanisms of these disorders – especially the role of emotional stress – and to warn them of habitual parafunctional activities (e.g., non-functional tooth contact or oral mucosa biting). Patients should develop awareness of their oral behaviors and, if such habits recur, make conscious efforts to eliminate them.53, 54
Bae and Park demonstrated that relaxation exercises for the masticatory muscles were effective treatment for the improvement of limited mouth opening and pain reduction in TMD.55 Turk et al. compared the efficacy of relaxation techniques (e.g., biofeedback and stress management) with occlusal splint therapy in patients randomly divided into 3 groups.56 After 6 weeks, pain intensity was significantly reduced in all 3 treatment groups, but occlusal therapy seemed to be more effective. However, at the end of the 6th month, patients treated with occlusal appliances reported the recurrence of symptoms, whereas those under relaxation therapy experienced a further reduction of pain levels. The combined treatment was more effective than either of the single treatment approaches alone, particularly in pain reduction, as observed at the 6-month follow-up.56
A systematic review by Aggarwal et al. provides clear evidence supporting the effectiveness of combined biomedical and psychological interventions, including self-management approaches, in improving long-term outcomes in the treatment of chronic orofacial pain, particularly TMD.31 It is claimed that muscular pain disorders should primarily be managed using conservative approaches. In cases of restricted mouth opening, the additional use of occlusal appliances may rapidly eliminate discomfort.38 Furthermore, self-management interventions have been shown to be effective in patients with chronic orofacial pain, and therapies incorporating physical and psychosocial self-regulation, as well as patient education, appear beneficial.31
We consider the symptoms of TMD – such as pain and tenderness in TMJ and the surrounding muscles and ligaments – to be triggered, among other factors, by the excessive tension in the masticatory muscles associated with parafunctional activities and stress. Therefore, interventions aimed at masticatory muscle relaxation, including targeted exercises and breathing techniques, may represent effective therapeutic strategies.57
As the number of patients reporting depressive symptoms during therapy was similar in both groups, and no such symptoms were reported at the end of the observation period, it may be concluded that the alleviation of TMD-related symptoms contributed to improved patient comfort and the resolution of depressive symptoms.
The authors observed that a combination of relaxation exercise therapy, psychological-behavioral interventions and proper breathing patterns (RPB) was as effective as occlusal splints in improving MMO and reducing pain levels in the treatment of myalgia. These findings suggest that a combined therapeutic approach may yield beneficial outcomes at both early and later stages of treatment, owing to the long-term effects of biobehavioral therapy and the immediate benefits provided by occlusal appliances.58
Given these premises, we propose that combining conventional conservative treatment with psychologically tailored interventions may represent the most effective strategy for managing myalgia.
Within the limitations of the study, including a small sample size, a short follow-up period, the lack of assessment of the longevity of therapeutic effects, the exclusion of patients with dentures (fixed or removable) and those with an open bite, a cross-bite or a prognathic relationship, and the absence of a placebo control group, it is concluded that occlusal splint therapy should not necessarily be regarded the initial treatment for all cases of myalgia. In certain instances, psycho-behavioral-relaxation exercises may be more effective than splint therapy alone.
Conclusions
Relax-psycho-breathing therapy (RPB) and splint therapy (ST) appear to be comparable in managing myalgia-related muscle pain in women. However, in the initial stage of treatment, a comprehensive approach incorporating relaxation therapy may be preferable to occlusal splint therapy alone.
Ethics approval and consent to participate
The study was approved by the Ethics Committee of Poznan University of Medical Sciences, Poland (approval No. 551/15). Written informed consent was obtained from all patients.
Data availability
The datasets supporting the findings of the current study are available from the corresponding author on reasonable request
Consent for publication
Consent for publication was obtained from the patient presented in Fig. 2.
Use of AI and AI-assisted technologies
Not applicable.