












Abstract
Background. Knowledge on the potential applications of artificial intelligence (AI) as a diagnostic instrument in the domain of pediatric dentistry is imperative, as AI may significantly influence present and future dental practice.
Objectives. The present study aimed to evaluate the knowledge, perception and attitude of pediatric dentists and postgraduate students in the pediatric specialty with regard to the employment of AI in pediatric dental practice.
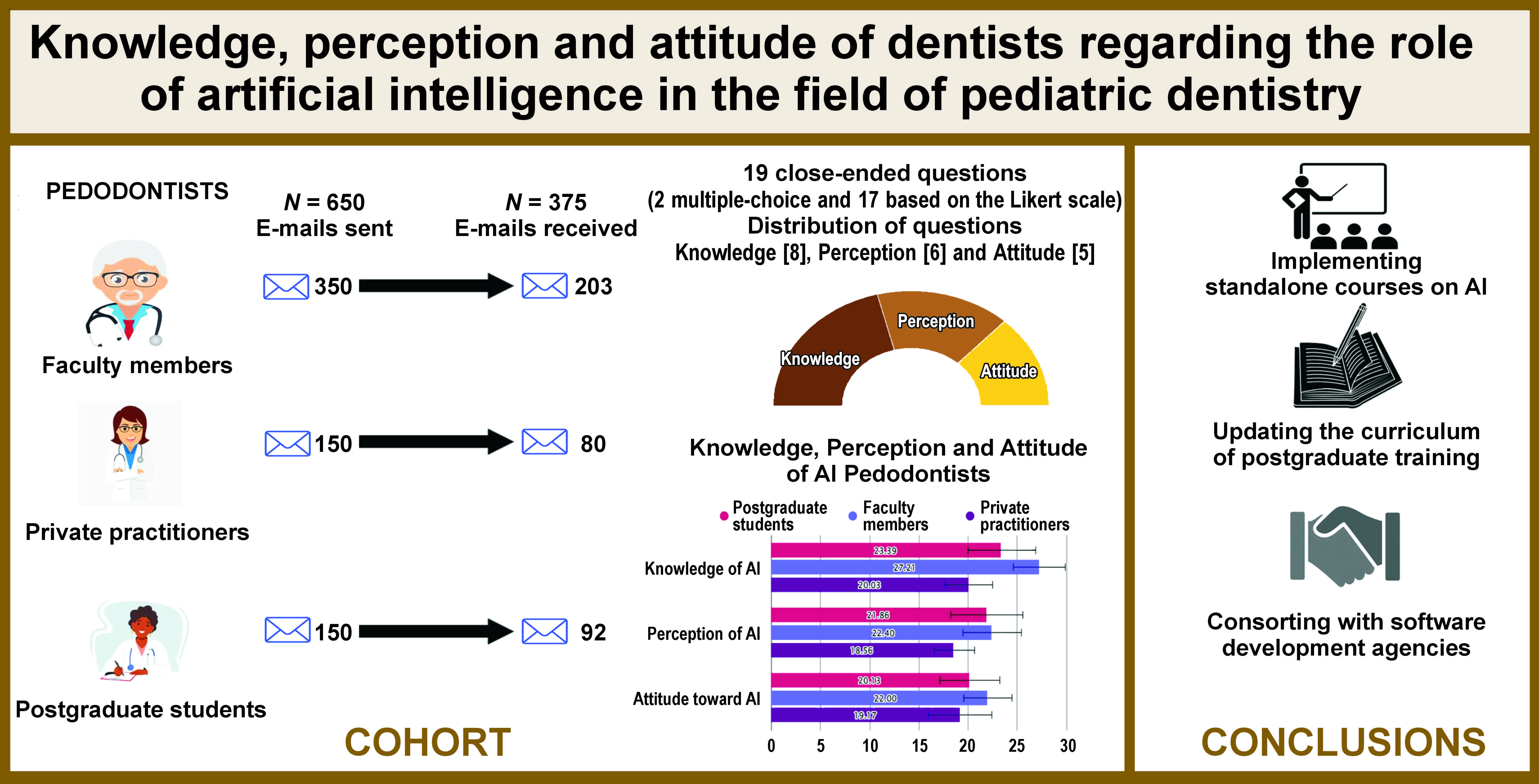
Material and methods. An online questionnaire survey was conducted among 375 participants (92 postgraduates, 203 faculty members and 80 private practitioners), who were provided with 19 close-ended questions through the Google Forms link sent via email. The questions referred to the knowledge, perception and attitude of the participants, with 17 questions answered using a three-point Likert scale and 2 of them being multiple-choice questions. The responses were analyzed using the χ2, Kruskal–Wallis and Mann–Whitney U tests.
Results. A total of 62% of the participants were familiar with the term ‘artificial intelligence’, and the majority confirmed that AI could be used for the identification of plaque (57%) and supernumerary teeth (52%), the detection of early childhood caries (ECC) (68%) and the ectopic eruption of first permanent molars (67%), the assessment of child psychology (82%), and the estimation of chronological age (67%). Most participants felt that AI training should be incorporated into the postgraduate curriculum (82%) and were willing to introduce AI to clinical practice (87%). The barriers related to the use of AI were high costs (83%), the lack of training after graduation (78%), the lack of technical knowledge (77%), the fear of misdiagnosis (73%), and the lack of awareness (71%).
Conclusions. The present study concluded that although most pedodontists and postgraduate students had knowledge on AI, there were many obstacles connected with the use of AI in the field of pediatric dentistry. Therefore, the basic training of AI should be included in the curriculum of postgraduate studies.
Keywords: knowledge, survey, questionnaire, pediatric dentistry, artificial intelligence
Introduction
In 1956, John McCarthy introduced the concept of artificial intelligence (AI).1 This field of study can be defined as the practical application of computer science, which aims to replicate the cognitive abilities of humans. Artificial intelligence is focused on the development of intelligent systems that possess the capacity to think and learn, similar to their human counterparts.1 Artificial intelligence and its subcategories – machine learning (ML) and deep learning (DL) – have been integrated into numerous facets of dentistry, encompassing the field of pediatric dentistry.2
Machine learning, a subset of AI, relies on algorithms to make predictions based on datasets. Its objective is to enable machines to learn from the available data and solve problems without human intervention. In contrast, neural networks consist of algorithms that process signals using artificial neurons. Deep learning, a subset of ML, utilizes a deep neural network with multiple computational layers to analyze the input data. The purpose is to create a neural network that would be able to automatically identify patterns and enhance feature detection. Deep learning is also referred to as a convolutional neural network (CNN). In the field of pediatric dentistry, CNNs are primarily employed to analyze large and intricate images, thereby improving the accuracy and efficiency of diagnostic processes.3
The implementation of AI can potentially eliminate some laborious and time-consuming procedures so far performed by dental professionals. Furthermore, it is plausible to enhance the health of the general population at decreased expenditure, provide customized, preventative and predictive dental treatment, and consolidate the accessibility of healthcare for all. Artificial intelligence possesses the capability to elevate the benchmarks of dental care, refine the precision and efficacy of diagnostic procedures, devise enhanced visual aids for treatment, simulate outcomes, and forecast oral ailments and well-being.2
Artificial intelligence has been commonly employed in the field of pediatric dentistry to provide support for pedodontists in improving the accuracy of their diagnoses. These models prove to be immensely beneficial at both the individual and community levels, as they effectively classify children into various risk groups, at the same time enabling the identification and enumeration of teeth, the identification of supernumerary teeth, the diagnosis of the early ectopic eruption of first permanent molars, and the assessment of age, among other functionalities. Furthermore, they can serve as valuable tools in the planning and evaluation of oral health programs in schools, thereby increasing the awareness of dental well-being among children.2, 4
Despite the numerous advantages of AI, its use in pediatric dentistry remains significantly restricted. This can be ascribed to a multitude of factors, including the limited knowledge and understanding of AI principles among pedodontists, fear and apprehension with regard to using AI software, and the lack of proper knowledge, training and skills for using AI in clinical practice. Moreover, the public is reluctant to place confidence in the outcomes of AI. As a result, various challenges persist, necessitating a proactive approach to finding a resolution.5
Owing to the lack of previous studies, the present study was conducted to assess the knowledge, perception, attitude, and barriers regarding the use of AI in the field of pediatric dentistry among postgraduates, faculty members and private practitioners.
Material and methods
Study design and setting
The present cross-sectional, descriptive, questionnaire-based study was conducted from July to September 2023 at the Department of Pedodontics at Yogita Dental College and Hospital, Khed, India, on postgraduate students, faculty members and private practitioners in the field of pedodontics, who were registered with the Indian Society of Pedodontics and Preventive Dentistry (ISPPD). This survey was approved by the institutional ethics committee (approval No. EC/NEW/INST/2022/2959/Y23/212), and was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Study participants and data collection procedure
A formal letter of request was submitted to the administrative officers of ISPPD, seeking authorization to disclose the list of pedodontists, along with their corresponding email addresses, who have been duly registered as postgraduate students, faculty members and private practitioners in the field of pediatric dentistry. From the list of 2,974 individuals provided by ISPPD, it was observed that there were 680 postgraduate students, 694 private practitioners and 1,600 individuals who were faculty members. This distribution followed an approximate ratio of 1:1:2.3. Consequently, for the purpose of the present study, the participants were selected through the non-probabilistic convenience sampling technique. Specifically, a Google Forms link, accompanied by a set of instructions and consent forms, was randomly dispatched via email to 650 ISPPD members (150 postgraduate students, 150 private practitioners and 350 faculty members). This distribution was carried out in accordance with the initial ratio of 1:1:2.3. The participants were afforded the opportunity to complete the questionnaire on a single occasion, with no time restrictions. Subsequently, after clarifying the objective and ensuring the preservation of confidentiality, and after the participants had provided informed consent and expressed willingness to participate in the survey, their responses were gathered. The survey guaranteed the maintenance of confidentiality, as it did not require the disclosure of personal information regarding the participants’ identities. Additionally, it was explicitly stated in the participant recruitment statement that participation in the survey was completely voluntary. The responses were provided anonymously, without any identifying information. The principal investigator was the sole individual granted access to the data. Duplicated entries were rectified, and only responses that were fully completed were considered. Reminder emails to complete the forms were sent after 1 month.
Pedodontists employed as faculty members and in private practice, along with postgraduate students pursuing their course in the specialty of pedodontics, who agreed to participate in the study, were included. Undergraduates, participants who did not provide consent, as well as those who provided incomplete forms, were excluded from the study.
Sample size estimation
The sample size estimator provided by Calculator.net (https://www.calculator.net/sample-size-calculator.html) was used to establish the appropriate sample size. According to the statistics from ISPPD, the total number of pedodontists in 2023, including postgraduate students, was 2,974. Based on this, statistical power analysis was performed to calculate the sample size. The suggested sample size was 341, with a design effect of 50%, a margin of error of 5% and a confidence level of 95%. Considering a 60% response rate, the estimated sample size was 569. Previous studies yielded a fluctuating rate of response ranging from 50% to 60%.6, 7, 8 Consequently, the current study was undertaken encompassing a sample size of 650 individuals.
Study instrument
The questionnaire was divided into 4 domains. The first one, known as part A, focused on 6 open-ended questions on sociodemographic characteristics; the participants entered their age, gender, designation, workplace, region, and years of experience. Part B consisted of 8 close-ended questions identifying the basic knowledge of the participants on the use of AI in the field of pediatric dentistry (7 questions used a three-point Likert scale (agree, neutral, disagree) and 1 was a multiple-choice question). Part C consisted of 6 questions assessing the participants’ perception with regard to the use of AI (5 questions used a three-point Likert scale and 1 was a multiple-choice question). Part D comprised 5 questions on a Likert scale, regarding the attitude of the participants toward AI.
Pre-testing and content validity of the questionnaire
The questionnaire was created through the collaborative efforts of 5 professionals, including 3 pedodontists, one AI expert and one researcher with a decade of experience, who were not part of the study. Subsequent to the evaluation conducted by these 5 specialists, Aiken’s V statistic was calculated, revealing a value of 0.92, indicating a favorable level of content validity. To assess the dependability of the inquiries, a preliminary examination or pre-testing of the questionnaire was conducted on 35 individuals who were not involved in the study. The reliability of the questionnaire was assessed by employing Cronbach’s alpha; the test yielded a value of 0.87 for knowledge-based questions, and 0.92 for perception- and attitude-based questions. To determine the level of agreement among the questions, the questionnaire was administered to the same cohort after a 2-week interval. Inter-observer agreement was evaluated using the kappa coefficient, which amounted to 0.94.
Scoring criteria
Each question (except for questions 2 and 14) was scored as agree = 5, neutral = 2 or disagree = 0. The maximum score for knowledge was 35 (7 × 5), 25 (5 × 5) for perception and 25 (5 × 5) for attitude. The mean and standard deviation (M ±SD) values were calculated for knowledge, perception and attitude.
Statistical analysis
The collected data was subjected to statistical analysis with the use of the IBM SPSS Statistics for Windows software, v. 22.0 (IBM Corp., Armonk, USA). The normal distribution of the data was confirmed using the Shapiro–Wilk test. The compilation and presentation of sociodemographic variables and the participants’ responses were achieved using frequency distributions. To determine significant differences between the variables, non-parametric tests, including the χ2 test, were employed. The knowledge, perception and attitude scores were calculated and analyzed using the Mann–Whitney U test (for gender) and the Kruskal–Wallis test (for other variables), followed by post-hoc analysis with Dunn’s test. The correlation for ordinal data, such as the knowledge, perception and attitude scores, was calculated with Spearman’s ρ test. The level of significance was set at p ≤ 0.05.
Results
Demographic details of the respondents
The baseline demographic characteristics of the participants are presented in Table 1. A total of 375 participants completed the online survey, with a response rate of 58%. A total of 118 participants represented the age group of 26–30 years, and the smallest number of participants were in the age group of 56–60 years. With regard to gender, 57% of the participants were male, and 43% were female. Of the 375 participants, 54% were faculty members, 25% were postgraduates and 21% were private practitioners. Of the sample, 41% had less than 5 years of experience, and 34% had more than 10 years of experience (Table 1).
Assessing the knowledge of the participants on AI and its applications
A total of 62% of the participants were familiar with the term ‘artificial intelligence’, with a statistically significant difference between the groups (p = 0.001); among them, there were 74% of faculty members, followed by 61% of postgraduates. As many as 44% of private practitioners were unaware of the term ‘AI’. The most common source of AI information was industry news (78%), and the least common professional organizations (45%). Most of the participants agreed that AI could be used for identifying plaque in children, with no significant differences between the participants (p > 0.05), whereas statistically significant differences were observed when the participants were asked about the use of AI for the identification of supernumerary teeth, the detection of early childhood caries (ECC) and the ectopic eruption of first permanent molars, and the assessment of child psychology (p < 0.05). Most faculty members agreed with the use of AI for various purposes in the field of pediatric dentistry. A total of 67% of postgraduates expressed their agreement with the implementation of AI in the identification of supernumerary teeth, while 38% of private practitioners held a different opinion. The majority of faculty members (81%) and private practitioners (56%) were in favor of utilizing AI for the detection of EEC, although 41% of postgraduates disagreed with this notion. Similarly, the majority of faculty members (77%) and postgraduates (71%) accepted the use of AI for the estimation of chronological age in children, whereas 33% of private practitioners expressed their disagreement. With regard to the detection of the ectopic eruption of first permanent molars in early mixed dentition, most faculty members and private practitioners were supportive of employing AI, with only 59% of postgraduates agreeing to the same. Furthermore, the majority of the respondents agreed with the use of AI for assessing child psychology (Table 2).
Assessing the perception of AI by the participants
A total of 81% of the participants wanted to use AI software in the future, and the highest agreement was noticed among the faculty members. Most of the respondents (82%) felt that it should be part of postgraduate training, with a statistically significant difference between the groups (p = 0.026). As many as 85% of the participants, mostly faculty members (88%) and private practitioners (85%), wanted a professional training course on the use of AI (p > 0.05). Also, 87% of the participants agreed that AI could be used in clinical practice, and 85% of the participants would recommend the use of AI to their fellow colleagues, with statistically significant differences noted (p < 0.05), where the highest agreement was noticed among the private practitioners and the lowest among the postgraduates. The barriers related to the use of AI in the field of pediatric dentistry were high costs (83%), the lack of postgraduate training (78%), the lack of technical knowledge (77%), the fear of incorrect diagnosis (73%), and the lack of awareness (71%), as shown in Table 2.
Assessing the attitude of the participants toward AI
Aggregating the attitude scores for the 5 questions could result in biased interpretation. Therefore, each question was individually scrutinized to enhance comprehension. A considerable number of male faculty members and private practitioners aged between 26 and 55 years demonstrated elevated mean scores and exhibited a favorable disposition toward incorporating AI into the field of pediatric dentistry. They firmly believed that AI had immense prospects, with the difference being statistically significant at p < 0.05. In contrast, female postgraduate students and older individuals aged 56–60 years displayed comparatively lower mean scores and held a less optimistic attitude toward the integration of AI. The postgraduates and those with less than 5 years of experience, ranging in age from 46 to 50 years, exhibited low mean scores and expressed uncertainty regarding the superior diagnostic capability of AI as compared to pedodontists. A substantial majority, constituting 66% of the academic faculty, conveyed a belief that AI may generate errors in the treatment protocols. By contrast, 49% of postgraduate students maintained a divergent perspective; the difference was statistically significant (p = 0.001). A considerable proportion of female respondents, postgraduates and older individuals between the age of 56 and 60 years had low scores and held the view that AI is prone to committing diagnostic errors, as well as expressed concern over the unethical utilization of AI by certain institutions (Table 2 and Table 3).
Mean scores for the knowledge, perception and attitude of the participants
There were statistically significant gender differences in the mean knowledge scores of the participants, with males having higher scores (28.12 ±3.78) than females (26.67 ±3.12) (p < 0.05). The faculty members had the greatest mean perception scores (22.40 ±2.98), followed by the postgraduates (21.86 ±3.67) and the private practitioners (18.56 ±2.03). The participants with less than 5 years of experience had better mean knowledge scores (27.39 ±3.12), while the participants with 5–10 years of experience had better mean perception scores (23.40 ±2.32). The lowest mean knowledge (22.03 ±2.34) and perception scores (19.56 ±2.45) were noticed in the participants with more than 10 years of experience. Statistically significant age differences were observed in the participants’ mean knowledge and perception scores (p < 0.05). The participants aged less than 45 years had better scores than the participants aged more than 45 years, as shown in Table 4.
Post-hoc analysis was conducted to perform pairwise comparisons between different age groups. The analysis revealed that there were significant differences in the knowledge scores between age groups 26–30 years and 31–35 years, 36–40 years, 46–50 years, and 56–60 years. Furthermore, significant differences were observed between age groups 41–45 years and 46–50 years as well as 56–60 years. In terms of perception scores, significant differences were found between age groups 31–35 years and 46–50 years, 51–55 years and 56–60 years. Additionally, differences were evident between age groups 36–40 years and 46–50 years, 51–55 years as well as 56–60 years. Lastly, significant differences were noted in the attitude scores between age groups 26–30 years, 31–35 years, 36–40 years, and 41–45 when compared to age group 56–60 years. Pairwise comparisons for designation demonstrated that significant differences were apparent between the postgraduates and the faculty members in relation to the scores for knowledge and attitude. The perception scores of the private practitioners were significantly different from those of the faculty members and postgraduates. Pairwise comparisons in terms of experience indicate the presence of notable disparities among individuals with varying levels of experience. Specifically, when examining the knowledge and perception scores, it was observed that individuals with less than 5 years of experience differed significantly from those with 5–10 years of experience or more than 10 years of experience. Conversely, in relation to the attitude scores, discernible differences were identified between individuals with less than 5 years of experience and those with 5–10 years of experience (Table 5).
Correlation between the knowledge, perception and attitude scores and the demographic variables of the participants
The knowledge, perception and attitude exhibited by the participants showed a negative correlation with the age of the participants, suggesting that older individuals possessed less profound mindset, knowledge and interpretation pertaining to the utilization of AI in the realm of pediatric dentistry as compared to younger individuals. However, there was a weak correlation between age and attitude, which suggests that there might be a tendency for attitude to decrease with an increasing age, but this relationship is not strong enough to be considered significant. There was a positive correlation between knowledge and attitude, and between knowledge and perception. These findings indicate that as pedodontists’ comprehension of AI increased, their mindset and interpretation also improved. This is evident from the data presented in Table 6.
Discussion
Artificial intelligence has a vast array of medical applications and has recently experienced a surge of popularity, necessitating the meticulous exploration of its potential implementation in the field of dentistry. However, a considerable number of scientists and medical professionals are not familiar with AI and its potential impact on both their personal and professional lives. To the best of our knowledge, this survey stands out among the existing research because of its distinctive focus on the application of AI in the field of pediatric dentistry.
The results of the present study indicated that 62% of the participants, mostly faculty members, were aware of the existence of AI. Our findings are similar to those of previous studies.6, 7, 8 The reason behind this phenomenon may lie in the fact that AI encompasses a wide range of emerging technologies that have a lasting impact on everyday life. Artificial intelligence enables the analysis of large sets of data, thus providing accurate and dependable information, and ultimately enhancing the process of making informed decisions.9 The main sources of knowledge on AI were industry news, conferences and online data from both social media and academics. This is in contrast with the findings of a previous study, in which social media were the main source, and not academics.10
Regarding the field of pediatric dentistry, AI can be used to identify plaque in children. An AI model demonstrated satisfactory clinical efficacy in the identification of dental plaque on primary teeth in comparison with an experienced pediatric dentist.11 The utilization of an AI model can potentially offer support to parents in their everyday existence, as it can significantly diminish the challenges associated with identifying dental plaque on their offspring’s teeth, thereby aiding in the prevention of dental caries.4 In our study, 52% of the participants felt that AI could also be used for the identification of supernumerary teeth. The CNN-based deep learning represents a highly promising strategy for identifying supernumerary teeth in the initial stage of mixed dentition.12
As many as 68% of the participants felt that AI could detect ECC, as reported in previous studies as well.13, 14 Parents can utilize their customary smartphones to capture the images of their offspring’s dentition, which can then be analyzed with the aid of AICaries. This enables parents to proactively pursue the treatment of their children during the initial and remediable phases of ECC. The incorporation of AI has the potential to enhance the diagnostic acumen of dentists, primarily by augmenting their ability to detect enamel lesions with greater sensitivity.14 In the present study, 67% of the participants agreed that AI could be used for the estimation of chronological age in children. AI-supported standards can offer considerably more precise forecasts of chronological age, with mean errors of less than 0.05 years. Conversely, conventional approaches have yielded inflated outcomes for both genders.15
Moreover, 67% of the participants agreed that AI could effectively detect the ectopic eruption of first permanent molars, which was also observed in previous studies,4, 16 and 82% of the participants agreed upon the use of AI in assessing child psychology. There are numerous mechanisms by which AI can assist parents, ranging from the provision of tailored guidance that aligns with the requirements of each family to prompt intervention upon the detection of the preliminary indications of developmental challenges or parental strain.17
Most of the participants wanted to use AI software in the future and to attend professional courses to learn about the use of AI in pediatric dentistry. They felt a strong need to include AI training during their postgraduation years and would recommend their colleagues to use AI in their practice. This is in accordance with previous studies.10, 18 These results show the interest of pedodontists in learning new technologies, such as AI, and their willingness to incorporate it into clinical practice. When asked about the barriers related to the use of AI in the field of pediatric dentistry, the majority enumerated the high costs of AI software, the lack of proper training and technical knowledge, the fear of misdiagnosis, and the lack of awareness, as stated in previous studies as well.5, 10 While 82% of the participants felt that AI had a promising future in the field of pediatric dentistry, 55% felt that AI could make errors in diagnosis and treatment planning. Some of them also felt that AI was used unethically by some organizations. Mistakes in the procedure or protocol within the realm of healthcare can potentially yield dire ramifications for the individual undergoing treatment, consequently serving as the unfortunate recipient of said errors. Currently, the absence of clearly established regulations hinders the resolution of legal and ethical dilemmas that could emerge because of the integration of AI within healthcare environments. There is an undeniable requirement for the disclosure of algorithms, safeguarding data privacy and the protection of all parties who benefit from these systems while also ensuring the security of the vulnerabilities linked to cybersecurity.19
The present study revealed no significant difference in the attitude scores between individuals with less than 5 years of experience and those with more than 10 years of experience, which suggests that the level of professional experience may not be a strong predictor of attitude toward AI. This might be due to fact that professionals with different levels of experience may possess a relatively homogeneous knowledge base when it comes to AI in pediatric dentistry. If decision-making processes within the field involve input from professionals of varying experience levels, it could contribute to a consensus in attitude toward AI. However, a better understanding of the specific reasons behind the lack of difference in the attitude scores would likely involve a more in-depth examination, including surveys, interviews or focus group discussions with professionals from both experience groups. Although AI has shown promising results in specific diagnostic tasks within dentistry, it is not a substitute for skilled pedodontists’ comprehensive care, judgment and experience. The treatment protocols in medicine and dentistry can be highly complex and involve multiple factors, such as patient history, comorbidities and individual responses to treatment. Artificial intelligence systems may not yet be sufficiently sophisticated to fully understand and integrate all these variables as effectively as human practitioners.
Our study also revealed that females demonstrated less knowledge about AI than males. However, they were eager to learn about AI. The faculty members and postgraduates had better knowledge and perception scores than private practitioners. Better scores, particularly the knowledge and perception scores, were reported for individuals aged 26–30 years and with less than 5 years of experience, which represents a younger population, mainly postgraduates, as compared to an older age group of 56–60 years and with more than 5 years of experience. This phenomenon could potentially be attributed to a rise in consciousness, availability and enthusiasm among the younger generation to acquire knowledge about the emerging technologies, such as AI, whereas the older generations are more afraid of using AI for diagnosis, as they feel that a machine cannot replace or work better than an experienced pedodontist; most contemporary AI applications offer limited information, which falls short of fully explaining the intricate decision-making process in clinical care.20 Younger individuals, particularly those from generations that have been immersed in technology, are prone to possess a greater level of knowledge and ease with regard to AI concepts. They might have obtained more up-to-date education or training, and may have been exposed to the most recent advancements in AI and its potential applications in pediatric dentistry. Generational perspectives toward technology, innovation and change may influence the way individuals perceive the integration of AI in the field of pediatric dentistry. Differences in the sources of information and exposure to AI-related content through media and educational platforms can also contribute to variations in the knowledge and perception scores across different age groups. Despite this, older individuals demonstrate a strong interest in acquiring knowledge about AI and express a desire to integrate it into clinical practice.
Limitations
As we explored the limitations of the study, it is important to acknowledge the presence of an age bias, as the concepts employed in the survey might be unfamiliar to older individuals. Consequently, this selection bias resulted in a greater representation of younger age groups within the sample. Considering the ease of distributing and accessing the survey via the Google Forms link, coupled with the subject matter’s appeal to a younger population, these circumstances may have contributed to the overrepresentation of young individuals within the study sample. The questionnaire was formulated in English, which is the dominant language in the area under investigation. This might have hindered the involvement of individuals who did not possess proficiency in English. The use of the Likert scale in close-ended questions may have hindered the generation of suggestions or concepts for inquiries that require a multitude of perspectives, thereby leading to misinterpretation. The novel scoring system used in the study needs to be tested in a diverse population for generalizability, external validation and reliability assessment.
Recommendations
According to the findings of the current survey, most pedodontists generally exhibit a predominantly positive attitude toward AI technology. A significant proportion of them expressed their willingness to incorporate AI into their professional practice, with numerous individuals indicating their readiness to acquire new technological skills and embrace novel advancements. Nevertheless, the findings also revealed that these professionals harbor concerns regarding the financial and time investments required for the implementation of AI in their practice, as well as the lack of awareness and technical expertise. To address these concerns effectively, it is recommended that AI be seamlessly integrated into academic curricula for undergraduate and postgraduate students. This integration will cater to the specific needs of pedodontists across disciplines. Furthermore, targeted efforts should be made to increase the comfort level of pedodontists in the age range of 45–64 years. To achieve this, it is important to provide training programs, workshops and other resources that are specifically designed to assist users in feeling more comfortable and confident when utilizing AI tools.
Conclusions
The majority of participants exhibited knowledge regarding the advantages of employing AI in the field of pediatric dentistry and expressed confidence in its potential as an advantageous tool. The investigation revealed that the presence of enhanced technical facilities within clinics and the provision of education to professionals at both undergraduate and postgraduate levels could potentially overcome obstacles in utilizing AI within the domain of pediatric dentistry.
Ethics approval and consent to participate
The study was approved by the institutional ethics committee at Yogita Dental College and Hospital, Khed, India (approval No. EC/NEW/INST/2022/2959/Y23/212). All participants provided written informed consent.
Data availability
The datasets supporting the findings of the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.