Abstract
Background. The coronavirus disease 2019 (COVID-19) pandemic has had a profound impact on people’s daily lives, resulting in lifestyle changes, social distancing, isolation, as well as economic consequences. An evaluation of the effects of COVID-19 on oral health is necessary.
Objectives. The aim of the study was to evaluate the effects of fixed orthodontic treatment on periodontal health and quality of life in adult patients.
Material and methods. Due to the COVID-19 pandemic, the study methodology was based on a questionnaire consisting of 20 items addressed to patients undergoing orthodontic treatment. The questions concerned the frequency and duration of toothbrushing, brushing techniques as well as the use of auxiliary means of oral hygiene, with the objective of drawing conclusions regarding the oral health of this patient population. Additionally, 5 items adapted from the Oral Health Impact Profile-5 (OHIP-5) were included, asking subjects how frequently they had experienced specific problems during orthodontic treatment.
Results. The oral health of adult patients undergoing orthodontic treatment was influenced by the technique, frequency and means of toothbrushing. During fixed orthodontic treatment, pathological changes in periodontal tissues were often observed (23.6–56.4%), along with other conditions influencing patients’ quality of life (10.2–81.3%).
Conclusions. Early diagnosis of periodontal conditions during orthodontic treatment is essential for treatment success. Orthodontists should instruct patients on appropriate oral hygiene practices and on detecting changes in periodontal status, as well as should recommend periodontal consultation when needed. Orthodontic treatment in adult patients, through esthetic and functional improvement, should lead to an improvement in psychosocial wellbeing and an increase in quality of life.
Keywords: quality of life, oral health, esthetics, orthodontic treatment, periodontal structures
Introduction
Orthodontic treatment has increasingly been applied to improve esthetic appearance in adult patients. Orthodontic treatment is used to stabilize occlusion and modify tooth position, if necessary. These procedures must be performed professionally, as inadequate treatment may lead to functional impairments, including difficulties in speech.1, 2 The aim of orthodontic treatment is to obtain esthetically acceptable results, functional occlusion and appropriate tooth movement, i.e., the interaction between the teeth and the periodontal tissues.3, 4 Previous studies have demonstrated that educating parents in oral and periodontal hygiene can lead to less dental and periodontal complications during orthodontic treatment.1, 2, 3, 4, 5 However, regular professional consultations are essential to prevent complex orthodontic–periodontal conditions.1, 2, 3, 4, 5 Dental braces are commonly used to correct tooth misalignment,4, 5 and various prophylactic measures have been introduced to improve the quality of orthodontic treatment.6, 7, 8
Early detection of periodontal conditions is essential for successful orthodontic therapy. Therefore, comprehensive periodontal examinations should be performed before, during and after treatment, including the assessment of the plaque index (PI), papillary bleeding index (PBI), periodontal pocket depth (PD), and radiographic evaluation.2, 9, 10
Patients should be instructed to maintain proper oral hygiene and effective plaque control, and clinicians should carefully monitor their patients’ health.7, 8, 9, 10, 11 In adult patients, radiological examination aimed at detecting carious lesions and bone or root resorption should be performed at least once a year. The benefits of brushing teeth twice a day and using an ultrasonic toothbrush12 or an oscillating-rotating power toothbrush13 over a manual toothbrush have been demonstrated, particularly when combined with appropriate brushing techniques14 and regular interdental cleaning.11, 15 To protect gingival tissues and reduce bacterial load, chlorhexidine may be administered in gel16 or mouthwash form.17
If clinical or radiologic examinations reveal pathological changes in superficial or deep periodontal structures, patients should be referred to a periodontology specialist for a consultation. Orthodontic treatment should be initiated only in the presence of an intact or reduced periodontium, as treatment in the presence of pre-existing periodontal lesions may exacerbate existing lesions and compromise outcomes.
Before initiating orthodontic treatment, clinicians must ensure that patients are capable of maintaining consistent and efficient oral hygiene practices. If adequate plaque control cannot be achieved, treatment should be postponed until satisfactory oral hygiene is established. Patient awareness regarding oral health maintenance is essential for achieving optimal treatment results.
The aim of the present study was to evaluate the effects of fixed orthodontic treatment on periodontal health and quality of life in adult patients, to assess potential changes in periodontal structures, and to examine how orthodontists address these issues in clinical practice.
Material and methods
Due to the restrictions associated with the coronavirus disease 2019 (COVID-19) pandemic, this study was conducted using a questionnaire. The questionnaire consisted of 20 items and was designed to be easily understood by participants. The target population comprised adult patients who were currently undergoing or had previously undergone fixed orthodontic treatment with brackets on one or both dental arches. The first part of the questionnaire included questions about the frequency and duration of toothbrushing, brushing techniques, and the use of auxiliary oral hygiene aids. Given the lack of clinical examinations, additional questions were included to allow indirect assessment of periodontal health. To improve comprehensibility, colloquial expressions were used where appropriate (e.g., “growth in volume of the gums” for gingival edema of bacterial cause or “bad breath” for halitosis). Additionally, 5 items adapted from the Oral Health Impact Profile-5 (OHIP-5) were incorporated. Participants indicated the frequency of experiencing each problem (functional limitation, physical pain, psychological discomfort, physical disability, social disability) during orthodontic treatment using a five-point Likert scale, as follows: 0 – never; 1 – hardly ever; 2 –occasionally; 3 – fairly often; and 4 – very often. In addition to questions evaluating the effects of orthodontic treatment, the questionnaire included items assessing the clinical measures undertaken by orthodontists in response to observed changes in periodontal structures.
A total of 165 patients of both sexes, aged between 19 and 58 years, from Târgu Mureș and Sibiu, Romania, completed the questionnaire. Based on the previous studies,2, 9 the examination protocol presented in Table 1 was adopted.
Results
Of the 165 respondents, 139 (84.2%) were female and 26 (15.8%) were male. Ninety-one participants (55.2%) had completed their orthodontic treatment and reported the duration of therapy.
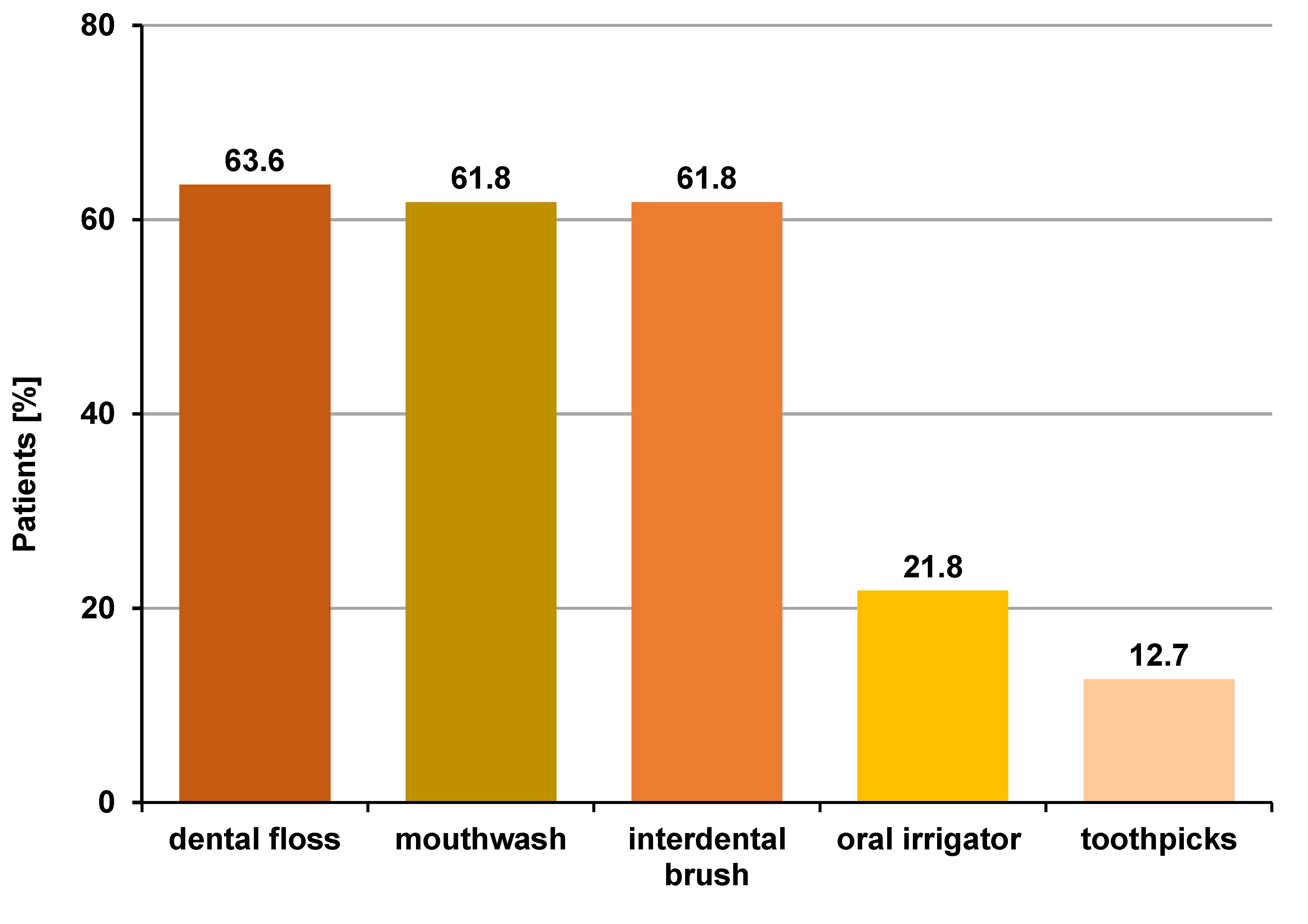
Regarding oral hygiene practices, 108 patients (65.5%) used a manual toothbrush, 48 (29.1%) used an orthodontic toothbrush and 51 (30.9%) used an electric toothbrush. Most participants (126 (76.4%)) reported brushing their teeth twice a day, 33 (20.0%) brushed after every meal and 6 (3.6%) brushed once daily. In terms of brushing techniques, 6 patients (3.6%) used horizontal movements, 33 (20.0%) brushed vertically, 57 (34.5%) used circular movements, and 69 (41.8%) applied a combined technique. With respect to auxiliary means of removing oral biofilm, 105 individuals (63.6%) used dental floss, 102 (61.8%) – mouthwash, 102 (61.8%) – interdental brush, 36 (21.8%) – oral irrigator, and 21 (12.7%) – toothpicks (Figure 1).
Orthodontic treatment was reported to make oral hygiene maintenance difficult by 96 patients (58.2%). However, 126 participants (76.4%) stated that they improved their oral hygiene techniques and plaque control measures during orthodontic treatment.
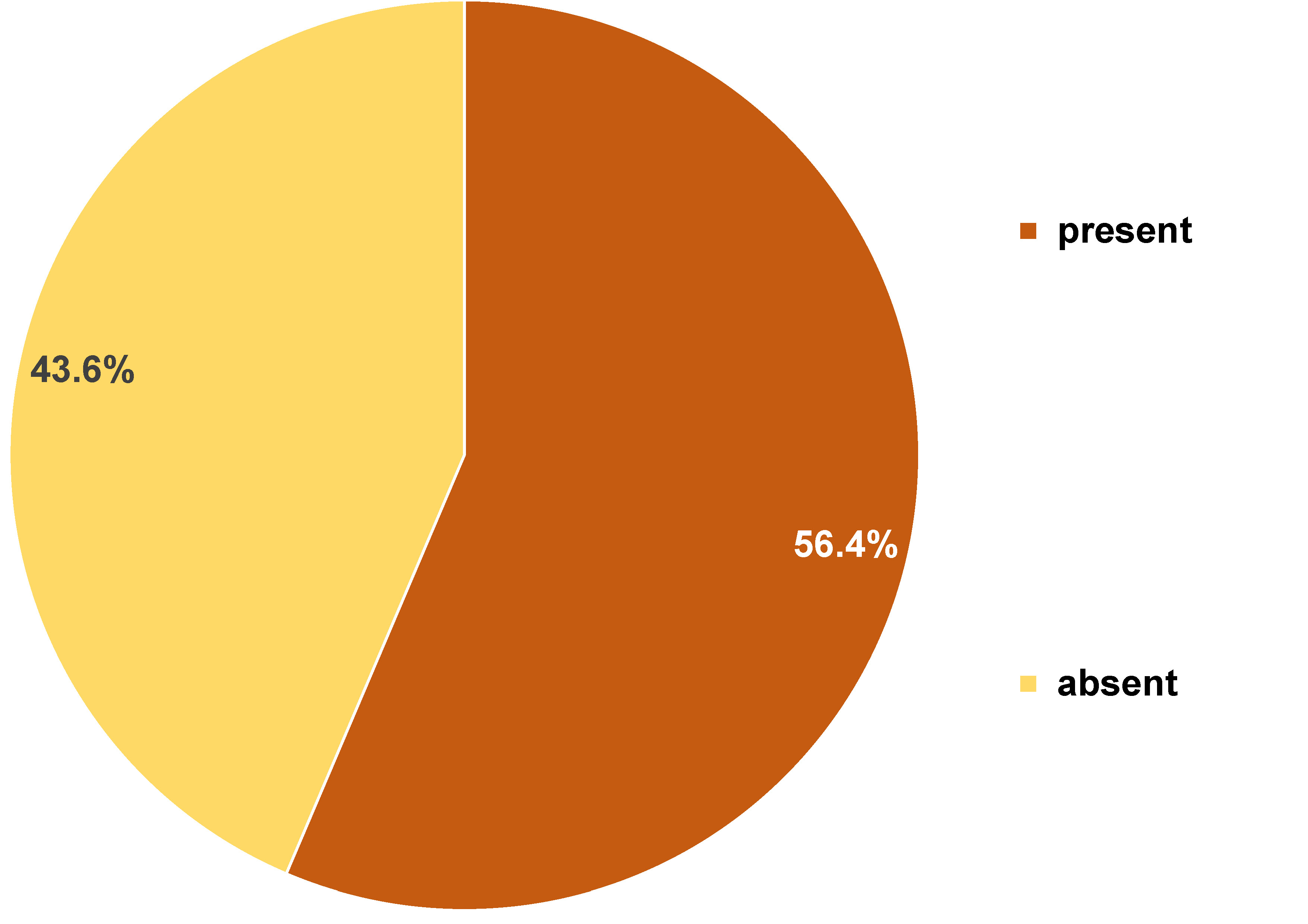
Over the course of treatment, 90 patients (54.5%) observed changes in the color of their gingiva to red, 85 (51.5%) reported increased gingival volume, 39 (23.6%) experienced gingival retraction, and 93 (56.4%) participants reported spontaneous bleeding or bleeding during brushing (Figure 2).
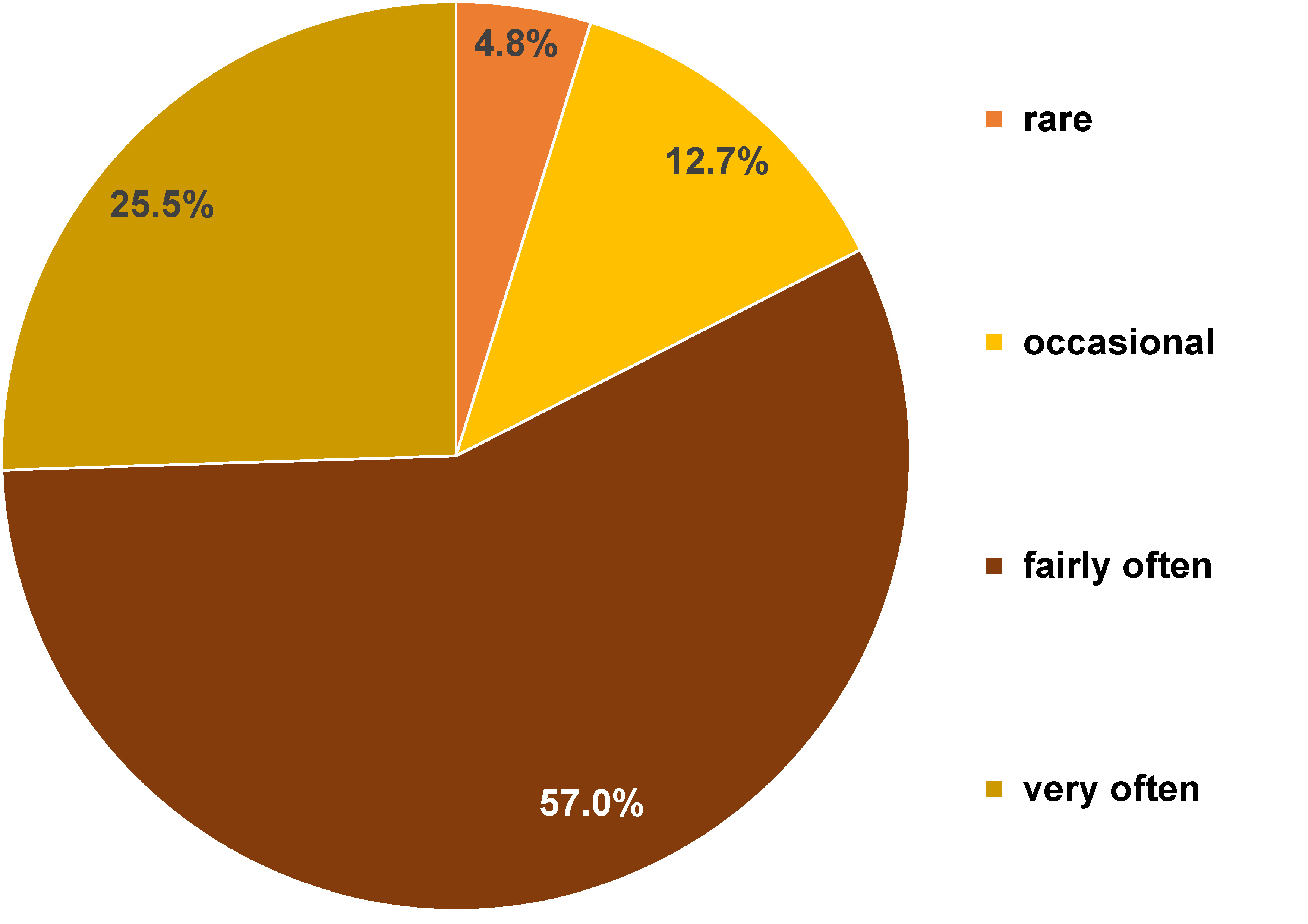
Sixty-six (40.0%) patients noticed the accumulation of calculus during treatment and underwent scaling. In response to the question “Have you had difficulty chewing certain foods because of orthodontic treatment?”, participants answered as follows: never (1 (0.6%)); hardly ever (4 (2.4%)); occasionally (15 (9.1%)); fairly often (134 (81.2%)); and very often (11 (6.7%)). Pain, secondary to orthodontic treatment, was reported as follows: hardly ever (8 (4.8%)); occasionally (21 (12.7%)); fairly often (94 (57.0%)); and very often (42 (25.5%)) (Figure 3).
For the question “Have you felt that food had less flavor because of fixed orthodontic treatment?”, the responses were: never (23 (13.9%)); hardly ever (42 (25.5%)); occasionally (67 (40.6%)); fairly often (22 (13.3%)); and very often (11 (6.7%)).
When asked whether they felt uncomfortable about the appearance of their teeth, mouth or dentures, participants responded as follows: never (51 (30.9%)); hardly ever (34 (20.6%)); occasionally (38 (23.0%)); fairly often (17 (10.3%)); and very often (25 (15.2%)). Regarding difficulty performing usual daily activities because of orthodontic treatment, the answers were: never (18 (10.9%)); hardly ever (47 (28.5%)); occasionally (53 (32.1%)); fairly often (38 (23.0%)); and very often (9 (5.5%)).
Among patients who reported anatomical or functional changes in periodontal structures during orthodontic treatment, 48 (29.1%) stated that these changes were noted or managed by their orthodontist. In addition, 9 patients (5.5%) reported being referred to or treated by a periodontology specialist before or during orthodontic treatment, as recommended by their orthodontist.
Discussion
By analyzing the responses to the questionnaire, we were able to assess oral health status of adult patients undergoing orthodontic treatment. The occurrence of pathological changes in the gingiva during orthodontic therapy is closely associated with the quality of oral hygiene practices. Therefore, the questionnaire included several items addressing brushing techniques and auxiliary oral hygiene measures.
In the present study, the majority of participants used a manual toothbrush (65.5%), while 30.9% used an electric toothbrush. Gingival color changes were reported by 54.5% of patients, gingival volume growth by 51.5%, gingival retractions by 23.6%, and spontaneous bleeding or bleeding during toothbrushing by 56.4%. These gingival alterations were more frequently reported by individuals who used electric toothbrushes.
The efficiency of manual toothbrushing compared to electric toothbrushing was assessed by evaluating the PI and gingival inflammation before and after 30 days of brushing.6 The authors concluded that manual toothbrushes were more effective than ultrasonic toothbrushes in removing plaque around orthodontic appliances, although no significant difference in gingival status were observed. Other studies have reported that electric toothbrushing may be superior, although differences in plaque removal are not significant.18, 19, 20
Most participants in the present study reported brushing their teeth after major meals (33 (20.0%)), two times a day (126 (76.4%)) or once a day (6 (3.6%)), indicating a generally high level of oral hygiene awareness. A similar study performed by Pandey et al. showed that 63% of patients undergoing orthodontic treatment brush their teeth once per day, 26% brush twice a day, and 11% – three times a day.7
Our results also showed that patients who used horizontal or combined brushing techniques experience gingival inflammation more frequently that those using vertical movements. Given the lack of consensus regarding optimal brushing techniques, Nassar et al. compared horizontal, Stillman and Bass methods in 30 adult patients over 9 months and found that the Bass technique was most effective in reducing PI and gingival inflammation in patients with fixed orthodontic appliances.9
Of the patients who responded to our questionnaire, 105 (63.6%) used dental floss, 102 (61.8%) – mouthwash, 102 (61.8%) – interdental brush, 36 (21.8%) – oral irrigator, and 21 (12.7%) – toothpicks. Individuals who used auxiliary oral hygiene aids reported fewer inflammatory gingival changes, suggesting improved plaque control. Previous studies have shown that combining manual and interdental brushing provides better plaque control and reduces gingival inflammation compared with manual brushing alone.15
Bock et al. compared cylindrical and cylindro-conical interdental brushes and found significant reductions in plaque levels with both types, but no significant difference was observed between them.12
Patients undergoing fixed orthodontic treatment are particularly susceptible to gingival inflammation due to difficulties in mechanical plaque removal. Therefore, these individuals would benefit from the use of mouthwashes. Chlorhexidine-based products are widely used to reduce oral bacterial load and prevent or treat some forms of gingivitis and periodontitis.16
Mazzoleni et al. observed that the water jet of the oral irrigator does not significantly improve the efficiency of oral hygiene in patients with orthodontic treatment. However, these patients did not present the traditional aggravation of periodontal status throughout the entire orthodontic treatment.17 Oral irrigators represent useful adjuncts for reducing gingival inflammation despite their limited effects on plaque accumulation.21 In our study, most participants (76.4%) reported an enhancement in their oral hygiene practices during orthodontic treatment. Petrauskiene et al. noted significant modifications in oral hygiene habits among patients with braces, while the majority of patients wearing removable orthodontic apparatus did not change their habits.2
Orthodontic treatment may improve periodontal status, but adverse effects during therapy are relatively frequent. In our sample, 85 patients observed the increase in gingival volume and 39 participants reported gingival retraction. Zhao et al. noted increased gingival volume or gingival retraction in patients undergoing orthodontic treatment,10 while Verrusio et al. reported increased periodontal parameters following orthodontic treatment, which is likely related to changes in subgingival microbial flora.22 These modifications can subsequently induce inflammation and papillary bleeding.22
Plaque accumulation remains a major secondary effect of fixed orthodontic treatment due to long-term difficulties in maintaining adequate oral hygiene. In the present study, 40.0% of patients with gingival inflammation underwent scaling and/or professional brushing. Previous research emphasized that regular professional hygiene sessions and patient motivation significantly contribute to maintaining periodontal health during orthodontic treatment.23 Fixed orthodontic treatment also influences adult patients’ quality of life. The OHIP-5 assesses key domains of oral health-related quality of life (OHRQoL), including functional limitation, physical pain, psychological discomfort, physical disability, and social disability.24 This instrument has been validated in several countries, including Romania and Poland.25, 26
Incorporating OHIP-5-based questions into our questionnaire allowed us to evaluate these aspects. Most participants (81.2%) stated that they often have difficulties chewing, while 40.6% occasionally experienced reduced taste perception following orthodontic treatment. Pain related to orthodontic treatment was commonly reported (57%), suggesting a potential correlation with the orthodontic apparatus activation sessions.
Patients who responded to our questionnaire indicated that they never (30.9%) or hardly ever (23%) felt insecure about the appearance of their mouth due to the orthodontic apparatus. Furthermore, the orthodontic treatment rarely (32.1%) impeded their ability to perform their usual duties. These results demonstrate that patients are focused on the ultimate outcome of treatment and are highly motivated to achieve it.
Finally, emerging evidence indicates that the COVID-19 pandemic has influenced various aspects of oral health, including implant stability, overdenture performance, oral-facial-digital syndrome (OFD), temporomandibular disc displacement, and gingival crevicular fluid and periodontal ligament.27, 28, 29, 30, 31, 32
Limitations
This study has several limitations. First, the distribution of male and female participants could not be controlled. However, the inclusion of participants of both sexes represents a strength, as it allows the results to be applied to a broader population.
Second, due to restrictions related to the COVID-19 pandemic, the information obtained in the questionnaire could not be correlated with a clinical examination.
Conclusions
Early diagnosis of periodontal conditions during orthodontic treatment is essential for successful therapeutic outcomes. Many adult patients undergoing orthodontic therapy perceive monthly check-ups as sufficient for managing their oral and periodontal needs. However, orthodontists play a central role in educating patients about effective oral hygiene practices, identifying changes of periodontal status, and referring patients for periodontal consultation when needed. The inclusion of periodontal examinations before, during and after orthodontic treatment can lead to the prognosis improvement and reduce the incidence of treatment-related periodontal lesions.
Orthodontic treatment in adults contributes not only to esthetic and functional improvements but also to enhanced psychosocial well-being and overall quality of life.
Ethics approval and consent to participate
Not applicable.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.