Abstract
Background. One of the most important aspects of root canal therapy is pain control after treatment. Postoperative pain is an unwanted but common sensation following endodontic procedures. Recently, bioceramic sealers have gained attention in endodontics; however, clinical evidence supporting their effectiveness in pain reduction is still limited.
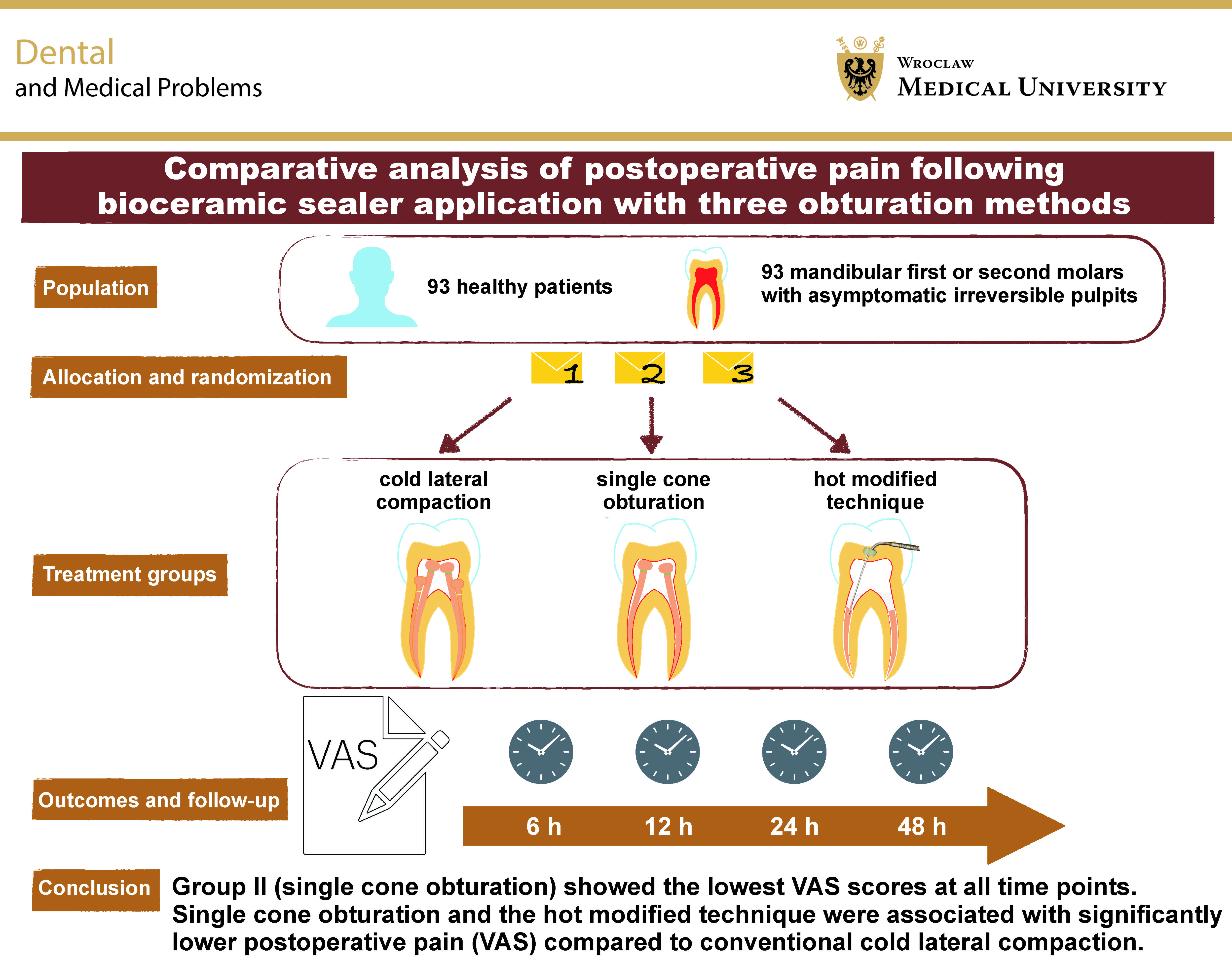
Objectives. This randomized controlled trial aimed to evaluate the efficacy of 3 obturation techniques using a bioceramic sealer (Cerafill RCS®) on postoperative pain in patients with asymptomatic irreversible pulpitis.
Material and methods. Ninety-three patients diagnosed with asymptomatic irreversible pulpitis were randomly allocated to one of three groups according to the obturation technique: cold lateral compaction; single cone obturation; or a hot modified technique. The severity of pain was assessed using a visual analogue scale (VAS) at 6, 12, 24, and 48 h after treatment. The study utilized Kruskal–Wallis and Mann–Whitney U tests to analyze pain scores across groups. Linear regression analysis was performed to identify predictors of postoperative pain.
Results. The sealer-based and hot modified techniques were associated with significantly lower postoperative pain levels compared to cold lateral compaction at all measured time points (p < 0.05). The regression analysis confirmed the obturation technique as a significant predictor of postoperative pain. The hot modified method, in particular, provided the most consistent pain relief, underscoring the potential of advanced obturation methods in enhancing patient recovery and comfort.
Conclusions. The sealer-based and hot modified methods significantly reduced postoperative pain compared to traditional techniques. These findings support the clinical adoption of innovative bioceramic sealer techniques to optimize pain management and patient satisfaction.
Keywords: postoperative pain, randomized controlled trial, root canal therapy, endodontics, bioceramics
Introduction
Endodontic success is generally defined as the resolution or sustained absence of clinical signs and symptoms associated with pulpal or periapical disease following treatment.1
Clinician-reported outcomes, such as tenderness to percussion or palpation, the presence of a sinus tract, increased tooth mobility, periodontal pockets, and radiographic findings, remain central to defining treatment success. Yet, patient-reported outcomes, particularly those concerning pain and overall quality of life, are equally important for a comprehensive evaluation of endodontic effectiveness.2
A comprehensive approach to pain management should consider factors influencing each stage of treatment.3 Several clinical variables have been identified as contributors to intraoperative and postoperative pain, including the choice of irrigating solutions,4 irrigation activation techniques,5, 6 apical extrusion of irrigants,7, 8 flare-ups,9 instrumentation protocols,10, 11 extrusion of debris,12, 13 and the use or omission of occlusal reduction.14 Furthermore, mechanical and procedural factors, such as over-enlargement of the apical foramen,15 lack of apical patency,16 over-instrumentation, instrument kinematics,17, 18 and the physicochemical properties of root canal sealers,19, 20 may significantly influence the onset and severity of postoperative pain.
Postoperative pain remains a prevalent concern in endodontic therapy. It typically decreases substantially within 24 h and rarely persists for more than a week.21, 22 This multifactorial phenomenon arises from mechanical trauma, such as over-instrumentation or extrusion of filling materials, as well as chemical irritation and microbial extrusion of periradicular tissues.23, 24, 25, 26 While systematic reviews have established a robust correlation between root canal instrumentation and postoperative pain,27, 28 limited evidence is available regarding the influence of bioceramic-based obturation techniques on this outcome.29, 30, 31, 32
Achieving a three-dimensional seal of the root canal system is critical, as it prevents the leakage of microorganisms and their byproducts, thereby reducing the likelihood of reinfection and mitigating postoperative discomfort.33, 34 Procedures such as cold lateral compaction, single cone obturation and the hot modified technique differ in methodology, sealing efficacy and potential impact on patient comfort. Conflicting evidence underscores the need for further investigation into the influence of these techniques on postoperative outcomes, particularly when used in conjunction with bioceramic sealers.
Calcium silicate-based sealers (CSBSs), also referred to as bioceramic sealers, including Cerafill RCS® (Prevest DenPro Ltd., Bari Brahmana, India), have garnered significant attention due to the bioactive properties such as hydroxyapatite formation and the ability to promote tissue healing.35, 36, 37 These materials exhibit a high alkaline pH, improved apical sealing properties, and the potential to enhance periapical healing through odontoblastic differentiation and dentin mineralization.36, 37 Although previous studies have reported comparable postoperative pain levels between resin-based and bioceramic sealers,36, 38, 39, 40 further exploration is necessary to elucidate the unique benefits of individual bioceramic sealers, including Cerafill RCS®.
The potential of Cerafill RCS® as a bioceramic root canal sealer supports its inclusion in the present randomized controlled trial. To date, no clinical studies have rigorously evaluated its effectiveness, leaving a significant gap in the literature. Addressing this gap is critical to provide clinicians with robust evidence for optimizing endodontic outcomes. Therefore, the present randomized controlled trial aimed to evaluate postoperative pain associated with the use of Cerafill RCS® in combination with 3 bioceramic-based obturation techniques: cold lateral compaction; single cone obturation; and the hot modified technique. By generating evidence-based recommendations, this research would seek to advance clinical practice in single-visit root canal treatments. The null hypothesis posits that there are no significant differences in postoperative pain scores between the 3 obturation techniques using Cerafill RCS® in patients diagnosed with asymptomatic irreversible pulpitis and undergoing single-visit root canal treatment.
Material and methods
Study protocol
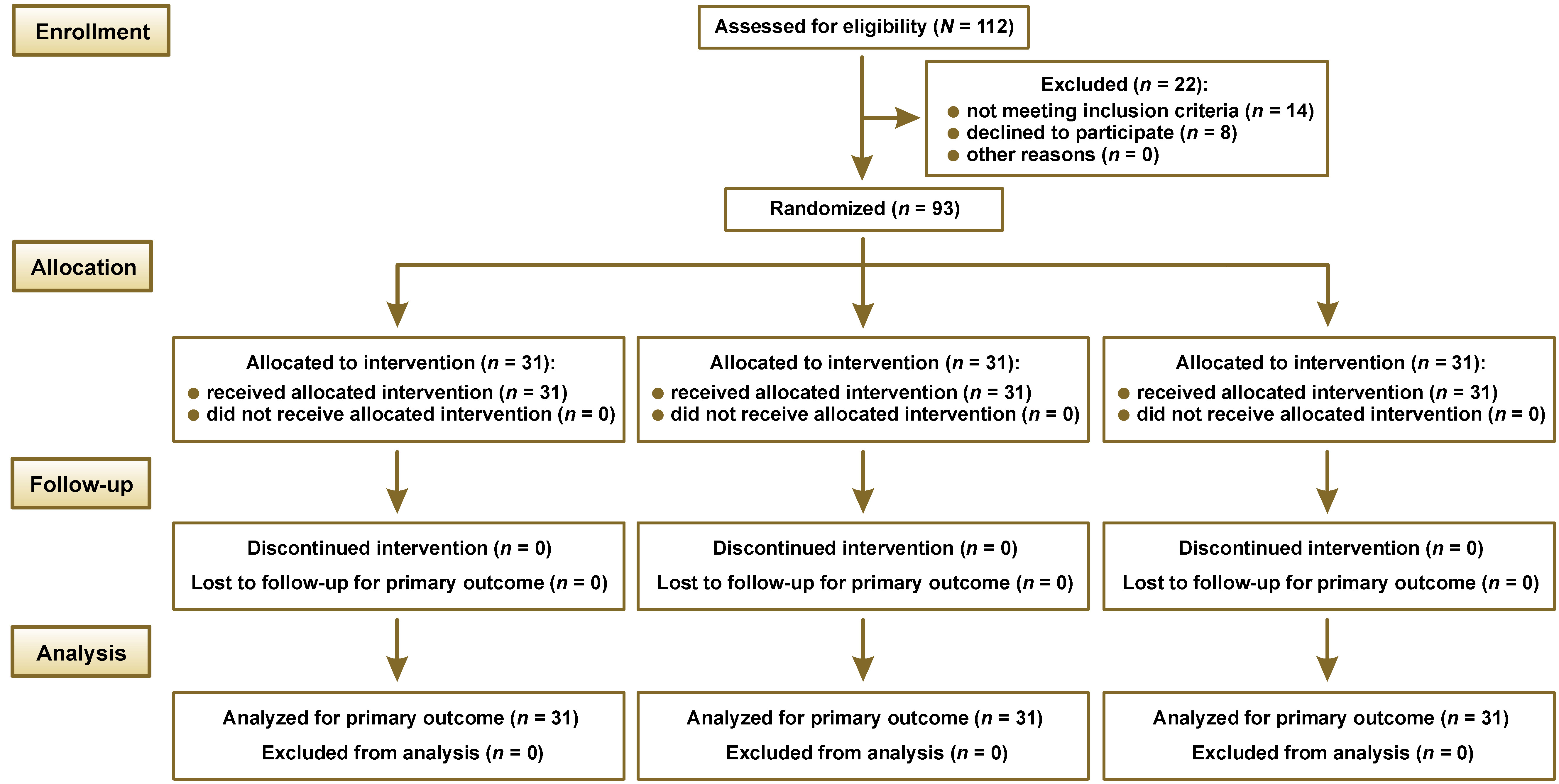
The present study was designed as a prospective, multicenter, randomized, single-blind controlled clinical trial. Ethical approval for the study was obtained from the Institutional Human Ethics Committee of Saveetha Dental College and Hospitals, Chennai, India (approval No. IHEC/SDC/FACULTY/21/ENDO/134), prior to study initiation. Additionally, the study was prospectively registered in the Clinical Trials Registry – India (CTRI) (http://ctri.nic.in; CTRI/2024/10/074776.) Research was conducted at the Mamata Institute of Dental Sciences, Kaloji Narayana Rao University of Health Sciences, Hyderabad, India. The conducted procedures posed minimal risk to participants and were carried out following the principles outlined in the Declaration of Helsinki. The study adhered to the Consolidated Standards of Reporting Trials (CONSORT) 2025 guidelines (Figure 1),41 as well as the Preferred Reporting Items for Randomized Trials in Endodontics (PRIRATE) 2020 guidelines.42
Sample size
The sample size was calculated a priori using the G*Power software, v. 3.0.10, based on data from a previous study.28 Using a one-way analysis of variance (ANOVA) model for 3 independent groups, with an effect size of 1.73 (Cohen’s f), a significance level of 0.05, and a statistical power of 95% (1 – β = 95%, α = 0.05), the required total sample size was determined to be 93 participants (n = 31/group). No adjustments for potential dropout were made.
Inclusion and exclusion criteria
Patients aged between 18 and 60 years with asymptomatic irreversible pulpitis in mandibular first or second molars, without associated periapical pathology, and classified as systemically healthy according to the American Society of Anesthesiologists (ASA) were included in the study. Individuals who were medically compromised or unable to communicate symptoms due to cognitive or psychological impairment, pregnant women, or those receiving antibiotics or analgesics for preoperative pain, as well as patients with incomplete apex formation, calcified canals, periapical abscess, tooth affected by cracks or sinus openings were excluded from the study.
Preoperative assessment
Two calibrated endodontists with comparable clinical experience and proficiency in all obturation techniques performed the entire experimental protocol under an operating microscope (Prima DNT; Labomed Europe, Capelle aan den Ijssel, the Netherlands). Before allocating participants to the operators, an examiner who was not involved in the study charted the preoperative pulpal and periapical status. All patients were preoperatively diagnosed with asymptomatic irreversible pulpitis without associated periapical pathosis, according to the criteria of the American Association of Endodontists (AAE).43 Pulpal diagnosis was confirmed using a cold test (Endo-Ice™ Green; Hygenic Corp., Akron, USA) and electrical pulp stimulation (Vitality Scanner; Kerr Analytic Technology Corp., Redmond, USA). Patient history, including past and present symptoms, was considered prior to inclusion. Patients who exhibited tenderness upon vertical or lateral percussion of teeth or showed periapical pathosis on radiographic examination were excluded from the study. Additionally, individuals whose postoperative radiographs revealed underfilling or overfilling of thermoplasticized gutta-percha of the root canal obturation were excluded from the final analysis.
Participant allocation and randomization
The study followed a single-blind protocol. A computer-generated randomization sequence (https://www.random.org) was used for allocation. The SNOSE (sequentially numbered, opaque, sealed envelopes) technique was implemented for allocation concealment, which concealed the sequence until interventions were assigned. A piece of paper containing a randomized group number was sealed in a dark-colored envelope prepared by a third party. Patients were assigned study numbers as they enrolled in the study. Each envelope was opened after participant enrollment and immediately prior to intervention. Participants were randomly divided into 3 groups (n = 31/group) based on the bioceramic-based obturation technique: group I – cold lateral compaction; group II – single cone obturation; and group III – hot modified technique.
Treatment protocol
After allocation, all participants received a standardized inferior alveolar nerve block with 1.8 mL of 2% lidocaine and 1:200,000 epinephrine (LOX 2%; Neon Laboratories Ltd., Mumbai, India) administered with a 27-gauge long needle. Supplemental doses of the same anesthetic were provided as needed. After achieving profound numbness, the tooth was isolated with a rubber dam, and the access cavity was prepared using sterile carbide burs (Cavity Access Set; Dentsply Maillefer, Ballaigues, Switzerland) and the Endo-Access Burs (size 2; Dentsply Maillefer). Access refinement was performed using the Endo-Z Bur (Dentsply Maillefer) under the operating microscope. Initial canal patency was established with the use of stainless steel K-files (size #10; MANI Inc., Tochigi, Japan), and initial orifice enlargement was carried out using rotary files (ProTaper Gold Shaper X; Dentsply Maillefer). Working length was determined with the use of a specific initial binding file with an apex locator (Root ZX Mini; J. Morita USA, Inc., Irvine, USA) and confirmed radiographically. Subsequently, standardized instrumentation procedures were performed with rotary files (ProTaper Gold Shaper X) using a crown-down technique. Apical enlargement was standardized to three file sizes larger than the initial binding file. Apical patency was maintained throughout the shaping procedure using stainless steel K-files between successive instruments. Each canal was irrigated with 10 mL of 5% NaOCl (HYPOSOL®; Prevest DenPro Ltd.) between each instrument. Irigants were delivered with continuous oscillations using a conventional syringe attached to a flexible root canal irrigation needle (IrriFlex®; Produits Dentaires SA, Vevey, Switzerland), positioned 1 mm short of the working length. After complete instrumentation, canals were flushed with 5 mL of normal saline. Then, 1 mL of 5% NaOCl was activated for 20 s over 3 cycles using an ultrasonic device (VDW Ultra; VDW GmbH, Munich, Germany) with an attached ultrasonic tip (IRRI S; VDW GmbH) at a power setting of 30, placed 1 mm short of the working length. Final irrigation consisted of 4 mL of 5% NaOCl, 5 mL of 17% ethylenediaminetetraacetic acid (EDTA) (EDTA Solution; Prevest DenPro Ltd.) and 5 mL of normal saline. Canals were then dried with paper points. After experimental irrigation, obturation was conducted during a single visit, according to the assigned intervention.
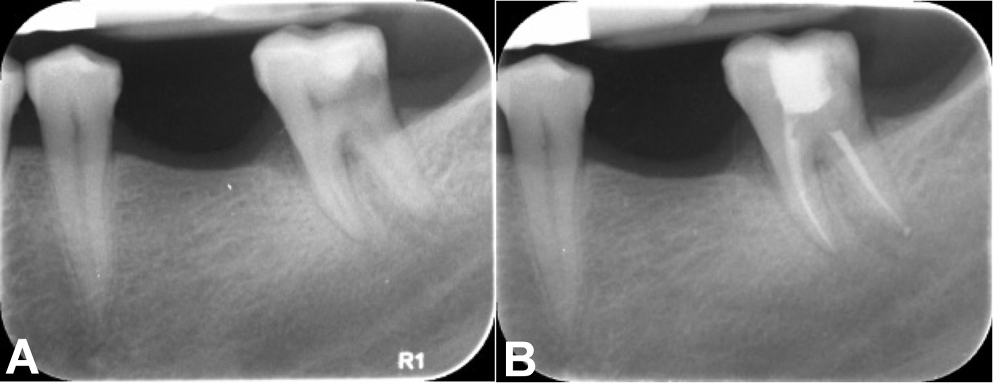
Group I: cold lateral compaction
After root canal debridement, the master cone was verified with an intraoral periapical radiograph. Once the working length was confirmed, the premixed injectable Cerafill RCS® sealer (Prevest DenPro Ltd.) was dispensed onto a paper mixing pad. The master cone (Dentsply Maillefer) was adequately coated with the sealer and placed into the canal at working length. Spreaders of an appropriate size were introduced 1 mm short of the working length to create lateral space for accessory cones. Accessory cones (Dentsply Maillefer) were then coated with the sealer and packed until the spreader penetrated no more than 1–2 mm into the root canal orifice. Before the excision of the accessory cones, an intraoral periapical radiograph was taken to confirm the quality of the seal. If any voids or spaces were detected, additional accessory cones were placed until an adequate seal was obtained. Finally, excess gutta-percha was removed using a heated plugger to 1 mm below the orifice level and condensed (Figure 2).
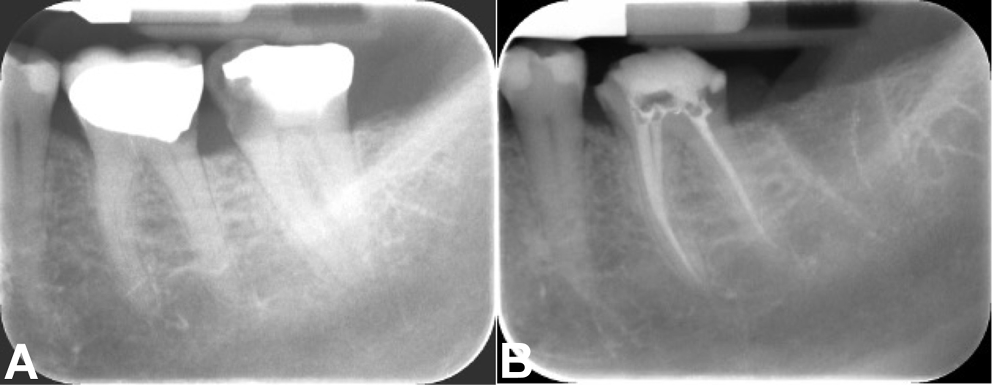
Group II: single cone obturation
Following master cone verification, the premixed Cerafill RCS® sealer was injected into the root canal using flexible syringe injection tips provided by the manufacturer. Before injection, the applicator tip was adjusted to 5–6 mm short of the working length using a rubber stop and calibrated with the Endo-Block (Dentsply Maillefer). The flexible syringe injection tip was then placed into the canal until the rubber stop was reached. The Cerafill RCS® sealer was injected by gently pressing the syringe plunger while withdrawing the tip until the sealer was visible at the root canal orifice. The tip of the master cone was then coated with the bioceramic sealer and inserted carefully to the desired working length. Excess gutta-percha was removed using a heat carrier tip set at 180°C, and the material was condensed to 1 mm below the canal orifice level (Figure 3).
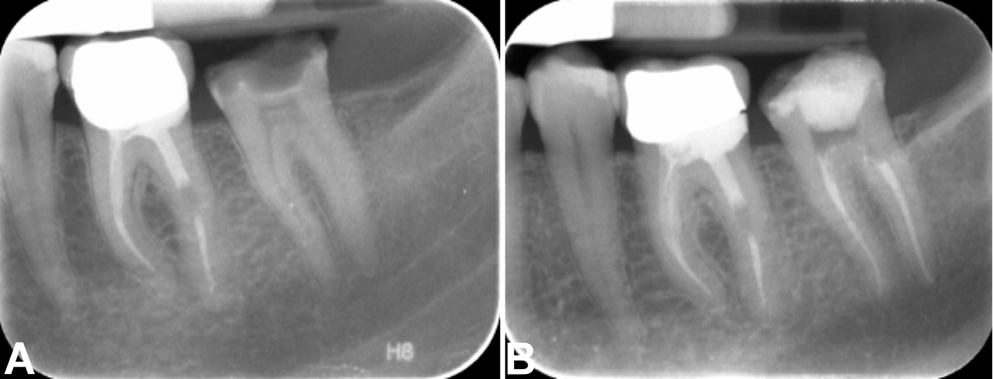
Group III: hot modified technique
The hot modified technique was performed following the protocol described in a previous report.44 After verification of the master cone, the premixed bioceramic sealer (Cerafill RCS®) was injected into the canal using a disposable tip. The master gutta-percha cone was lightly coated with the sealer and inserted to full working length.
A heated plugger set at 180°C was used for downpacking. The plugger was inserted to a depth of 6–10 mm short of the working length and activated for 4 s to thermosoften and compact the gutta-percha in the middle and coronal thirds. Care was taken to avoid disturbing the apical 3–4 mm to preserve the apical seal and prevent sealer extrusion.
The softened gutta-percha was vertically compacted using pre-fitted pluggers. Accessory cones were placed in wide canals to ensure adequate filling. Additional thermoplasticized gutta-percha was added as necessary to fill voids, and the quality of obturation was verified radiographically. Excess gutta-percha was removed to 1 mm below the canal orifice using a heated plugger and vertically compacted to complete the obturation (Figure 4).
All obturation procedures were standardized in duration to approx. 45–50 min per tooth, regardless of group allocation. Following obturation, in all groups, excess sealer was removed using an ultrasonic scaler tip under water irrigation, and the chamber was air-dried. The access cavity was examined under an operating microscope to ensure complete removal of the sealer contents. Radiographs confirmed that no under- or overfilling of thermoplasticized gutta-percha occurred in any treated canal and that all canals had been properly treated. An intraorifice seal was placed using a flowable core build-up composite (Fusion Core DC Flo™; Prevest DenPro Ltd.), and the final core buildup was completed with packable composite restoration (Magma NT™; Prevest DenPro Ltd.) for all the groups.
Evaluation of postoperative pain
All participants received a visual analogue scale (VAS) sheet after the procedure to record pain intensity. No medications were prescribed immediately after treatment. Patients were advised to contact the investigator by telephone if they experienced discomfort and were instructed not to take any medication without prior consultation. If patients reported pain, they were prescribed Aceclofenac. To ensure compliance and accurate data collection, the participants were contacted by telephone at 6, 12, 24, and 48 h after treatment. These follow-up calls served to assess patient status, reinforce completion of the VAS form at each time point, and document pain scores accordingly.
Statistical analysis
The statistical analysis was conducted using the IBM SPSS Statistics for Windows software, v. 21.0 (IBM Corp., Armonk, USA). The analyses were designed to evaluate both inter- and intragroup variations in VAS pain scores. Data normality was assessed using the Shapiro–Wilk test, which indicated a non-normal distribution of VAS scores; therefore, non-parametric tests were applied. The homogeneity of categorical variables such as sex and tooth type across groups was evaluated using the Pearson’s χ2 test. The Kruskal–Wallis test was used to compare pain scores across the 3 groups at each time point (6, 12, 24, and 48 h post-treatment). Wilcoxon signed-rank test was applied for intergroup comparisons of pain scores across successive time points, while the Friedman test was used to assess overall changes over time within each group. Pairwise comparisons between the groups at each time interval were performed using the Mann–Whitney U test. Pain scores were reported as medians and interquartile ranges (IQRs). Linear regression analysis was performed to explore the relationships between patient characteristics, treatment modalities and postoperative pain scores, providing insights into the factors that significantly affected pain outcomes. A p-value <0.05 was considered statistically significant.
Results
Demographic and baseline characteristics
A total of 115 patients were enrolled between January and February 2025. Of these, 14 did not meet the inclusion criteria, and 8 individuals declined to participate, resulting in the exclusion of 22 patients. Finally, 93 patients were randomly allocated into 3 study groups (n = 31/group), all of whom received the intended intervention and were included in the final analysis. No losses to follow-up, exclusions after randomization, or deviations from the prespecified protocol occurred. All outcomes were analyzed in accordance with the registered trial protocol. The mean age of participants was 32.43 ±6.32 years (median: 32; IQR: 28–37). The demographic characteristics of the study population are presented in Table 1. All procedures were performed by 2 calibrated endodontists under standardized conditions using an operating microscope. Radiographic evaluation confirmed obturation fidelity in all cases. No adjunctive medications were administered unless patients reported postoperative pain during follow-up.
VAS scores
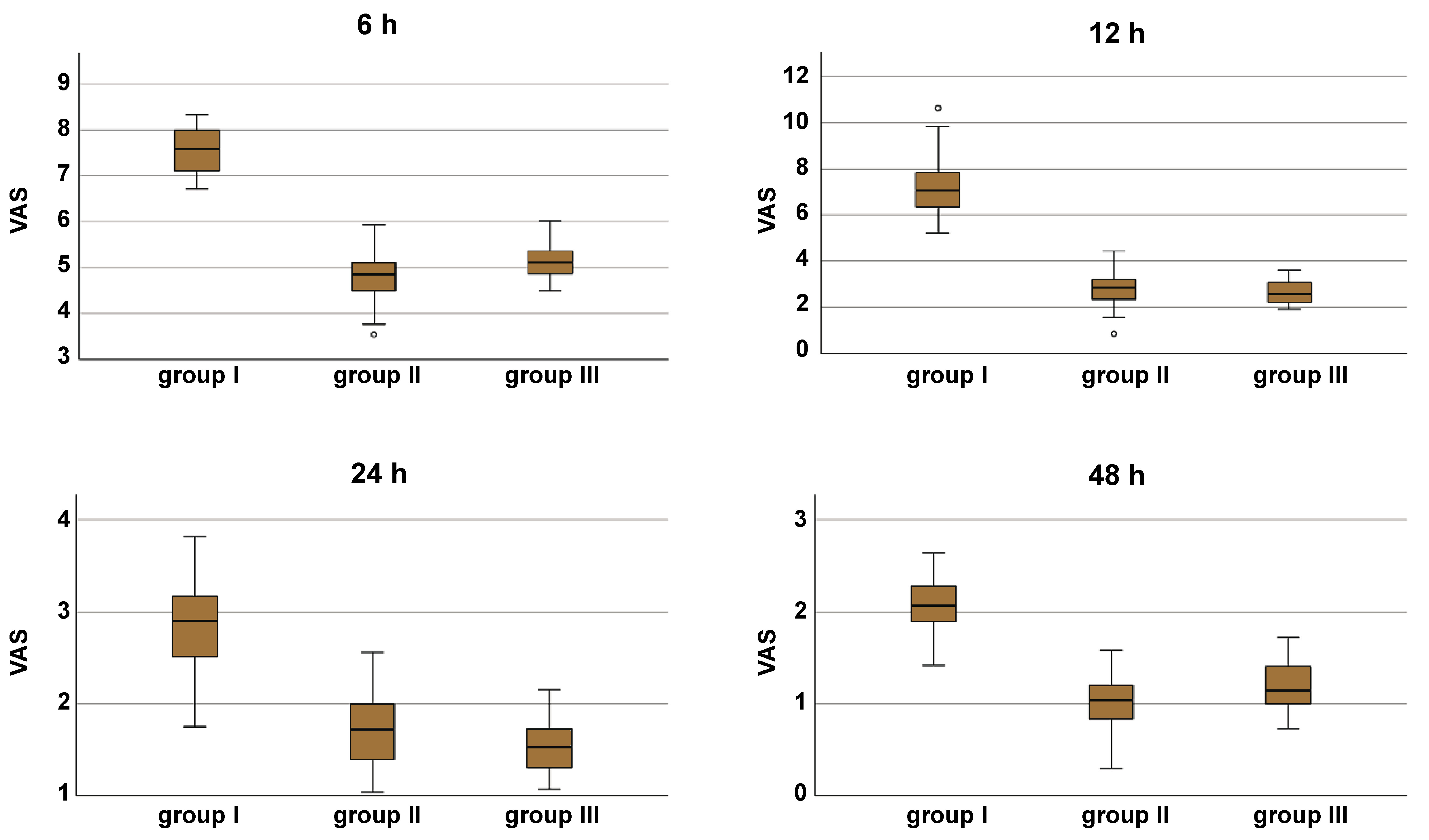
No missing data was noted; all randomized participants completed the follow-up and were included in the primary analysis. VAS scores were assessed at 6, 12, 24, and 48 h post-treatment across all groups. When all groups were considered collectively, the Friedman test demonstrated a significant reduction in VAS scores over time (p < 0.001). A significant decrease in mean VAS scores was also observed within each group across all evaluated time points (p < 0.001) (Table 2). The Kruskal–Wallis test revealed statistically significant differences is VAS scores among the 3 obturation techniques at 6, 12, 24, and 48 h (p < 0.001) (Figure 5).
Intergroup comparisons indicated that groups II and III exhibited significantly lower VAS scores compared to group I at all time points (p < 0.001) (Table 3).
The Wilcoxon signed-rank test demonstrated a significant reduction in pain between successive time intervals (6 h vs. 12 h, 12 h vs. 24 h, and 24 h vs. 48 h) for the overall sample. Intragroup evaluation showed that groups II and III demonstrated significant reductions in VAS scores at each follow-up interval. Group I exhibited a substantial reduction in pain 24 h after treatment (p < 0.001), while no significant differences were observed between 6 h and 12 h (p = 0.131).
Table 4 presents the pairwise comparisons of VAS scores at each time interval. Statistically significant differences were observed at 6, 12, 24, and 48 h, with groups II and III reporting significantly lower pain levels than group I at each time point (p < 0.001). Notably, at 12 h and 24 h, the differences between groups II and III were not significant (p = 0.312 and p = 0.703, respectively), while at 48 h, group II exhibited significantly lower VAS scores compared to group III (p = 0.035).
Influence of sex
Analysis of postoperative pain according to sex revealed no significant differences at 6 h (p = 0.713), 12 h (p = 0.495), 24 h (p = 0.942), or 48 h (p = 0.969).
Predictors of postoperative pain
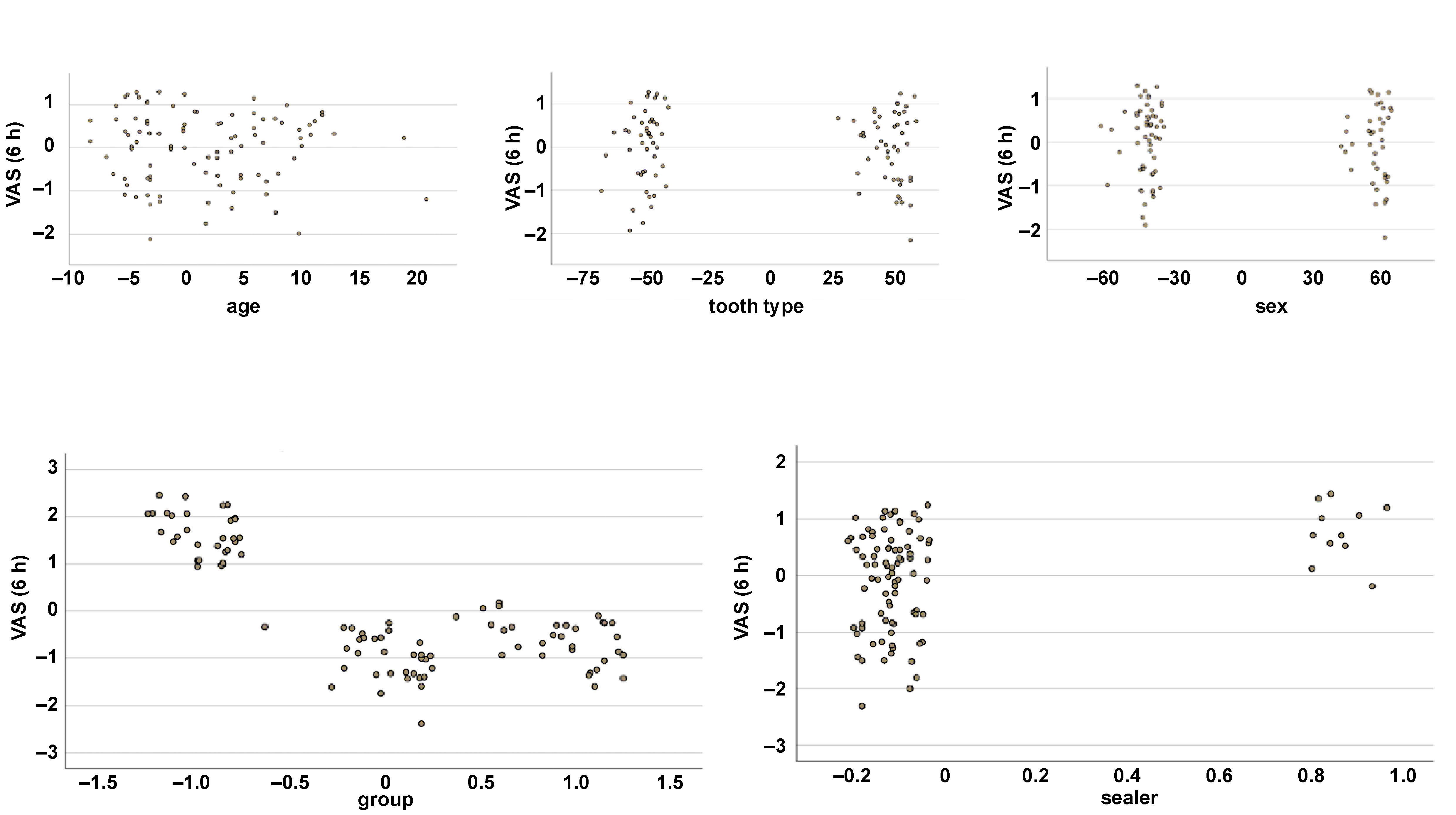
Linear regression analysis indicated that the bioceramic-based obturation technique and sealer extrusion had a significantly negative impact on VAS scores at 6 h (Table 5, Figure 6). At subsequent time points, only the obturation technique remained a significant predictor of postoperative pain, while no other variables showed a statistically significant effect.
Discussion
The current randomized controlled trial evaluated the impact of 3 different bioceramic-based obturation techniques using Cerafill RCS® on postoperative pain in patients with asymptomatic irreversible pulpitis.
The findings demonstrated significant differences in pain reduction among the bioceramic-based obturation techniques, highlighting their clinical relevance in optimizing endodontic outcomes. Moreover, these results align with the current shift toward patient-centered care in endodontics, where minimizing post-treatment discomfort is a key objective. Statistically significant differences in VAS scores were observed between the groups at 6, 12, 24, and 48 h post-treatment (p < 0.05), suggesting that the choice of obturation technique directly influences early postoperative pain. These findings are consistent with previous reports showing a wide range of postoperative pain incidence (3.0–69.3%) following non-surgical root canal treatment.23 Moreover, symptomatic teeth have been reported to exhibit a higher incidence of postoperative pain compared to asymptomatic cases (15.9% vs. 7.1%).24 Therefore, postoperative pain might be considered an important indicator of treatment outcomes.45
Cerafill RCS® has demonstrated superior in vitro properties, including enhanced bioactivity, crystallinity and solubility,46, 47 which may contribute to improved healing and reduced postoperative pain.48 Its handling characteristics and low solubility support the formation of a durable and stable apical seal, thereby minimizing the risk of reinfection. Comparative studies evaluating its performance across obturation techniques have suggested that warm vertical compaction methods may provide superior sealing results when compared to lateral compaction or single cone techniques.46, 47, 49 Furthermore, Cerafill RCS® outperforms other sealers in maintaining excellent flow characteristics and a consistently high alkaline pH, essential for periapical healing.48
In the present study, the intragroup analysis indicated a significant reduction in pain over time within each group (p < 0.001), validating the effectiveness of bioceramic sealers in pain alleviation, probably due to their bioactive properties.35, 36, 37, 42, 46, 47, 50 Moreover, groups II (single cone obturation) and III (hot modified technique) demonstrated significantly lower pain levels compared to group I (cold lateral compaction). These findings are consistent with the study by Martín-González et al.who reported higher pain levels following traditional compaction techniques.32 The authors reported a 55.3% incidence of pain after obturation in subjects treated with cold lateral compaction compared to 44.7% in those treated with thermoplasticized gutta-percha.32 The higher pain levels reported in group I might be attributed to the undue lateral forces exerted on the periodontium.32 Although interappointment flare-ups are uncommon, postoperative pain is frequent even when appropriate treatment is performed.51 Findings of the present study suggest that the hot modified technique (group III) consistently outperformed cold lateral compaction (group I) and sealer-based obturation (group II), not only at early postoperative time points but throughout all follow-up intervals. This was further corroborated by the Mann–Whitney U test results, which emphasized superior outcomes in group III, indicating a more effective management of pain compared to the traditional methods. Although some studies report higher pain levels with carrier-based thermoplastic obturation and lateral compaction compared to back-fill thermoplastic methods,30, 32 others show no significant differences between cold lateral compaction and continuous wave technique.29
The superior efficacy of the hot modified technique in reducing postoperative discomfort is consistent with existing literature, which established that bioceramic sealers paired with warm obturation techniques yield notably lower postoperative pain compared to traditional cold lateral compaction.20 Bioceramic sealers have favorable physical properties, such as reduced porosity and enhanced material adaptability, which are critical factors in minimizing periapical inflammation and associated postoperative symptoms.52 The reduced pain associated with the hot modified technique may be explained by the superior thermoplastic characteristics of gutta-percha employed in this method. By promoting closer adaptation of gutta-percha and sealer to the dentinal walls, this approach minimizes void spaces and reduces the risk of apical microleakage. Consequently, the inflammatory response triggered by extruded materials is significantly mitigated.
Conversely, the increased postoperative pain observed with lateral compaction techniques may be attributed to mechanical stress applied to the root to achieve the compaction and less optimal material adaptation, increasing the risk of sealer extrusion and periapical inflammation.20
Previous studies have shown that factors such as age, sex, pulpal status, tooth type, site, and preoperative pain play a significant role in postoperative pain outcomes.23 In the present study, no significant differences were observed among groups with respect to these variables. Pain perception is a highly subjective experience, modulated by various physical and psychological factors. Furthermore, measuring pain is challenging due to a high potential for error.53 The VAS is a validated and sensitive tool for measuring acute pain,54, 55 therefore, this method was adopted in the present study. The time intervals chosen for pain assessment ranged from 6 h to 48 h, as maximum post-treatment pain typically occurs within this period.21 Comorbidities such as pain before obturation were not reported among all 3 groups.
Linear regression analysis further confirmed that the bioceramic-based obturation technique was a significant predictor of postoperative pain, with the hot modified technique showing the most favorable outcomes. This statistical insight highlights the clinical efficacy of the method, aligning with recent advancements in endodontic materials and techniques that prioritize patient outcomes and procedural innovations.
According to the present study, it is recommended that clinicians consider adopting sealer-based and hot modified techniques over traditional cold lateral compaction. The demonstrated efficacy of these methods in reducing postoperative pain can significantly improve patient satisfaction and treatment acceptance, which are crucial in clinical settings. This recommendation is evidenced by superior clinical and radiographic success rates with bioceramic sealers used in single cone techniques.33, 56 This is the first trial focusing on assessing the real-time clinical benefits of the hot modified technique and investigating postoperative pain in patients undergoing single-visit root canal treatment using different bioceramic-based obturation methods. However, this study focused exclusively on asymptomatic irreversible pulpitis, which limited its applicability to symptomatic patients, who often represent a substantial portion of endodontic cases. Future research should consider subjects with varying degrees of symptomatic pulpitis and apical periodontitis. Additionally, exploring other bioceramic sealers could provide broader insights and validate the generalizability of current findings across different materials.
Conclusions
Single cone obturation and the hot modified technique were associated with significantly lower postoperative pain compared to conventional cold lateral compaction. These findings suggest that the adoption of these techniques may improve patient outcomes, such as pain control and long-term treatment results. Future research involving symptomatic cases and a broader range of materials is recommended to strengthen the generalizability of these results.
Trial registration
The study was prospectively registered in the Clinical Trials Registry – India (CTRI) (http://ctri.nic.in; CTRI/2024/10/074776).
Ethics approval and consent to participate
The conducted procedures posed minimal risk to participants and were carried out following the principles outlined in the Declaration of Helsinki. All personal data was treated with strict anonymity and confidentiality. Ethical approval for the study was obtained from the Institutional Human Ethics Committee of Saveetha Dental College and Hospitals, Chennai, India (approval No. IHEC/SDC/FACULTY/21/ENDO/134), prior to study initiation.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.