Abstract
Background. Radiation-induced and drug-induced bone necrosis present significant challenges for maxillofacial surgery departments and dental clinics. While the incidence of osteoradionecrosis (ORN) has decreased, the number of cases of medication-related osteonecrosis of the jaw (MRONJ) has markedly increased. This trend is associated with higher life expectancy and more frequent use of medications linked to MRONJ. To date, no uniform, scientifically validated treatment standards have been established for these conditions.
Objectives. The aim of the study was to evaluate treatment outcomes in patients with ORN and MRONJ, as well as to identify risk factors for complications, with particular emphasis on differences in clinical presentation and management.
Material and methods. A retrospective analysis of medical records over a five-year period was conducted, including the charts of patients diagnosed with MRONJ and ORN who were hospitalized at the Department of Maxillofacial Surgery, Poznan University of Medical Sciences, Poland, and subsequently followed up in the outpatient setting. Selected parameters included C-reactive protein (CRP), smoking status, type of necrosis, sex, and hospitalization time.
Results. Differences in patient characteristics, including age, sex, smoking status, and clinical presentation, were observed between the groups. Patients with MRONJ were, on average, 5 years older than those with ORN and exhibited a significantly higher concentration of CRP, indicating a more pronounced inflammatory response. Smoking was identified as a weak but notable predictor of the need for mandibular resection. Additionally, elevated concentrations of CRP were associated with longer hospitalization and a higher incidence of complications, potentially contributing to prolonged hospital stays and an increased risk of adverse outcomes.
Conclusions. The findings highlight distinct clinical courses for MRONJ and ORN, underscoring the need for differentiated treatment strategies. Given the lack of standardized treatment protocols, the observed variations in clinical outcomes suggest the necessity for more targeted therapeutic approaches. Further research is essential to establish effective treatment protocols.
Keywords: ORN, osteonecrosis, maxillofacial surgery, MRONJ, medication-related osteonecrosis of the jaw
Introduction
Bisphosphonates, antiresorptive drugs, anticancer agents, immunomodulators, and steroids, among others, provide significant benefits to patients with cancer and rheumatic diseases. However, their use is also related to adverse effects, including medication-related osteonecrosis of the jaw (MRONJ).1, 2, 3, 4, 5 Osteonecrosis is defined as exposed bone in the oral cavity that does not heal within 8 weeks in a patient receiving medications associated with MRONJ and with no history of head and neck radiotherapy.6
The pathophysiology of MRONJ is multifactorial, and its exact mechanism remains unknown. One of the contributing factors is the inhibition of bone remodeling. Bisphosphonates and denosumab impair osteoclast function, leading to delayed bone tissue healing. Inflammation and infection also play significant roles. Most patients who develop MRONJ present with periapical lesions, poor oral hygiene or a history of dental procedures. Additionally, bisphosphonates and antiangiogenic drugs impair the formation of new blood vessels, resulting in reduced blood supply to affected areas and diminished defense mechanisms. The weakening of natural immunity, particularly in patients with cancer and autoimmune diseases, further increases susceptibility to MRONJ. Lastly, genetic factors are mentioned in the literature. Several single-gene polymorphisms have been identified as potential risk factors. However, studies involving large patient groups are lacking.2, 6
Overall, MRONJ results from the interplay of multiple factors. Impaired bone regeneration due to osteoclast inhibition, combined with infection in the oral cavity and limitations in blood flow lead to compromised healing ability and, ultimately, jaw necrosis.
The treatment of MRONJ is challenging and not clearly defined. According to the 2022 guidelines of the American Association of Oral and Maxillofacial Surgeons (AAOMS), conservative treatment is recommended as the first-line approach, including pain management, antibacterial treatment and local debridement of the affected area. In cases where conservative therapy fails, surgical intervention involving the resection of affected bone is recommended.6
Another type of jaw necrosis is osteoradionecrosis (ORN), a rare complication of head and neck radiotherapy,7 first described in 1922.8 Although no universally accepted definition exists, ORN is generally characterized as exposed bone within an irradiated area, unrelated to tumor presence, persisting for 3–6 months.
According to the current state of knowledge, the pathogenesis of ORN is associated with vascular disturbances associated with damage to small blood vessels. Radiation doses exceeding 50 Gy primarily damage small vessels.9 It has been demonstrated that reduced blood flow in these vessels likely contributes to impaired bone turnover, resulting in necrosis.10 The higher incidence of ORN in the mandible, as compared to the maxilla, supports this theory.11, 12 Infections and invasive dental procedures are also considered contributing factors.7
The treatment protocol for ORN is not well-established. Initial management is typically conservative and involves antiseptic rinses and antibiotic therapy. Additional treatment options include hyperbaric oxygen therapy as well as the use of pentoxifylline and tocopherol.7, 13, 14 Surgical treatment involves local debridement, removal of necrotic bone, reconstruction using adjacent tissues, and, in cases of extensive defects, reconstructive surgery. The primary goals of treatment are pain relief, restoration of function and improvement of quality of life.7, 15
Attention should be drawn to the exceptionally rare occurrence of both MRONJ and ORN in the pediatric patient population, which remains an ongoing subject of research.16, 17, 18 Cases of both MRONJ and ORN differ significantly, and the number of detailed clinical descriptions is limited. The pathophysiology and treatment processes differ.
In MRONJ, bone exhibits blocked osteoclast activity. Upon trauma or infection, an inflammatory response arises, but the inability of osteoclasts to address the inflammation leads to its spread. In this scenario, the bone remains viable but becomes inflamed. This process is associated with an increase in inflammatory mediators, such as interleukins (ILs), and the recruitment of immune cells to combat inflammation. Persistent inflammation and the inability to manage it effectively result in necrosis. Consequently, elevated levels of inflammatory markers may be detectable in blood tests.19
Osteoradionecrosis primarily results from vascular damage and reduced blood flow. The theory of radiation-induced fibrosis has been proposed as a three-phase mechanism describing the molecular events leading to clinical manifestations of the disease. The initial prefibrotic phase is followed by an organized phase characterized by abnormal fibroblast activity and disorganization of the extracellular matrix. The late fibroatrophic phase involves tissue remodeling, resulting in fragile, healed tissues susceptible to re-injury. Histologically, ORN is characterized by significant osteocyte destruction and the absence of osteoblasts along bone margins.20, 21
The number of affected patients varies across centers. In most countries, the incidence of ORN remains similar or is decreasing, while the number of MRONJ cases is increasing. The observed rise is presumably due to the growing number of patients receiving bisphosphonates and anticancer therapies.22
An increasing number of studies emphasize the importance of preventing both MRONJ and ORN. Preventive strategies should include patient education as well as the training for healthcare providers delivering primary medical and dental care.23
The aim of the present study was to present and compare cases of MRONJ and ORN in a 5-year retrospective cohort of patients from the Wielkopolska region of Poland, with the goal of providing data to support future research.
Material and methods
The study involved an analysis of medical records obtained from the Department of Maxillofacial Surgery, Poznan University of Medical Sciences, Poland, and its affiliated outpatient clinic, where follow-up visits were conducted. The research was performed in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. The study protocol was approved by the Bioethics Committee at Poznan University of Medical Sciences (approval No. KB761/24).
Medical records were identified using the International Classification of Diseases, 10th Revision (ICD-10) diagnostic codes within the hospital’s electronic system. Subsequently, the etiology for necrosis was verified through chart review. All included cases met the diagnostic criteria for either MRONJ or ORN. To reduce potential bias, statistical analyses were performed independently.
Patients eligible for inclusion met the diagnostic criteria for ORN or MRONJ. Surgical qualification was determined by a maxillofacial surgery specialist. Surgery was indicated in patients who developed pathological fractures, experienced exacerbation of inflammatory processes, or did not respond to conservative treatment.
Patient records from March 2018 to March 2023 were analyzed, as full electronic documentation was available from that period. The following variables were evaluated: type of necrosis; sex24; location; age25; C-reactive protein (CRP) concentration, due to its higher levels in a previous study involving MRONJ patients26; smoking status; body mass index (BMI) (underweight, normal weight, overweight, obesity)27; length of hospital stay28; histopathological findings29; and treatment outcomes. Given the higher incidence of surgical complications in older individuals, patients were divided into 2 groups, namely those aged ≥65 years and those aged <65 years. A similar analysis was performed for CRP levels, using a threshold of >10 mg/dL to indicate greater severity of inflammatory changes.26 Oral hygiene was not included due to the absence of questionnaires applicable to this type of research.
The CRP concentrations were measured on admission, and the information about smoking status was given and noted in medical charts on admission and in the anesthesiology form before the administration of anesthesia. All patients presented with comorbidities; however, to perform surgery, these had to be clinically stabilized.
Statistical analysis
During the analyzed period, 162 records of patients hospitalized due to bone necrosis were identified. The normality of data distribution was assessed using the Kolmogorov–Smirnov test. Depending on the distribution, parametric (Student’s t-test) or non-parametric tests (Mann–Whitney U test, χ2 test) were applied. Potential risk of bias was limited to the retrospective character of the study. Selected parameters were chosen as the most objective.
Results
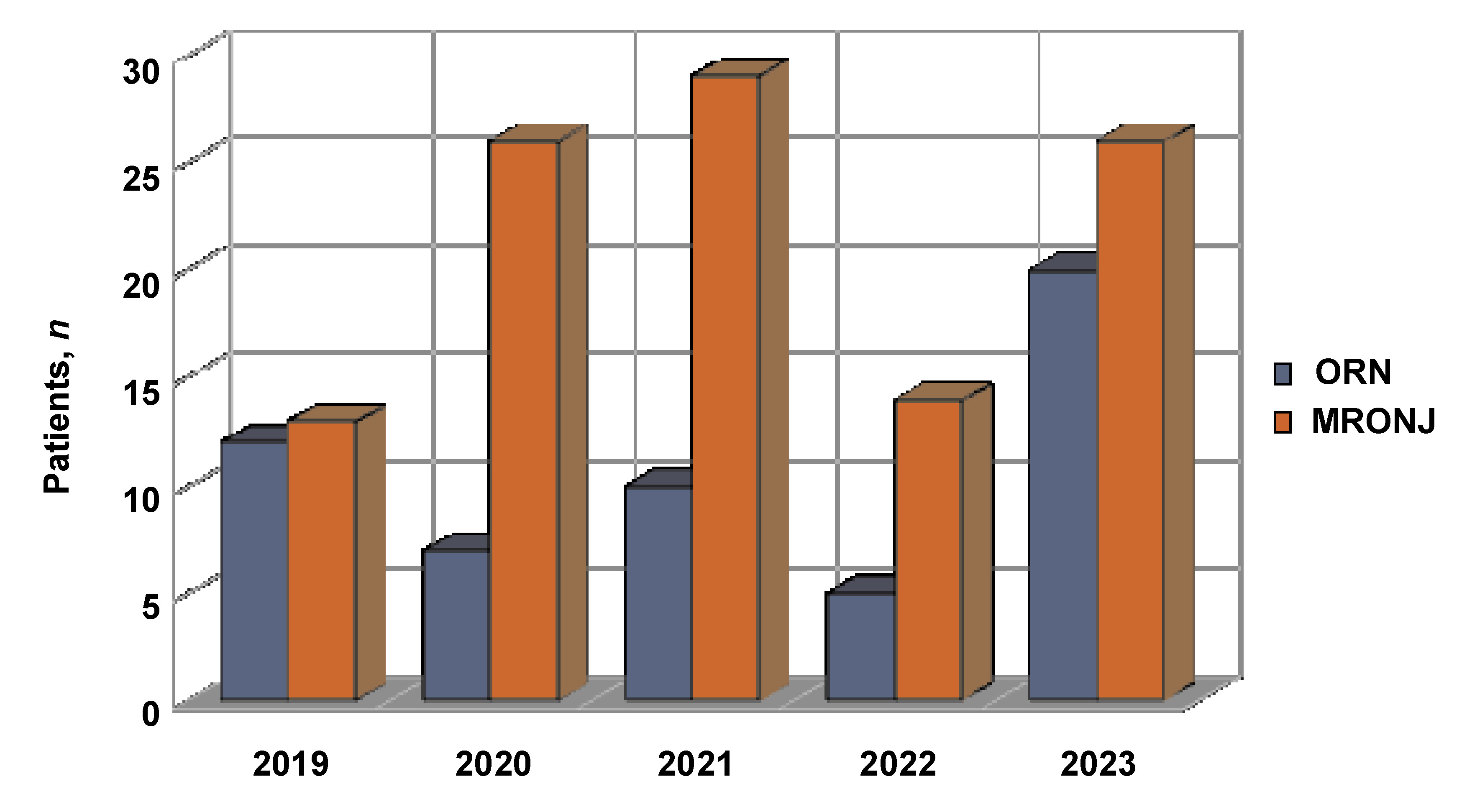
A total of 162 patients were included in the analysis, of whom 108 were diagnosed with MRONJ and 54 with ORN. Over the 5-year period, the number of patients with MRONJ increased during the first 3 years, followed by a decrease, while the number of ORN patients remained stable (Figure 1). A noticeable decline observed in the 4th year (2022) coincided with the coronavirus disease 2019 (COVID-19) pandemic and potential limitations in access to healthcare services.
A statistically significant difference in average age was observed between patients with MRONJ and ORN (68 years vs. 62.9 years; p < 0.05, Mann–Whitney U test), with those affected by MRONJ being, on average, 5 years older. The majority of patients with ORN were smokers. Additionally, smoking was identified as a weak but statistically significant risk factor for bone resection and was associated with a higher rate of complications (Cramér’s V = 0.17; p = 0.04). Male patients predominated in the ORN group.
A total of 143 patients attended at least 1 follow-up appointment. The incidence of complications during follow-up was comparable between the 2 groups. Treatment success was defined as the absence of necrosis and complications at the first follow-up appointment, that is, approx. 6 weeks post-surgery. Subsequent visits were scheduled every 3–6 months, depending on the clinical condition.
Complications occurred in 53 of 93 patients with MRONJ (57%) and in 31 of 50 patients with ORN (62%), with no statistically significant difference between the groups (p > 0.05, McNemar–Bowker test). Patients with MRONJ had notably higher CRP levels at admission compared to those with ORN (21.03 mg/dL vs. 9.35 mg/dL, respectively; p < 0.05, Mann–Whitney U test; 95% confidence interval (95% CI): 4.50–29.02). Elevated CRP concentration was correlated with prolonged hospitalization. Similarly, longer hospital stays were observed in patients who underwent bone resection. Approximately half of the patients reported pain on admission (53/108 in the MRONJ group and 26/54 in the ORN group) and presented with intraoral or extraoral fistulas. Detailed results are summarized in Table 1 and Table 2.
Discussion
In recent decades, the incidence of ORN has decreased, while MRONJ has become more common, reversing the proportions observed over the past century. Similar findings have been reported in other studies.30, 31 This trend is primarily due to the more precise use of radiotherapy techniques and proper dental preparation of patients before treatment.32 The increasing use of antiresorptive drugs in cancer treatment, along with extended life expectancy, has contributed to the rising incidence of MRONJ.28, 31 The decline in MRONJ cases observed in the 4th year coincided with the COVID-19 pandemic, which led to a decrease in the number of patients visiting maxillofacial surgery departments.28, 33, 34, 35
Lockdowns and restrictions in access to healthcare services may have led to delays in treatment initiation. Unfortunately, the use of telemedicine was unable to provide any assistance to these patients. Moreover, treatment delays often resulted in the development of more advanced conditions, including abscesses and pathological fractures, which significantly limited the options for surgical treatment.28, 35
Medication-related osteonecrosis of the jaw predominantly affects older individuals. In the present study, the average age of patients with MRONJ was 68 years. This age group is the primary target for antiresorptive drug use. Age is also correlated with a longer development period for MRONJ.25, 30, 36, 37
Previous studies report a mean age of approx. 60 years for patients with ORN, whereas in the present analysis the mean age was approx. 63 years. This difference may reflect the limited application of radiotherapy or the use of lower doses in older individuals, as the potential risks of complications and limited benefits in this group make aggressive treatment less favourable.38 The findings of this study are consistent with previously published data.30, 31, 39 Patients with MRONJ were, on average, 5 years older than those with ORN. Moreover, patients aged ≥65 years presented complications more frequently during follow-up. This may be attributed to reduced regenerative potential associated with the aging process and a higher prevalence of comorbidities in older individuals, which in turn may increase the need for visits and the associated treatment costs.
Previous reports have indicated a higher prevalence of smokers among ORN patients,30 and similar results were obtained in this analysis. Smoking is a known risk factor for both MRONJ and ORN.27, 30, 31, 40, 41 This phenomenon may partly reflect the higher proportion of smokers among patients with head and neck cancers, as smoking is a significant carcinogenic factor in the development of these malignancies.30, 42 Additionally, smoking impairs oral tissue healing,43 leading to a higher rate of complications, especially in MRONJ patients. There is a weak correlation between smoking status and the need for bone resection. This may be due to the abovementioned factors impairing healing process and the relatively small sample size. Nevertheless, patients should be consistently encouraged to cease smoking.
Smoking alone is unlikely to account for the observed outcomes, which could explain the weak correlation observed. The medical records analyzed in the study did not include standardized questionnaires regarding hygiene. Additionally, exacerbations of conditions such as diabetes in the postoperative period were not monitored. These factors could have an additional impact and should be addressed in future prospective studies, particularly with regard to disease exacerbation during healing process.
Previous studies have reported a higher prevalence of ORN in men,24, 29, 31, 41 which is consistent with the findings of the present study. Similar observations have been described by Grisar et al. and Akashi et al.30, 39 In contrast, earlier research shows that MRONJ occurs more frequently in women, with female sex often cited as a risk factor for disease development.29 However, in this study, the incidence of MRONJ was comparable between sexes. This could be explained by the increasing use of antiresorptive drugs among men, particularly in the treatment of prostate cancer, renal cancer and multiple myeloma.44, 45, 46 In addition, increased life expectancy among men has led to a higher incidence of neoplastic diseases. Lifestyle factors, including higher rates of tobacco and alcohol use, may also contribute to the development of necrotic lesions30 in the oral cavity, leading to an increase in MRONJ cases. Equally significant risk factor is the generally lower level of oral hygiene among men.
The role of specialized breast units should also be considered. Physicians specialized in the treatment of female cancers may be more aware of MRONJ risk and more likely to implement preventive measures. Furthermore, studies suggest that women are generally more aware of the risk of MRONJ and more frequently seek information from medication package inserts.47
The treatment of bone necrosis is not free of complications. In this study, complications were defined as the occurrence of intraoral or extraoral fistulas, pain, sensory disturbances, disease recurrence, impaired wound healing or dehiscence, and pathological fractures during follow-up. The complication rates were high and comparable between the groups – 57% for MRONJ and 62% for ORN, highlighting the difficulty of treating both conditions. These results differ from some previous reports for both MRONJ40 and ORN.41 Improved outcomes reported in ORN studies may be attributed to the use of reconstructive techniques, such as microvascular flaps, which were not employed in the treatment of ORN in the present study. Furthermore, limited access to oral and maxillofacial surgery treatment may have contributed to poorer outcomes. Patients often initially consult primary care physicians or dentists, and limited awareness of the condition may delay the initiation of appropriate treatment.
Inflammatory processes likely play a significant role in the development of MRONJ.1, 2, 3, 4, 42 In this study, the concentration of CRP was significantly higher in patients with MRONJ than in those with ORN. Previous research has identified elevated CRP as a marker of postoperative complications.48 However, no studies have examined the impact of CRP concentration on treatment outcomes in ORN. The current analysis also revealed a correlation between hospitalization time and CRP concentration in MRONJ patients, with higher concentrations of CRP leading to longer hospital stays. Although a similar trend was observed in ORN patients, it did not reach statistical significance.
When analyzing this data, it is important to consider the low specificity of CRP. Elevated CRP concentrations are also observed in rheumatic and neoplastic diseases,49 which affect a large proportion of patients with MRONJ. However, 1 study demonstrated higher CRP concentrations in patients with MRONJ compared to individuals receiving bisphosphonates without clinical signs of the disease.50 Additionally, elevated CRP levels have been observed in patients receiving intravenous bisphosphonates,51 and this route of administration is itself a risk factor for the development of MRONJ.
The limited specificity of CRP reduces its utility as a sole marker of complications. Nonetheless, future analyses should consider the concentration of CRP alongside other variables that potentially affect MRONJ or ORN treatment outcomes. This is especially relevant given that elevated CRP concentrations are commonly observed in patients with necrotic lesions.50, 51, 52
Due to the inflammatory component and frequent bacterial infections, patients with MRONJ often present with purulent fistulas. Swabs obtained from these areas allow for antibiogram analysis and targeted treatment. In many cases, this necessitates intravenous antibiotic therapy with agents available only in hospital settings, potentially prolonging the hospitalization period for these patients.
Elevated CRP levels in this patient group indicate the severity of inflammation and the necessity of initiating antibiotic therapy. Effective control of the inflammatory process significantly facilitates surgical procedures; however, it requires time and may delay surgery. Individuals with MRONJ frequently undergo chemotherapy, which compromises the body’s ability to combat infection. Therefore, early assessment of inflammatory markers upon admission, followed by timely initiation of antibiotic therapy rather than limiting treatment to the perioperative period, appears justified.
The current analysis found a correlation only with CRP concentration; no such relationship was observed for white blood cell (WBC) counts. Future studies on MRONJ could consider measuring markers such as IL-6, as increased expression of IL-6 receptors has been observed in patients affected by MRONJ.53
Data on the duration of hospitalization in patients with jaw necrosis is scarce. One study reported a 10-day hospital stay for MRONJ patients, attributed to the need for a 5-day course of intravenous antibiotics prior to surgery.54 No comparable data was identified for ORN. In the present analysis, patients undergoing bone resection had longer hospital stays in both MRONJ and ORN cases, likely due to the extent of the surgery. Prolonged hospitalization is also associated with increased treatment costs.
Patients with an elevated CRP concentration and MRONJ experienced longer hospital stays, likely due to the need for inflammatory markers to decrease. Another important factor is the presence of systemic diseases, particularly oncological conditions. These patients often develop anemia as a result of ongoing treatment, which may necessitate blood transfusions in the preoperative or postoperative period.
Bone resections are performed in the most advanced stages of necrosis.6, 7 According to previous studies, between 12% and 25% of ORN patients require bone resection.39, 55, 56 Similar proportions have been reported for MRONJ,57 although some studies state that nearly half of MRONJ patients undergo resection.39 In our analysis, resection rates were similar in both groups but higher than those reported in the literature, reaching 35% for MRONJ and 48% for ORN. This may result from patients being referred late to our facility, with delayed diagnosis resulting from low awareness of the disease.57 Furthermore, due to the limited involvement of the public sector in dental services, patients often initially consult general practitioners, which may prolong the diagnostic pathway.
The center providing care for patients with necrosis serves the Greater Poland and Lubuskie voivodeships, encompassing a significant portion of western Poland. These regions have a combined population of approx. 4.5 million, of whom 52% are women. A predominance of women becomes evident in the population pyramid from the age of 55 years. During the study period, our clinic provided services to 4,564 individuals.58, 59
There are relatively few maxillofacial surgery outpatient clinics within the public healthcare system. Moreover, these clinics are located in large cities, while the issues of MRONJ and ORN affect patients across all regions. Transportation barriers and limited access to specialized care prolong the time needed to reach a specialized center. Additionally, it can postpone the implementation of basic treatments, such as rinses or antibiotic therapy, particularly in cases with exacerbated local conditions. Patients without access to specialist care are at risk of pathological bone fractures due to the progression of inflammation, which often necessitates resection.
Pain on admission was present in nearly half of the patients hospitalized with necrosis. The level of pain on admission did not differ significantly between the 2 groups. In available studies, pain was present in the majority of MRONJ (61% and 81%) and ORN (81% and 96%) patients.30, 39 The presence of pain is an important diagnostic signal in at-risk populations. Additionally, pain, as an unpleasant sensation, significantly reduces the quality of life for these patients.60
A common clinical manifestation of necrosis is the formation of intraoral fistulas. In this analysis, such lesions were present in the majority of MRONJ and ORN patients, consistent with previous reports.30, 39 No significant differences between the groups were found. However, skin fistulas were more frequently observed in ORN patients. This observation aligns with the outcomes of other studies,30, 39 and may be related to the poorer condition of the skin in irradiated areas. The mandible remains the most commonly affected site, whereas the maxilla is involved less frequently. This is primarily due to the mandible’s poorer blood supply and its structure, including a lower proportion of cancellous bone.30, 39
Limitations
When considering potential risk factors, it is necessary to account for other clinical situations that may influence treatment outcomes and hospitalization time. As mentioned earlier, several factors may have an impact on the results of this analysis. These include oral hygiene, alcohol consumption and comorbidities. The socioeconomic status of the patient is also of significance, as patients from smaller towns may face difficulties in accessing specialized care.
In the present study, oral hygiene was not assessed using any available standardized indices applicable to scientific studies; thus, this variable was excluded from our analysis. The qualification for performing surgery, except in emergency cases, required stabilization of chronic diseases. Consequently, these conditions were not considered risk factors in the analysis. However, they should be taken into account in future studies, particularly prospective ones, due to the potential for exacerbation and their impact on healing outcomes.
Additionally, relying solely on patient medical history and test results may limit data utility. In this study, we aimed to prioritize objective factors. Nevertheless, a significant portion of the data was based on assessments not conducted by the primary researcher. This limitation is inherent to retrospective studies. However, the potential risk of bias is considered low due to the nature of the data.
Recommendations and future research directions
Many publications emphasize the importance of preventing MRONJ and ORN,61 as the treatment of these conditions remains highly challenging. Nevertheless, instances of improper management are still reported.5
The number of patients at risk for MRONJ and ORN is growing. Education on these conditions should be incorporated into medical and dental curricula. This topic should also form an integral part of postgraduate training, including specialized courses and certification programs. Additionally, not only dentists but also primary care physicians, oncologists and rheumatologists should regularly update their knowledge of MRONJ or ORN, as these specialists most frequently prescribe medications associated with the risk of MRONJ. Improved awareness will facilitate earlier identification of high-risk patients.23
In response to projections regarding oncological diseases, the establishment of care centers for high-risk patients should be considered. Such centers would address the growing number of patients requiring specialized care due to an increased risk of complications. They should ensure interdisciplinary approach to the patient by involving specialists from fields such as dentistry, oncology, and oral and maxillofacial surgery.
In addition to educating healthcare professionals, it is also crucial to increase patient awareness about potential complications. For example, similarly to patients receiving anticoagulants, individuals at risk of MRONJ could be provided with a short leaflet for their dentist, outlining their medication history. This is especially relevant, as some medications are administered every 3 months or for limited durations.
Patients should also be instructed on the importance of meticulous oral hygiene. Highlighting the benefits of this approach should be a key responsibility of the physician initiating treatment.
Historically, the issue of “phossy jaw”, associated with occupational exposure to phosphorus, was mitigated through mandatory dental examinations.62, 63 Similarly, implementing preventive measures, such as ensuring dental clearance of oral inflammatory foci before initiating antiresorptive therapy for oncological treatment, should be considered.
Patients receiving medications associated with MRONJ risk or those who have undergone radiotherapy should be informed about the importance of regular dental check-ups.
There is a lack of large-scale population-based studies on patients with MRONJ and ORN that encompass aspects such as quality of life, oral hygiene levels and systematically collected clinical data. Such studies would facilitate meta-analyses and provide deeper insights.
The introduction of standardized data collection forms, completed by both patients and clinicians, should be considered. These should include information on duration and route of medication administration, type of radiotherapy, pain intensity, oral hygiene (assessed using available scales), smoking status, comorbidities, and other relevant factors.
Currently, non-surgical methods of prevention primarily include enhanced oral hygiene and the use of antibiotics. Antibiotic therapy before and after invasive procedures related to the oral cavity is widely recommended, typically starting 12 h before the procedure and continuing for up to 14 days.64 Antibiotics and chlorhexidine oral mouthwashes are also used in conservative treatment, with moderate effectiveness. Other non-surgical methods include hyperbaric oxygen therapy65, 66 and pharmacological interventions.
The ongoing PENTO study is aiming to assess the possibility of using pentoxifylline and tocopherol in patients with MRONJ.67 The combination of these 2 drugs has already demonstrated positive effects in ORN.68, 69
Surgical attempts include the use of platelet-rich fibrin (PRF) in the socket after tooth extraction to reduce the risk of MRONJ or as a treatment method alone.65, 68, 69, 70
Future research should focus on identifying specific risk factors and evaluating therapeutic approaches, as well as exploring novel prognostic markers, such as IL-6. The absence of standardized treatment protocols highlights the need for randomized clinical trials, which should also consider long-term follow-up.
The majority of available papers is based on case reports and non-randomized studies,71 making it challenging to establish optimal treatment methods. Future research should consider factors such as CRP, IL-6, lesion location, specific interventions (e.g., the use of PRF), and extended follow-up periods.
Conclusions
Medication-related osteonecrosis of the jaw and ORN are distinct conditions, both representing serious complications of modern therapies. While advances in radiotherapy have contributed to a decrease in the incidence of ORN, the number of MRONJ cases has been alarmingly increasing.
Medication-related osteonecrosis of the jaw primarily affects patients with a higher disease burden, particularly those with active cancer. In contrast, ORN typically develops after the completion of treatment. Neither condition has a fully understood pathophysiology, and there is no gold standard treatment. However, both share certain similarities in clinical aspects.
Since diagnosis relies on patient history and clinical examination, clear differentiation between MRONJ and ORN is crucial. Physician awareness of these conditions remains limited but is gradually improving. Therefore, dissemination of clinical data regarding these diseases is important for continued education of healthcare professionals, enhancement of treatment outcomes, and the promotion of wider use of preventive strategies.
Further research should primarily include randomized trials with extended observation periods. During the study design phase, maximum standardization of parameters such as quality of life, oral hygiene status and inflammatory markers should be considered to enable better selection of therapeutic approaches in the future.
Until an effective treatment method is identified, and even thereafter, prevention should be actively promoted. Current preventive measures include antibiotic therapy, minimally invasive procedures and enhanced monitoring of patients in high-risk groups.
To the best of our knowledge, this is the first study to describe patient characteristics and treatment outcomes of MRONJ and ORN in Poland.
Ethics approval and consent to participate
The study protocol was approved by the Bioethics Committee at Poznan University of Medical Sciences, Poland (approval No. KB761/24).
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Artificial intelligence (ChatGPT; OpenAI, San Francisco, USA) was used for language editing and to improve readability.