Abstract
Background. Obstructive sleep apnea (OSA) is a prevalent chronic condition characterized by recurrent episodes of upper airway narrowing or collapse during sleep. Obstructive sleep apnea is associated with various health issues, including cardiovascular disease and metabolic disorders. The cervico-cranio-mandibular complex (CCMC) plays a critical role in musculoskeletal functions such as mouth opening and head stabilization; however, its relationship with OSA remains insufficiently explored.
Objectives. The aim of the study was to evaluate the association between cervico-cranio-mandibular musculoskeletal function and OSA severity, based on the hypothesis that dysfunctions within the CCMC are associated with greater OSA severity.
Material and methods. A pilot cross-sectional study was conducted involving 32 patients with symptoms of OSA. The participants underwent assessment of cervico-cranio-mandibular musculoskeletal function and an ambulatory sleep study to determine OSA severity. Spearman’s tests were used to analyze the relationships between cervico-cranio-mandibular musculoskeletal parameters and OSA severity.
Results. Significant negative correlations were observed between cervical range of motion (ROM) (flexion, left rotation, right/left lateral flexion) and OSA severity. The strongest correlation was identified for cervical movement in the frontal plane (r = –0.607, p < 0.001), especially among females (r = –0.772, p < 0.01). A positive relationship was found between mouth-opening muscle endurance and OSA severity in male participants (r = 0.445, p < 0.05).
Conclusions. This preliminary study highlights potential associations between specific musculoskeletal characteristics of the CCMC and OSA severity, with notable sex-specific patterns. These findings may contribute to the development of targeted screening approaches and support individualized physiotherapeutic interventions.
Keywords: neck pain, posture, temporomandibular joint, obstructive sleep apnea, craniomandibular disorders
Introduction
Obstructive sleep apnea (OSA) is a common and underdiagnosed condition characterized by recurrent episodes of upper airway obstruction during sleep, leading to intermittent hypoxia, sleep fragmentation and elevated sympathetic nervous system activity.1 These disruptions contribute to the development of cardiovascular disease,2 metabolic disorders,3 cognitive impairments,4 and reduced quality of life.5 Obstructive sleep apnea is strongly associated with hypertension, atrial fibrillation, type 2 diabetes mellitus, stroke, and myocardial infarction.6
While anatomical factors such as obesity, macroglossia, retrognathia, malocclusion, hyoid position, and tonsillar hypertrophy are well-established contributors to OSA,1, 7, 8, 9 the role of musculoskeletal function in maintaining upper airway patency remains less understood. The cervico-cranio-mandibular complex (CCMC), including the cervical spine, mandible and associated musculature, may influence airway stability through biomechanical and neuromuscular mechanisms. For example, cervical spine posture can affect pharyngeal wall tension,8 while masticatory muscle activity may alter hyoid bone and tongue positioning.1, 7, 10
Dysfunction or imbalance within the CCMC may compromise airway patency, even in the absence of overt anatomical abnormalities. Yet, clinical research on the musculoskeletal contribution to OSA is limited.11, 12 In light of this gap, conservative interventions such as physical therapy may offer potential therapeutic value.
Furthermore, sex-related differences in craniofacial anatomy, fat distribution and neuromuscular control suggest the presence of distinct OSA phenotypes. Women may rely more on accessory musculature and often present with atypical symptoms.10
The present pilot study investigated whether the neuromuscular function and mobility of the CCMC are associated with the severity of OSA. We hypothesized that reduced cervical mobility, altered posture, and imbalances in jaw muscle function would correlate with higher apnea–hypopnea index (AHI) values, with possible sex-based differences.
Material and methods
Study design and participants
This pilot cross-sectional observational study was conducted between August 2023 and May 2024. A convenience sample of 32 participants (20 males, 12 females), aged 18–70 years, was recruited through referrals from an otolaryngologist based on clinical suspicion of OSA. All participants underwent a comprehensive musculoskeletal evaluation followed by an ambulatory sleep study.
The inclusion criteria were as follows: 18–70 years of age (adult population); body mass index (BMI) ≤32 (to minimize a clear confounding factor); and referral for an overnight sleep study due to suspected OSA (e.g., excessive daytime sleepiness, loud snoring, morning headaches, unrefreshing sleep, or frequent nocturnal arousals). The exclusion criteria included prior treatment for OSA, a diagnosis of temporomandibular disorders based on the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD),13 subjective complaints of significant neck pain within the past 30 days, surgical interventions involving the CCMC, or neurological conditions affecting motor control. Participants who had received recent Botox treatment for bruxism or experienced technical issues during the sleep study were also excluded.
The study was approved by the Helsinki Committee of Soroka Medical Center, Ben-Gurion University of the Negev, Be’er-Sheva, Israel (approval No. SOR-0183-22). Written informed consent was obtained from all participants. A reliability protocol was implemented for mouth-opening and mouth-closing muscle performance measurements. The study protocol was retrospectively registered in the Open Science Framework (OSF) (https://doi.org/10.17605/OSF.IO/RFN75).
Musculoskeletal evaluation of the cervico-cranio-mandibular complex
Two trained physiotherapists (AW and DG) performed all physical assessments. Both examiners were blinded to the results of the sleep study to minimize assessment bias.
Mouth opening
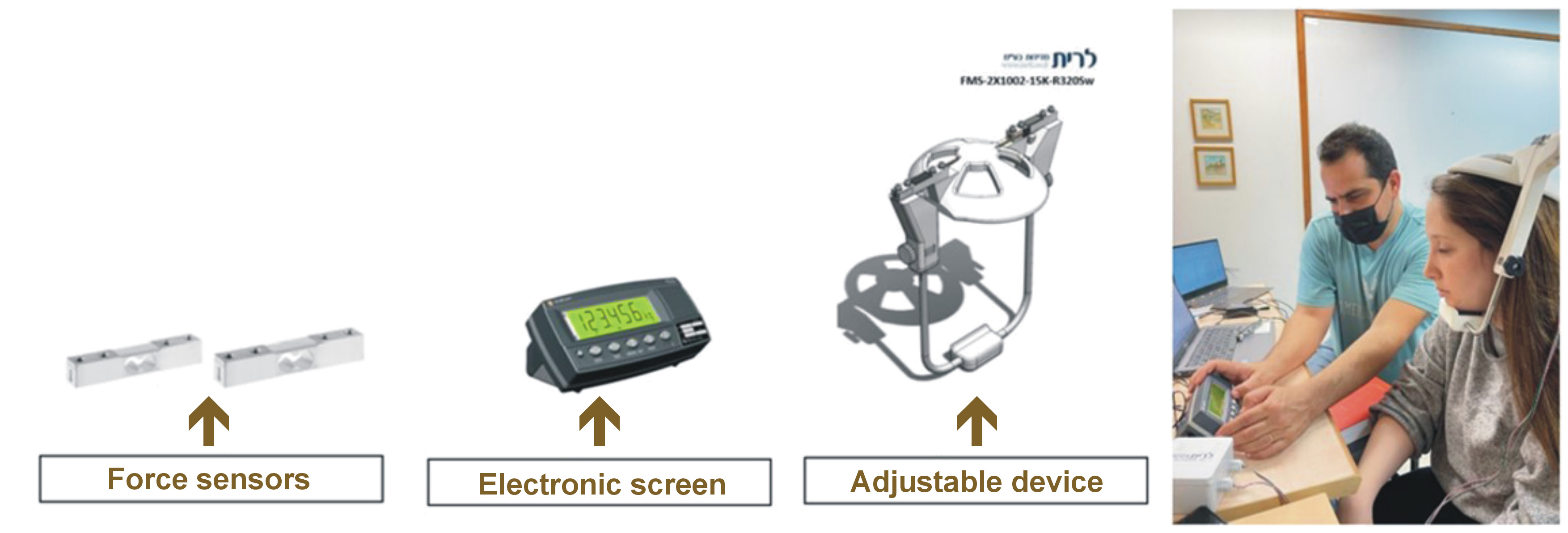
Isometric strength during mandibular depression and protrusion was assessed using a novel, adjustable extraoral force measurement device developed by the research team (Figure 1). The device incorporated 2 piezoresistive force transducers (FMS-2X1002-15K-R3205w; Vishay, Chartres, France), each with a maximum load of 150 N, providing digital force output in real time. In the present study, intra- and inter-rater reliability of the device were evaluated.
The participants were seated upright with full back support and fitted with the device adjusted to allow 20 mm of mouth opening. Based on a previous protocol,14 maximal pain-free isometric mouth-opening strength was measured 3 times. The maximal force achieved in 3 s was recorded and averaged. The verbal instruction for the participant was: “On the count of three, open your mouth as wide as you can”. Afterward, based on the same protocol,14 an endurance test was performed. The participants were required to maintain 30% of their maximal force (to fatigue the mouth openers) using screen-based biofeedback (±10% margin). For instance, for a maximal force of 10 kg, the endurance target was 3 kg (range 2–4 kg). The maximal pain-free time duration within this target range was recorded using a stopwatch, following a brief practice period. The verbal instruction was: “Maintain your mouth open at this target level as long as you can”.
Mouth closing
Based on a previous protocol,14 bite force was measured using a piezoresistive transducer-based device (iBite Pro®; Loadstar® Sensors, Fremont, USA), with a maximum load of 1,000 N and digital output displayed in real time.
The participants were seated upright with full back support. Maximal pain-free bite force was recorded over 3 trials and averaged. An endurance test was followed to assess fatiguability, during which participants maintained 30% of their maximal bite force using screen-based biofeedback (±10% margin). After a brief practice, the pain-free endurance time within the target range was measured using a stopwatch. Final outcomes included maximal strength [kg] and endurance time [s] for both mouth-opening and mouth-closing tests.
Reliability assessment for mouth-opening and mouth-closing tests
Intra-rater reliability was assessed by repeating the measurements on the following day by the same examiner, while inter-rater reliability involved 2 examiners performing measurements 1 h apart.
Neck muscle performance
The neck flexor muscle endurance test assessed craniocervical flexor function.15 Based on the protocol,15 the assessment was performed in a hook-lying position. The participants were instructed to retract their chin, lift their head approx. 2.5 cm above the surface while maintaining the chin tuck, and hold the position as long as possible. The test ended when the chin tuck was lost or when the head rested on the examiner’s hand for more than 1 s.
Cervical range of motion
Cervical range of motion (ROM), which is often altered in association with cervical disorders,16 was measured using a cervical ROM device (Performance Attainment Associates, Roseville, USA), a commonly used tool for the measurement of cervical spine mobility.17 The participants were seated upright with the trunk supported against the backrest and feet flat on the floor. Six physiological movements, namely flexion, extension, right and left lateral flexion, and right and left rotation, were assessed in a randomized order. Each movement was repeated 3 times with 30-s rest intervals. The mean value of the 3 measurements, expressed in degrees, was recorded for each direction.
Flexion–rotation test
The flexion–rotation test (FRT)18 was used to assess upper cervical (C1–C2) mobility. In the supine position, the participants performed maximal head rotation to each side while maintaining full cervical flexion. Range limitations and asymmetries were documented.
Assessment of head and neck posture
The assessment of head and neck posture was conducted using craniocervical angle analysis based on standardized lateral photographs.19
Sleep study
The severity of OSA was assessed using a validated home sleep testing device (WatchPAT® 300; ZOLL® Itamar®, Caesarea, Israel) that records peripheral arterial tone (PAT), heart rate and oxygen saturation.20 The main outcome was the AHI, representing the number of apneas and hypopneas per hour of sleep. The participants wore the device overnight at home, which consisted of a wrist unit, a finger probe and a chest sensor. The data was interpreted by the Sleep-Awake Laboratory of Soroka Medical Center, Ben-Gurion University of the Negev, Be’er-Sheva, Israel.
Statistical analysis
The data was analyzed using the IBM SPSS Statistics for Windows software, v. 22.0 (IBM Corp., Armonk, USA). Descriptive statistics were calculated as mean (M) and standard deviation (SD) values. The Shapiro–Wilk test was used to assess normality of data distribution. One-way analysis of variance (ANOVA) was utilized to compare demographic and CCMC variables across OSA severity groups. Spearman’s correlation coefficients were calculated to evaluate associations between CCMC function and OSA severity. Effect sizes were interpreted according to Cohen’s guidelines for Pearson’s r, as follows: 0.10 (small); 0.30 (medium); and 0.50 (large). Intra- and inter-rater reliability for mouth-opening and mouth-closing muscle measurements were evaluated using intraclass correlation coefficients (ICCs), based on a two-way mixed-effects model (consistency type) and 95% confidence intervals (95% CIs). The level of statistical significance was set at p < 0.05. As an exploratory study, the sample size of 32 participants was considered consistent with pilot study recommendations prioritizing feasibility and trend identification over statistical power.21
Results
The study included 32 participants (20 males and 12 females). The mean age was 47.4 ±14.7 years (range: 22–68 years), and the mean BMI was 26.75 ±2.53 kg/m2 (range: 22.9–31.9 kg/m2). Based on the AHI values, 28% of the participants were classified as having mild OSA, 41% as having moderate OSA, 12% as having severe OSA, while 19% had AHI values <5. All outcome measures were successfully obtained for all participants, ensuring a complete dataset for analysis.
Mouth-opening muscle strength and endurance demonstrated excellent reliability (intra-rater ICC: 0.87–0.91 and 0.87–0.88, respectively; inter-rater ICC: 0.90 and 0.89, respectively). In contrast, mouth-closing muscle strength exhibited poor intra-rater reliability (ICC: 0.07–0.20, M: 0.13) but high inter-rater reliability (ICC: 0.92). Mouth-closing muscle endurance demonstrated moderate to excellent reliability (intra-rater ICC: 0.65–0.93; inter-rater ICC: 0.85).
Among male subjects, mouth-opening muscle endurance was positively correlated with the AHI (r = 0.445, p < 0.05), indicating a medium effect size. Additionally, the endurance ratio of jaw-opening to jaw-closing muscles was negatively correlated with the AHI (r = –0.469, p < 0.05), also reflecting a medium effect size. These results imply that a relative imbalance favoring mouth-opening muscles may reflect or contribute to reduced airway stability. Specifically, higher mouth-opening muscle endurance relative to mouth-closing muscles was observed in males with moderate to severe OSA.
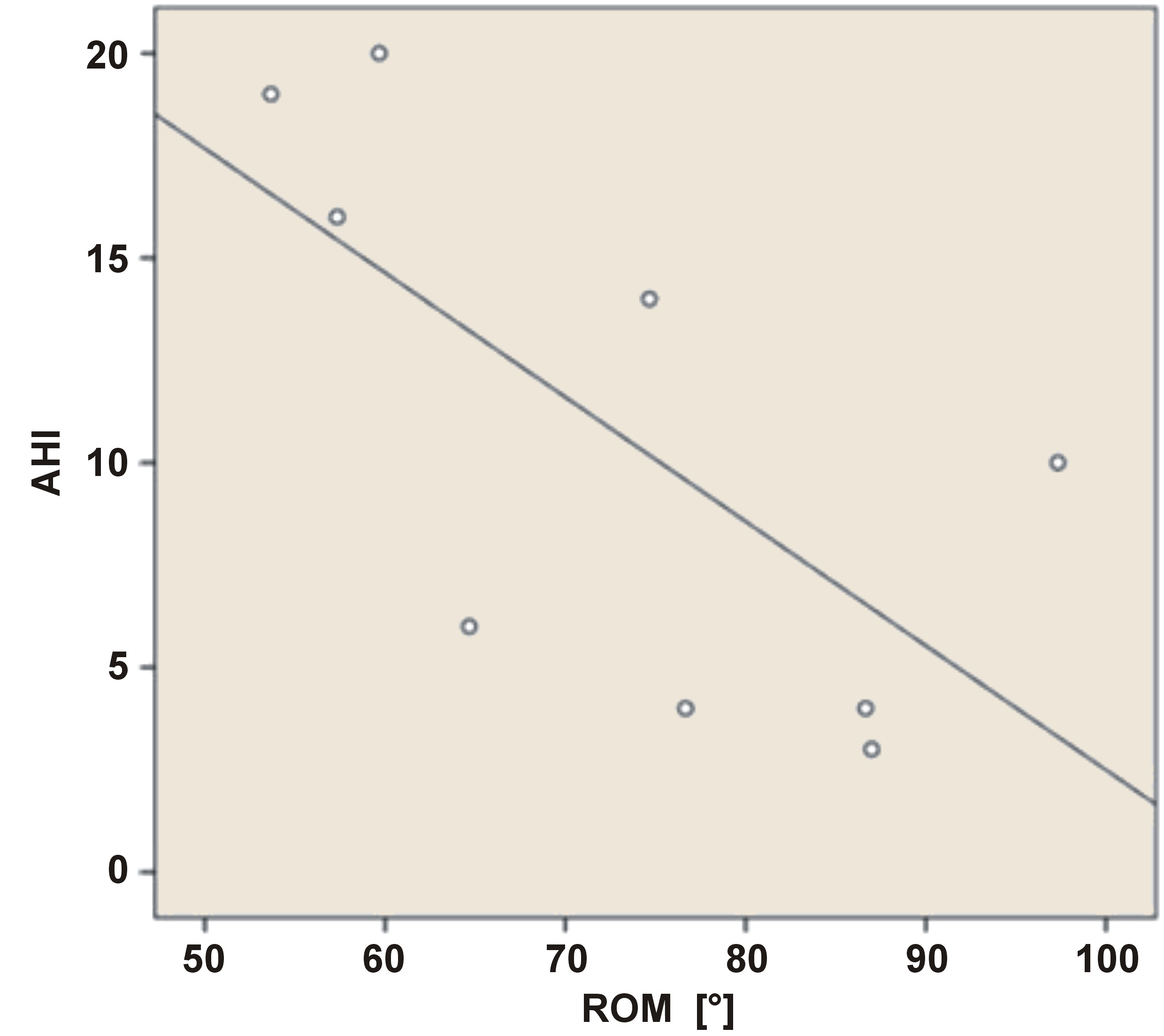
Cervical ROM, particularly in the frontal plane (lateral flexion to both sides), was significantly and strongly inversely correlated with the AHI (r = –0.607, p < 0.001). In female participants, the correlation was even stronger (r = –0.772, p < 0.01), indicating a large effect size and suggesting that reduced cervical mobility may disproportionately affect women’s airway function during sleep (Figure 2).
No significant associations were identified between the AHI and neck muscle performance, head and neck posture and the FRT.
Discussion
This preliminary study explored the relationship between musculoskeletal function of the CCMC and the severity of OSA. The findings demonstrated a strong negative correlation between restricted cervical ROM, particularly lateral flexion, and OSA severity, especially in females. These findings support the hypothesis that musculoskeletal dysfunction within the CCMC may be related to OSA severity. The observed relationship may be bidirectional. Limited cervical ROM could impair compensatory head and neck movements during apneic events, while chronic overactivation of accessory respiratory muscles (e.g., scalenes) may lead to musculoskeletal adaptations and subsequent ROM restrictions. This feedback loop highlights the clinical relevance of assessing cervical function in individuals with OSA.
Contrary to our expectations, no significant correlations were found between sagittal plane ROM or forward head posture and OSA severity. These outcomes may be partially explained by the relatively low BMI of the study sample, which may reduce mechanical strain on cervical structures.
Sex-specific analyses revealed stronger correlations between limited frontal plane ROM and OSA severity in women, aligning with evidence that women experience different symptom patterns and musculoskeletal involvement in OSA.10 These findings emphasize the importance of sex-specific diagnostic and therapeutic considerations.
Unexpectedly, in male participants, greater mouth-opening muscle endurance was associated with increased OSA severity. A possible explanation is habitual mouth opening during sleep as a compensatory response to upper airway obstruction, leading to chronic overuse and increased endurance of the mouth-opening muscles. This overuse may result in hypertrophy of the supra- and infrahyoid muscles, potentially narrowing the pharyngeal airway and contributing to increased airway resistance. These findings suggest a paradoxical adaptation that may exacerbate OSA severity. Further research is warranted to evaluate these hypotheses and clarify the underlying mechanisms.
Limitations
Several limitations should be acknowledged. First, the small sample size and absence of a control group, characteristic of preliminary studies, limit the generalizability of the findings. Second, the cross-sectional design precludes the establishment of causal relationships between CCMC function and OSA severity. Longitudinal studies are needed to determine whether interventions aimed at improving CCMC function can effectively reduce OSA severity. Additionally, mandibular ROM was not assessed, which may have limited our ability to fully characterize the functional status of the craniomandibular complex.
Conclusions
This preliminary investigation indicates that specific musculoskeletal characteristics of the CCMC are associated with OSA severity, particularly limitations in cervical lateral flexion and jaw muscle imbalances. The observed sex-specific patterns further support the importance of personalized assessment strategies. While preliminary, these findings open new directions for clinical screening and physiotherapy-based interventions.
Ethics approval and consent to participate
The study was approved by the Helsinki Committee of Soroka Medical Center, Ben-Gurion University of the Negev, Be’er-Sheva, Israel (approval No. SOR-0183-22). Written informed consent was obtained from all participants.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Written informed consent was obtained from all participants for the publication of any potentially identifiable data included in this article.
Use of AI and AI-assisted technologies
ChatGPT (OpenAI, San Francisco, USA) was used to improve the clarity and grammar of the manuscript. The authors reviewed and edited the final version and take full responsibility for the content.