Abstract
Background. The presence of severe atrophy in proximity to the maxillary sinus or the inferior alveolar nerve is a primary indication for the use of short dental implants. The placement of standard-length implants in such cases often requires complex regenerative procedures, leading to prolonged healing time and an increased invasiveness of the surgical procedure.
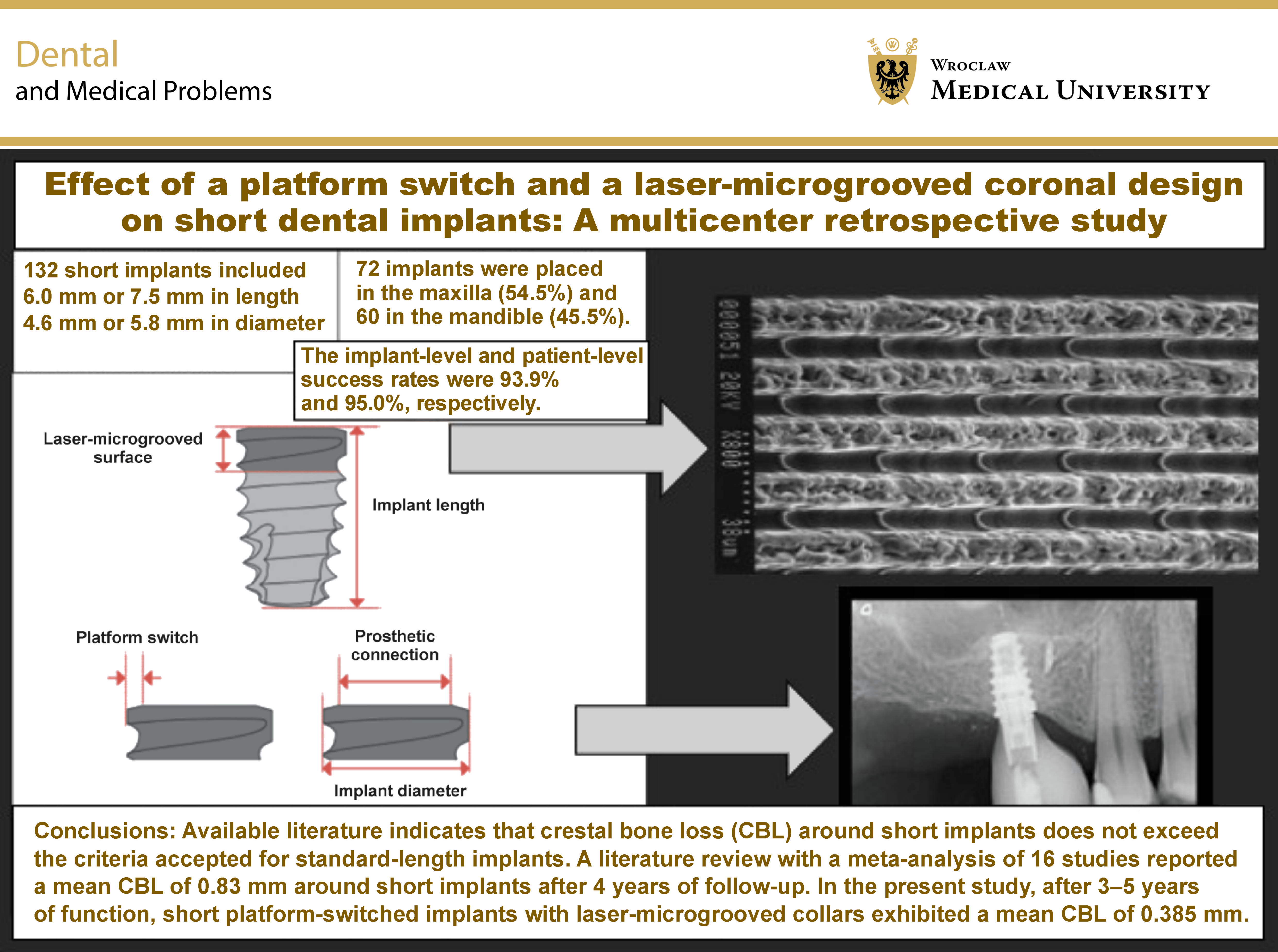
Objectives. The aim of the study was to evaluate crestal bone remodeling, implant success, complications, and implant- and patient-related risk factors associated with the use of short, platform-switched dental implants with a laser-microgrooved collar for prosthetic rehabilitation of atrophic posterior jaws.
Material and methods. This multicenter retrospective study involved a chart review of medical records from 5 private dental clinics. Variables such as age, sex, smoking, periodontal disease, systemic diseases, medications, anatomical location, implant diameter and length, crown-to-implant ratio, and type of placement were collected. A total of 132 short implants placed in 84 patients were analyzed, with a follow-up of 3–5 years (mean (M): 4.2 ±0.8 years).
Results. Eight short implants failed, including 62.5% of those affected by peri-implantitis. The implant-level and patient-level success rates were 93.9% and 95.0%, respectively. The mean crestal bone loss (CBL) was 0.385 ±0.7 mm. Univariate regression analysis revealed that female sex, smoking status and periodontal disease were significantly associated with implant success at both the implant and patient levels.
Conclusions. Platform-switched short implants with a laser-microgrooved coronal design demonstrated high success rates in atrophic posterior jaws after 3–5 years of function, with stable crestal bone levels.
Keywords: short dental implant, platform switch, laser-microgrooved collar
Introduction
Osseointegrated dental implants with a conventional length of 10 mm or greater represent a well-established modality for the prosthetic rehabilitation of partially and completely edentulous patients. However, their use in cases of severe posterior jaw atrophy, particularly in proximity to the inferior alveolar nerve or the maxillary sinus, often requires additional bone augmentation techniques, which increase both the biological and economic burden for patients.1, 2, 3, 4 In recent years, short dental implants (<10 mm) have been proposed as an alternative approach to avoid advanced bone augmentation procedures in atrophic jaws.5, 6, 7 However, the literature reports conflicting data regarding the success rates of short implants in the atrophic posterior alveolar ridge.5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16 First studies on short dental implants with machined (smooth) surfaces indicated that reduced bone-to-implant contact could represent an important risk factor for failure, especially in low-density bone, such as the atrophic posterior maxilla.8, 9, 10, 11, 12 In recent years, the use of short dental implants with textured surfaces, which augment the integrated surface area, has made it possible to overcome this limitation.13, 14 Preliminary studies have indicated that short implants with textured surfaces present clinical outcomes and success rates comparable to those of standard-length implants in the posterior maxilla.13, 14
The criteria for defining implant success remain a matter of ongoing debate. However, especially for short implants, the maintenance of crestal bone stability is of utmost importance.15 It is generally accepted that bone loss of up to 2 mm during the first year of functional loading, followed by an annual loss of approx. 0.2 mm around the implant neck, can be considered physiological.16 Nevertheless, even this level of crestal bone loss (CBL) may pose a significant concern for the long-term success of short implants compared to standard-length implants. For example, after 5 years of loading, a bone loss of approx. 2.0–2.5 mm around a 6-mm implant would correspond to nearly half of the implant length.
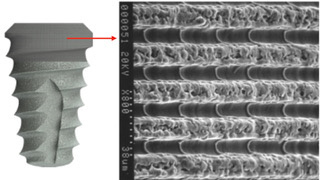
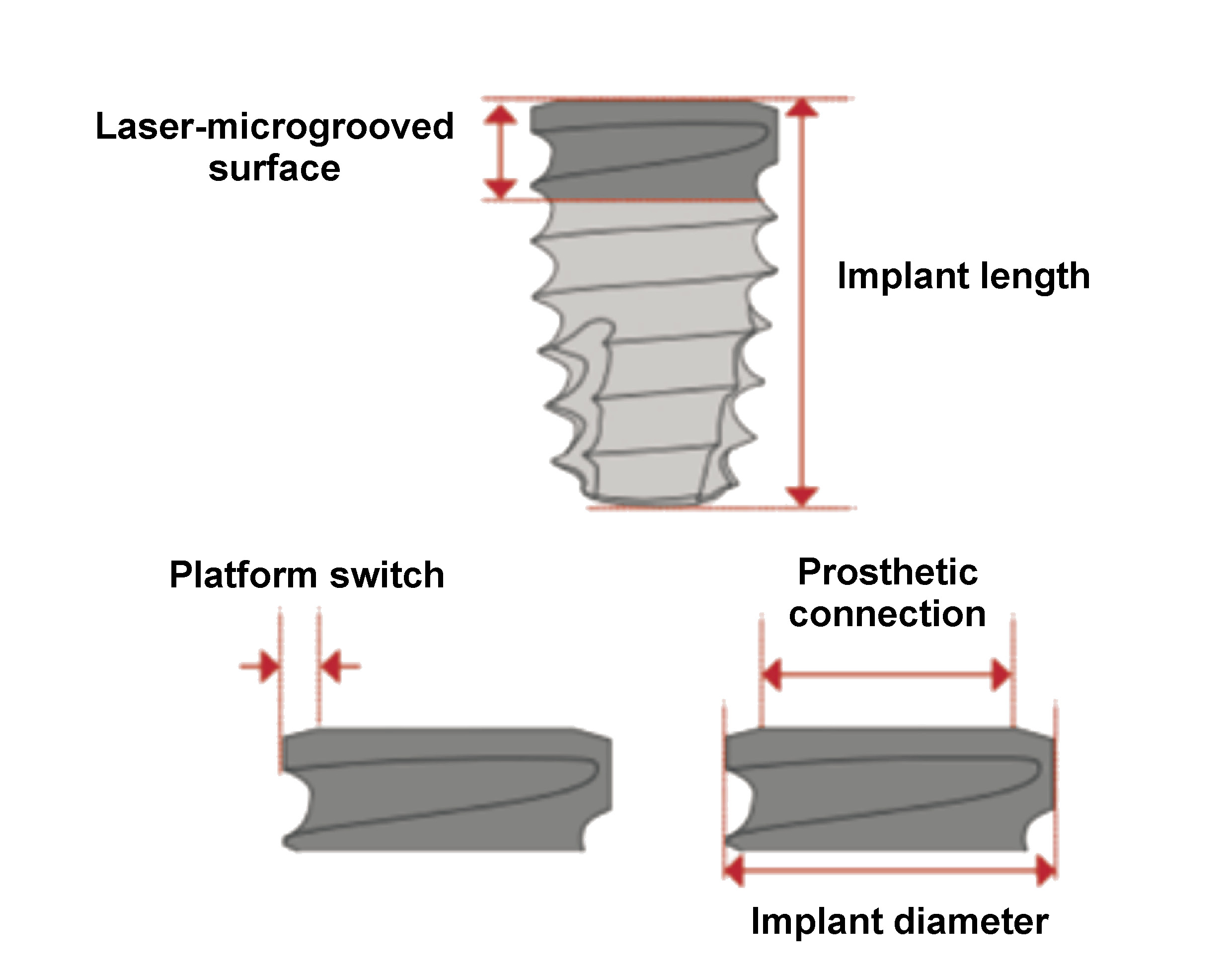
Various implant neck designs and surface modifications have been proposed to minimize CBL. Among these, a platform switch associated with laser-ablated microchannels placed within the implant collar has shown favorable results.17 Platform switching involves the use of a prosthetic abutment with a smaller diameter than the implant platform, thereby influencing the peri-implant biological width through geometric modification of the supracrestal connective tissue space. Additionally, laser-microgrooved surfaces have been developed to guide the alignment and the subsequent growth of fibroblasts at the implant neck (Figure 1).18, 19, 20 Histological studies in humans have demonstrated a different organization of peri-implant soft tissues around laser-microgrooved surfaces compared to machined (smooth) surfaces, characterized by an intimate physical contact of connective tissue and perpendicularly oriented collagen fibers along the laser-ablated, microgrooved implant necks.21
Previous studies evaluating standard-length, platform-switched implants with a laser-microgrooved collar have indicated that the configuration of the coronal part of the implant may counteract CBL.18 To the best of our knowledge, no studies have investigated the combined effect of platform switching and a laser-microgrooved collar on the stability of the marginal bone in short dental implants. Therefore, the objective of the current multicenter retrospective study was to evaluate the clinical and radiographic outcomes of short dental implants featuring a platform switch and a laser-microgrooved collar in atrophic posterior maxillae and mandibles after 3–5 years of loading.
Material and methods
A retrospective, multicenter, clinical and radiographic study was conducted. A clinical database of subjects previously treated within an approved research framework was used; therefore, this study did not require additional approval from an ethics committee. All patients provided written informed consent, and the study followed the guidelines of the Declaration of Helsinki on experimentation involving human subjects. Patients were treated in 5 private dental clinics.
The inclusion criteria were as follows: patients aged ≥18 years; absence of medical conditions considered contraindications to implant surgery; no history of alcohol or drug abuse; presence of resorbed posterior edentulous jaws requiring prosthetic rehabilitation with dental implants; and the presence of residual bone height to allow placement of implants of at least 6 mm or 7.5 mm in length, as well as residual bone width of at least 4.6 mm, as assessed by cone beam computed tomography (CBCT).
The following exclusion criteria were implemented: poor oral hygiene (full-mouth plaque score and full-mouth bleeding score >25%); and discontinuation of supportive periodontal therapy.
Patients were classified as periodontally compromised when ≥3 mm of attachment loss and ≥30% of radiographic bone loss affecting at least 30% of sites were present.
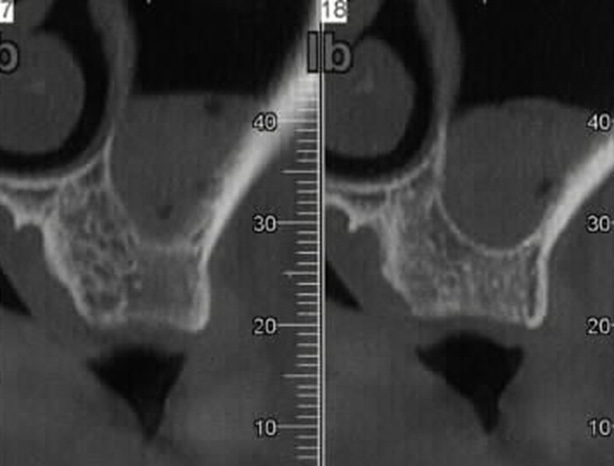
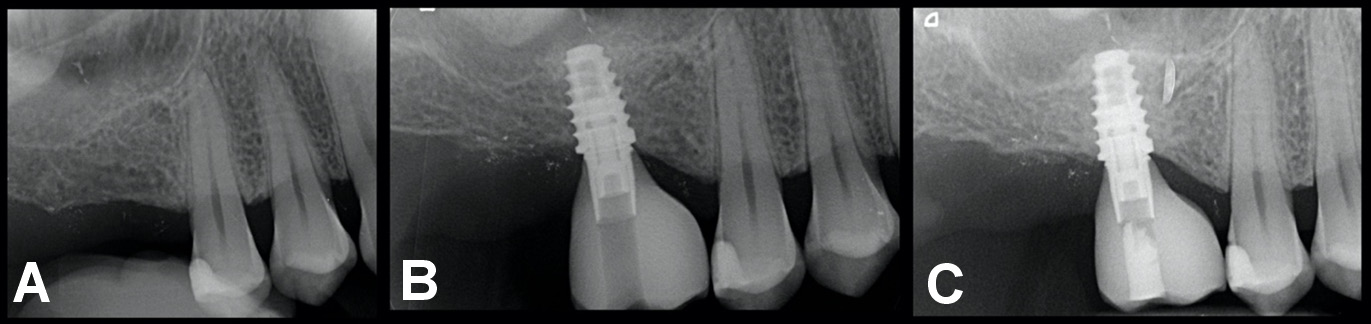
The analysis included 84 patients (44 men (52.4%) and 40 women (47.6%); mean age: 52.49 ±11.23 years) who underwent implant therapy between December 2015 and December 2018. Patients with severely atrophied, partially edentulous ridges (Classes III and IV according to Cawood and Howell19), with ≥8 mm of residual bone height and a thickness of ≥6 mm who received at least 1 short implant (≤7.5 mm) supporting a single crown were included in the study (Figure 2). Smokers, patients with periodontal disease (treated or untreated) and individuals with systemic conditions not considered absolute contraindications to implant surgery were included. Intraoral radiographs, CBCT scans, diagnostic wax patterns, and surgical templates were used for presurgical evaluation. At the end of the follow-up period (mean (M): 4.2 ±0.8 years), a total of 132 short implants were evaluated.
Surgical protocol
The same surgical protocol was applied in all patients. Antibiotic therapy consisted of amoxicillin and clavulanic acid (Augmentin; GlaxoSmithKline, Verona, Italy) at a dose of 1 g twice a day for 7 days, and rinses with 0.12% chlorhexidine digluconate solution (Dentosan; Johnson & Johnson, New Brunswick, USA) twice daily for 1 min prior to surgery. Infiltrations of articaine with epinephrine (Citocartin 1.7 mL; Molteni Dental, Milan, Italy) were used for local anesthesia. A full-thickness flap was then elevated at the level of the keratinized mucosa, with care taken to preserve the periodontal integrity of adjacent teeth. Implant placement was carried out according to the manufacturer’s instructions. Finally, 4-0 or 5-0 monofilament sutures were used and left in place for 10 days. Postoperatively, ibuprofen 600 mg was prescribed, with an additional dose administered after 8 h. Second-stage surgery for placement of healing abutments was performed after 4–6 months, followed by prosthetic restoration delivery at 5–7 months after implant placement.
Implants
Short implants with a platform switch and a laser-microgrooved coronal design (Tapered Short; BioHorizons, Birmingham, USA) were used in all patients (Figure 3). The implants varied in diameter (4.6 mm and 5.8 mm) and length (6.0 mm and 7.5 mm), depending on the bone dimensions at each site.
Follow-up
Patients were recalled at 5–10, 30, and 90 days following implant placement for clinical evaluation. After crown delivery, patients were enrolled in a 6-month recall program for professional oral hygiene maintenance. The following parameters were recorded at crown delivery and at each control visit: number of sites with plaque; number of sites with bleeding on probing (BOP); probing depth (PD); and mucosal recession (REC). Additional variables included anatomical location, implant diameter and length, type of placement (immediate or conventional), smoking habits, presence of periodontal disease, systemic diseases, pharmacological therapies, and implant success (time). Based on the criteria proposed by Albrektsson et al.,16 implant success was defined as the absence of mobility, peri-implant radiolucency and pain, as well as the absence of infection, neuropathy, paresthesia, or any violation of the mandibular canal. In addition, annual bone loss after the first year of function was required to be <0.2 mm.
For radiographic assessment, an individualized acrylic device was fixed to the residual dentition, and a radiograph holder was constructed for each patient. This technique ensured that the same position of the radiograph film could be reproduced at each visit, and the angle of the radiograph would not deviate.
Crestal bone loss was assessed radiographically on the mesial and distal sides of each implant by subtracting the CBL value at baseline from CBL at the 3/5-year follow-up visits. Measurements were calculated using imaging software (Gendex™ VixWin™ Platinum; Gendex, Des Plaines, USA).
To ensure reproducibility, calibration of the examiners was performed (1 examiner per clinic) by repeated assessment of clinical and radiographic parameters in the same 10 patients and using the same radiographs at a 1-week interval, achieving an intraexaminer reliability of 90%.
The following clinical variables were recorded:
• plaque score: assessed at 4 sites per implant (mesial, midfacial, distal, and palatal) using a dichotomous scale (0 = no visible plaque at the soft tissue margin; 1 = visible plaque at the soft tissue margin);
• probing depth: measured to the nearest 0.5 mm at 4 sites per implant (mesial, midfacial, distal, and palatal) using a manual probe (CP 15 UNC; Hu-Friedy Manufacturing, Co., LLC, Chicago, USA);
• bleeding on probing: recorded at 4 sites per implant (mesial, midfacial, distal, and palatal) using a dichotomous scale (0 = no bleeding; 1 = bleeding).
Statistical analysis
The sample size was determined based on previously published data.13, 14 The following parameters were used: a minimal detectable difference between means of 0.5; standard deviations on the difference between means of 0.7; an effect size of 0.71; a beta error of 10%; and a one-tailed alpha error of 5% with an 80% power. These calculations indicated that a minimum of 84 patients was required. Data analysis was conducted using the SAS/STAT® software (v. 9.2; SAS Institute Inc., Cary, USA). The data was analyzed to evaluate the survival rate of this type of rehabilitation at 5 years post-loading. Changes in CBL between baseline and 3/5-year follow-up were assessed using the Wilcoxon signed-rank test. The level of significance was set at 0.05. Homogeneity of variance and normality were assessed using Levene’s test and the Shapiro–Wilk test, respectively.
Repeated measures analysis of variance (ANOVA) was used for inter- and intragroup comparisons over time. Variability within and between subjects was used to estimate standard errors for regression coefficients. Bonferroni correction was used to maintain the overall type I error at α = 0.05.
Results
Out of the 84 patients included, 25 (29.8%) were smokers, 31 (36.9%) had been diagnosed with periodontal disease, while 8 (9.5%) and 3 (3.6%) presented type I and type II diabetes mellitus, respectively. Twenty individuals (23.8%) had other systemic diseases (Table 1). A total of 72 implants were placed in the maxilla (54.5%) and 60 in the mandible (45.5%). The distribution of patient- and implant-related variables is summarized in Table 1 and Table 2. At the end of the study period, 8 implants were lost in 6 patients. Of these, 5 implants (62.5%) were lost due to peri-implantitis. The implant-level and patient-level success rates were 93.9% and 95.0%, respectively (Table 3). Female sex, periodontal disease and smoking were significantly associated with implant failure at both the implant and patient levels (Table 4, Table 5). No statistically significant correlations were found between the remaining variables and short implant failure.
Regarding CBL, the mean values recorded after 5 years of follow-up were 0.38 ±0.7 mm at the mesial aspect and 0.39 ±0.6 mm at the distal aspect (Figure 4). Mean MBL values were higher in smokers (0.64 ±0.6 mm), periodontally compromised patients (0.66 ±0.4 mm) and females (0.61 ±0.7 mm). These differences were statistically significant.
Discussion
The present retrospective study aimed to evaluate crestal bone remodeling, implant success, complications, and implant- and patient-related risk factors associated with short, platform-switched dental implants with a laser-microgrooved collar used for prosthetic rehabilitation of atrophic posterior jaws over a follow-up period of 3–5 years. The majority of previously published studies have included 8-, 9- and 10-mm-long implants and patient populations without unfavorable conditions that could negatively influence implant success.9, 10, 19, 21, 22 In contrast, the present multicenter study exclusively evaluated 6.0- and 7.5-mm-long implants and included a broader patient population regardless of systemic conditions, periodontal status, smoking habits, or type of restoration. The results demonstrated that periodontal disease, smoking and female sex were significantly associated with short implant failure. The effect of a history of periodontitis on implant success has been widely documented.22, 23 However, only few studies reported data on short implants. Carra et al.evaluated the long-term outcomes of 213 short implants (≤10 mm) and reported comparable outcomes in patients with and without periodontal disease.22 Similar findings have been reported by Correia et al.24 in a sample of 202 patients (53% with a history of periodontal disease) and 689 implants, as well as by Zuffetti et al.,25 who analyzed 254 short implants (≤7.5 mm) in 174 patients, including 51 with a history of periodontitis. On the contrary, Hasanoglu Erbasar et al. noted a significant relationship between a history of periodontal disease and short implant failure.26 The findings of the current study indicate that patients with a history of periodontal disease are at increased risk of short implant failure. Despite strict adherence to supportive maintenance therapy during follow-up, peri-implantitis was diagnosed in 62.5% of implant failures. The etiology of periodontitis and peri-implantitis is bacterial.27 It can therefore be hypothesized that a similar complex pathogenic dysbiotic microbiota may trigger a dysregulated inflammatory or immune response, ultimately leading to the loss of both periodontal and peri-implant supporting tissues.27 However, further analysis is needed to confirm these results.
It is extensively documented that smoking is an important patient-related risk factor for the failure of standard-length dental implants.28 Its negative impact has also been documented for short implants.29 A recent systematic review reported a failure rate of 0.008 implants/year in smokers compared to 0.004 implants/year in non-smokers.29 In the present study, smokers comprised two-thirds of peri-implantitis cases. This data is in agreement with the study by Rinke et al.30 and Karoussis et al.,31 who reported a higher prevalence of peri-implantitis among smokers. The significant association between female sex and short implant failure may be related to a higher rate of periodontal disease and smoking within this subgroup in the present sample.
The use of short dental implants for the rehabilitation of atrophic jaws is supported by biomechanical evidence indicating that most of the load stress around dental implants is concentrated at the crestal bone level, while minimal stress is distributed apically.32 Therefore, preserving crestal bone is critical for the success of short implants. In implants measuring 6.0–7.5 mm in length, even physiologically acceptable levels of CBL may, over time, drastically reduce the percentage of bone anchorage.
Crestal bone loss has been associated with several factors, such as implant design, bone density, surgical trauma during implant placement, occlusal overload, and apical migration of the junctional epithelium to isolate bacterial infection or to establish the biological width.33
Platform switching34 and laser-microgrooved surfaces35 are implant design modifications aimed at reducing CBL. Platform switching involves the use of prosthetic abutments with a smaller diameter than the implant platform at the implant–abutment interface. This configuration results in a geometric manipulation of the supracrestal connective tissue, which thickens horizontally and may help protect the crestal bone from reabsorption. Another method attempting to reduce crestal bone remodeling is the use of a laser-microgrooved coronal surface at the implant neck. Laser-microgrooved surfaces were developed to modify cellular interactions with the titanium surface. These surfaces are created using controlled excimer laser ablation, which allows for the creation of a microgeometry characterized by parallel linear grooves with resolution in the micrometer range (Figure 1). Pre-clinical studies have shown that laser-microgrooved surfaces present a high potential for the growth of fibroblasts and effective inhibition of epithelial cell migration across the grooves.19 In contrast to implants with machined (smooth) necks, which typically exhibit a parallel distribution of collagen fibers, histological analyses have demonstrated that laser-microgrooved surfaces promote a more intimate connective tissue attachment, with fibers oriented perpendicularly to the implant surface.20 This configuration may contribute to improved protection of peri-implant crestal bone remodeling.35, 36, 37
Available literature indicates that CBL around short implants does not exceed the criteria accepted for standard-length implants. A literature review with a meta-analysis of 16 studies38, 39, 40 reported a mean CBL of 0.83 mm around short implants after 4 years of follow-up. In the present study, after 3–5 years of function, short platform-switched implants with laser-microgrooved collars exhibited a mean CBL of 0.385 mm. These results highlight the effectiveness of this configuration in preserving peri-implant marginal bone levels, even in short implants.41, 42
Limitations
However, the outcomes of the present study must be interpreted with caution due to several limitations, including the study’s retrospective design and the exclusive use of single crowns supported by short implants, which limits the possibility of evaluating the influence of different types of restorations on implant success. On the other hand, all eligible patients treated with short implants were included, regardless of their medical condition, smoking status or history of periodontitis, thereby minimizing selection bias and increasing the applicability of the study findings to the general population. Additional limitations include the multicenter nature of the study, involving different private clinics, and the lack of evaluation of potentially relevant variables, such as the presence or absence of keratinized mucosa.
It could be assumed that, due to aforementioned limitations, the present study may report more variable outcomes compared to efficacy studies with small, well-controlled and selective groups. However, effectiveness studies such as this one may better reflect outcomes achievable in routine clinical practice.
Conclusions
Short, platform-switched implants with laser-microgrooved collars supporting single crowns in atrophied posterior alveolar ridges demonstrate high long-term success rates. Furthermore, this implant design maintains stable crestal bone levels over time.
Ethics approval and consent to participate
Not applicable.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.