Abstract
Background. The close anatomical relationship between root apices and the mandibular canal (MC) may be of clinical importance in preventing inferior alveolar nerve (IAN) injury during the root canal treatment (RCT) of mandibular molars.
Objectives. The aim of the present study was to evaluate the impact of the mean distance between MC and the root apices of mandibular first and second molars on the risk of IAN injury during RCT in a Turkish subpopulation.
Material and methods. Cone-beam computed tomography (CBCT) images of 934 patients were evaluated. Mandibular molars were examined, and parasagittal sections were used to measure the shortest linear distance between the root apex and the superior cortical border of MC.
Results. The mesial and distal roots were closer to MC in the 18–25-year age group and in females (p < 0.05). Overall, 284 (10.5%) mesial roots were in intimate contact with or invading MC, and 80 (3.0%) were located very close to MC (<1.00 mm). Among distal roots, 328 (12.2%) were in intimate contact with or invading MC, 76 (2.8%) were very close to MC, and 2,288 (85.0%) were distant from MC.
Conclusions. The risk of IAN injury during RCT was higher for the distal roots of second molar teeth, especially in the age group of 18–25 years and in female patients.
Keywords: root canal treatment, inferior alveolar nerve, cone-beam computed tomography, mandibular canal, nerve injury
Introduction
The mandibular canal (MC) extends from the mandibular foramen to the mental foramen and contains the inferior alveolar artery, inferior alveolar vein, and inferior alveolar nerve (IAN).1 Paresthesia, dysesthesia, anesthesia, pain, and lip numbness may occur following IAN injury.2, 3 In a study investigating IAN neurosensory disturbances, 19.6% of injuries occurred during dental procedures, and 35.3% of these were reported after endodontic treatment.4 To prevent such complications, extreme caution is required during root canal treatment (RCT) and surgical procedures in the posterior mandible because of the close anatomical relationship between the superior border of MC and the apices of mandibular molars.5 Additionally, reduced microarchitectural bone density may create an unimpeded pathway for mechanical and chemical irritants to pass from the root apex to IAN during RCT.6
During non-surgical RCT, temporary or permanent IAN injury may occur as a result of over-instrumentation, inaccurate working length determination, the extrusion of irrigating solutions, or the over-extension of root canal obturation materials.7, 8, 9, 10, 11 Root canal sealers, which may exhibit neurotoxic properties before setting, can also contribute to nerve injury.12, 13 In addition, intracanal medicaments may cause nerve damage, and materials such as gutta-percha and paper points have been reported to injure IAN through direct mechanical contact.14 Furthermore, thermal injury may occur when warm obturation techniques are employed.15 To minimize these adverse effects and reduce the risk of IAN injury, meticulous care must be taken to avoid the extrusion of materials beyond the apical foramen during RCT.
Cone-beam computed tomography (CBCT) provides three-dimensional (3D) imaging with a moderate radiation dose.16 Numerous studies have demonstrated the value of CBCT in evaluating relationships among anatomical structures.17, 18 A limited number of investigations have specifically assessed the spatial relationship between root apices and IAN.19, 20, 21 Additionally, certain anatomical variations – such as C-shaped canals, dens invaginatus, radix entomolaris, and talon cusps – have been reported to show ethnic predilections.22, 23, 24, 25, 26 Therefore, variations in the anatomical course and position of IAN may also be expected among different ethnic populations.
The aim of this study was to assess the mean distance between MC and the root apices of mandibular first and second molars in a Turkish subpopulation. The close anatomical relationship between root apices and MC may be of clinical importance in preventing IAN injury during the RCT of mandibular molars.
Material and methods
This study was approved by the ethics committee of Biruni University, Istanbul, Turkey (2020/36-16). In total, 1,244 CBCT scans obtained from patients between January 2019 and December 2019, and saved in the database of the Department of Oral and Maxillofacial Radiology were evaluated.
Eligibility criteria
The inclusion criteria were the presence of at least one fully erupted molar with completely formed roots. The exclusion criteria comprised molars with open apices or severe external root resorption; anatomical variations, such as fusion, taurodontism or radix entomolaris; and CBCT images with artifacts that precluded the accurate visualization of MC or measurement of the distance between root apices and MC.
In total, 934 CBCT scans met the inclusion criteria. The age and sex of the participants were also recorded from the patient files.
Image assessment
A GALILEOS® Comfort Plus CBCT unit (Dentsply Sirona, Bensheim, Germany) was used to acquire the volumetric data, and the images were analyzed using the Sidexis software (Dentsply Sirona). The imaging parameters were as follows: voxel size – 0.25 mm; tube voltage – 98 kV; and field of view (FoV) – 15 cm.
The CBCT images were evaluated independently by a radiologist and an endodontist, each with at least 5 years of clinical experience. The course of MC was manually delineated, and measurements were performed by both examiners. As the diameter of MC may vary, the software canal-marking tool, which applies a fixed diameter, was used for all CBCT examinations to ensure standardization. The same CBCT unit and software system were used throughout the study.
Prior to the main assessment, the examiners underwent calibration using a set of randomly selected CBCT scans (N = 70) that were not included in the study sample. Following calibration, all images were evaluated, and any discrepancies were resolved by discussion until consensus was reached. The obtained Cohen’s kappa coefficient indicated very good inter-observer agreement (κ = 0.87).27 All evaluations were performed on an Asus Pro A4310-BB158M All in One PC (ASUSTeK Computer Inc., Taipei, Taiwan) equipped with a high-definition, wide-screen LED monitor (resolution: 1,600 × 900 pixels) under dim ambient lighting conditions.
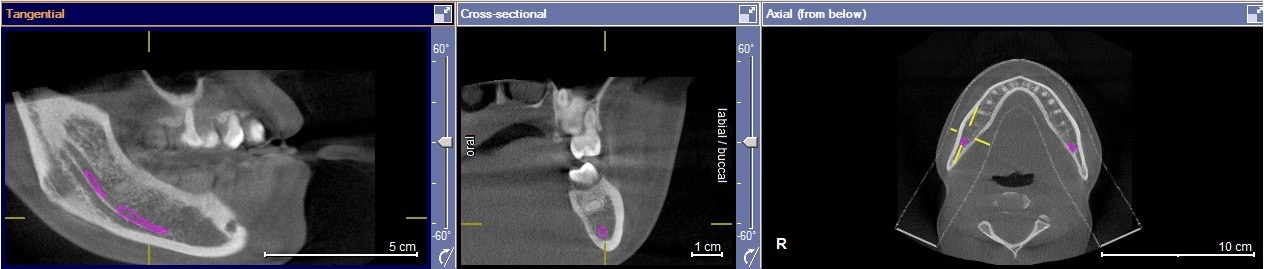
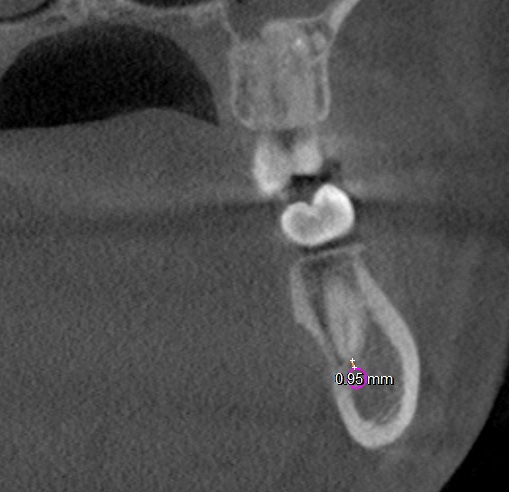
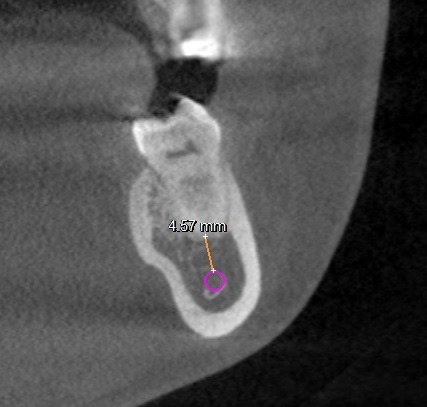
All molar teeth were evaluated in 3 planes (sagittal, axial and coronal) to determine the shortest linear distance between the root apex and the superior cortical border of MC (Figure 1). Distances <1.00 mm were classified as very close to MC (Figure 2).28 Distances ≥1.00 mm were considered distant from MC (Figure 3).28 When the root apex was in intimate contact with or invading MC, the distance was recorded as 0 mm (Figure 4).
The patients were categorized into the following age groups: 18–25 years; 26–35 years; 36–45 years; 46–55 years; 56–65 years; and >65 years. The potential effects of age and sex were subsequently analyzed.
Statistical analysis
Statistical analysis was performed using IBM SPSS Statistics for Windows, v. 22.0 (IBM Corp., Armonk, USA). The normality of the data was assessed using the Kolmogorov–Smirnov and Shapiro–Wilk tests, which indicated that the parameters were normally distributed. Qualitative data were compared using the one-sample χ2 test. The relationships between the distance from root apices to MC and age or sex were analyzed using Student’s t test for independent samples. One-way analysis of variance (ANOVA) was employed to compare parameters across multiple age groups. For comparisons between mesial and distal root apices, the paired-samples t test was used. Statistical significance was set at p < 0.05.
Results
In total, 934 CBCT scans were examined from 442 men (47.3%) and 492 women (52.7%). The patients’ age ranged from 18 to 76 years, with a mean of 37.7 +13.6 years. In total, 1,162 first and 1,530 second molar teeth (5,384 roots of 2,692 teeth) were evaluated. The distances between root apices and MC according to sex and tooth type are shown in Table 1.
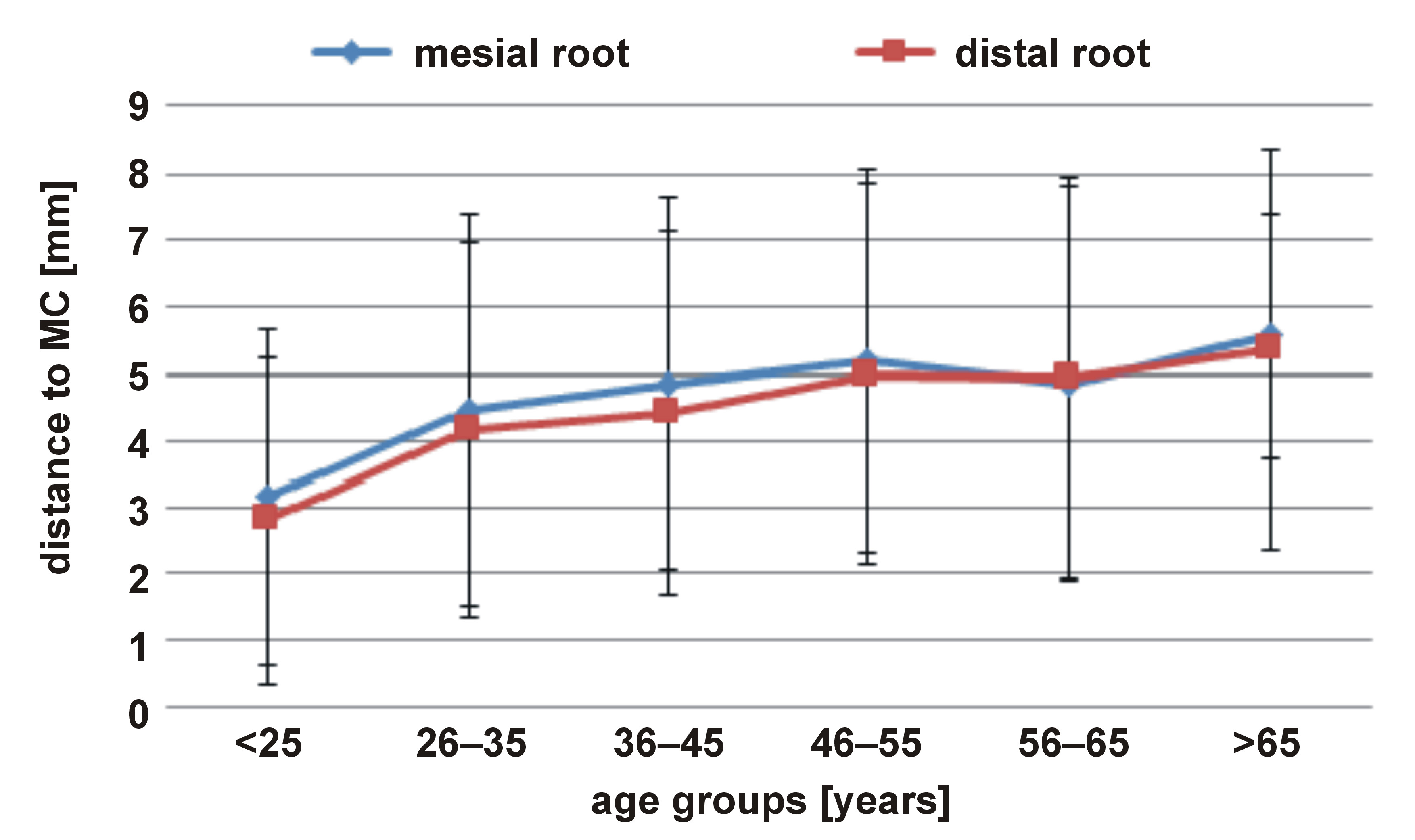
In terms of the mean distance, mesial and distal roots were closer to MC in the 18–25-year age group as compared to other age groups (p < 0.05). Mesial roots in the 26–35-year age group were significantly closer to MC than in the 46–55-year age group (p < 0.05). Similarly, distal roots in the 26–35-year age group were significantly closer to MC than in the 46–55- and 56–65-year age groups (p < 0.05). In addition, in terms of both mesial and distal roots, the mean distance in the 36–45-year age group was significantly shorter as compared to the 46–55-year age group (p < 0.05) (Table 2, Figure 5). With respect to sex, both mesial and distal root apices were significantly closer to MC in females than in males (p < 0.05) (Table 2).
Overall, 284 (10.5%) mesial roots were in intimate contact with or invading MC, 80 (3.0%) were very close to MC, and 2,328 (86.5%) were distant from MC. A total of 328 (12.2%) distal roots were in intimate contact with or invading MC, 76 (2.8%) were very close to MC, and 2,288 (85.0%) were distant from MC (Table 3).
In the comparison of the mean distances of the mesial and distal root apices of first and second molars to MC, the distal roots of first and second molars were closer to MC than mesial roots (p < 0.05) (Table 4).
Discussion
Only a limited number of studies have investigated the relationship between root apices and MC from an endodontic perspective, using CBCT.29, 30 These studies measured the distance between root apices and MC in mandibular molars, and reported that the distal roots of second molars were in the most intimate contact with MC, followed by the mesial roots of second molars.29, 30 Kim et al. previously confirmed the reliability and accuracy of CBCT for measuring the proximity between anatomical structures.31 Therefore, the present study utilized CBCT images to evaluate the relationship between the root apices of first and second molars and MC in a selected subpopulation.
In the current study, the shortest distance between root apices and MC was observed in the 18–25-year age group. Similarly, Bürklein et al. reported that the distance between MC and root apices increases with age.21 These findings may be attributed to the continued growth of the facial skeleton during young adulthood.21, 28, 31, 32, 33, 34
Consistent with several previous studies,21, 35 the present results demonstrated shorter distances between root apices and MC in females as compared to males. This finding suggests that the risk of IAN damage may be greater in females than in males.8, 36 Females generally have smaller body dimensions than males, which may account for the reduced distance between root apices and MC observed in women.
Among the molar teeth examined, MC was located closer to the mesial and distal root apices of second molars than to those of first molars. Furthermore, in both first and second molars, distal roots were closer to MC than mesial roots. These findings are consistent with previous research.19, 20 This anatomical proximity may help explain the higher incidence of paresthesia reported after the endodontic treatment of second molars.37
The results of the present study demonstrated that the distal roots of second molars were not only the closest to MC, but also exhibited the highest percentage of intimate contact with or invasion of MC. Additionally, 11.4% of the evaluated mandibular molars had root apices that were in intimate contact with or invading MC. Consistent with these findings, Chong et al.19 and Oliveira et al.38found intimate associations between MC and root apices in more than 8% and 50% of cases, respectively. In contrast, Lvovsky et al. reported that 3.4% of the roots assessed in their CBCT study were in intimate contact with MC.39 These discrepancies among studies may be attributable to differences in genetic background and ethnicity across the populations examined.
The findings regarding the proximity of root apices to MC have important clinical implications. They indicate that the extrusion of irrigating solutions or filling materials, as well as over-instrumentation, may result in iatrogenic injury to IAN.40, 41 Therefore, the accurate determination of the working length is essential not only to minimize the risk of IAN injury, but also to ensure the success of endodontic treatment, particularly in cases where root apices are in intimate contact with or invade MC. As suggested in previous research, the use of new-generation apex locators in combination with conventional radiographic techniques may provide more accurate working length determination than either method used alone.42
Symptoms indicative of IAN injury may include acute pain or paresthesia, and can progress to inflammation and edema.43, 44 Contemporary endodontic practice emphasizes minimally invasive approaches supported by magnification and enhanced illumination systems.45 These modern techniques may be beneficial in the management of cases involving IAN injury following RCT.46, 47
In an analysis of 134 CBCT scans, Chong et al. reported that MC was located ≤3 mm from root apices in 54.8% of cases.19 However, the authors did not explain the rationale for selecting ≤3 mm as the reference threshold. In the present study, a distance of <1 mm was defined as ‘very close’, based on previous reports indicating that the accuracy of electronic apex locators ranges from 90% to 100% within ±1 mm of the apical foramen.39, 48, 49 The recommended technique when using an electronic apex locator is to advance the instrument to the apical foramen until the apex is indicated, and then withdraw it 0.5–1 mm coronally.50 However, in cases where the root apex is in intimate contact with MC, this approach may increase the risk of nerve injury.
Limitations
Although the risk of IAN injury during RCT is greatest when root apices invade MC, the risk remains considerable in cases of intimate contact. For this reason, the roots invading MC and those in intimate contact with it were categorized together in the present study. This approach may be regarded as a limitation.
One of the inclusion criteria was the presence of at least one molar tooth. However, when the adjacent molar is missing, the remaining molar may undergo mesio-distal inclination over time. Such positional changes could have influenced the measured mean distances, and therefore represent an additional limitation. Future studies may address this issue by including only cases in which both first and second molars are present bilaterally.
Furthermore, factors such as ethnicity and certain systemic medical conditions may influence the risk of IAN injury during RCT. Endodontic procedures should therefore be performed with particular caution in populations reported to have shorter distances between root apices and MC, as well as in patients with medical conditions that may impair healing.
Conclusions
We conclude that the shortest distance between root apices and MC is observed in the distal roots of second molars, particularly in patients aged 18–25 years and in female individuals. Cases in which root apices are in intimate contact with or invade MC are representing a clinically relevant anatomical finding.
CBCT imaging, which clearly demonstrates the relationship between anatomical structures without superimposition, may serve as a valuable tool for identifying high-risk cases and minimizing the likelihood of iatrogenic IAN injury.
Ethics approval and consent to participate
This study was approved by the ethics committee of Biruni University, Istanbul, Turkey (2020/36-16).
Data availability
The datasets supporting the findings of the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.