












Abstract
Background. Root resorption (RR) is usually a consequence of dental trauma, pulpal infection, primary occlusal pressure, or orthodontic tooth movement, leading to the loss of anatomical root formation. As a result of apical RR, the apical constriction is destroyed, and the determination of the working length (WL) may become difficult.
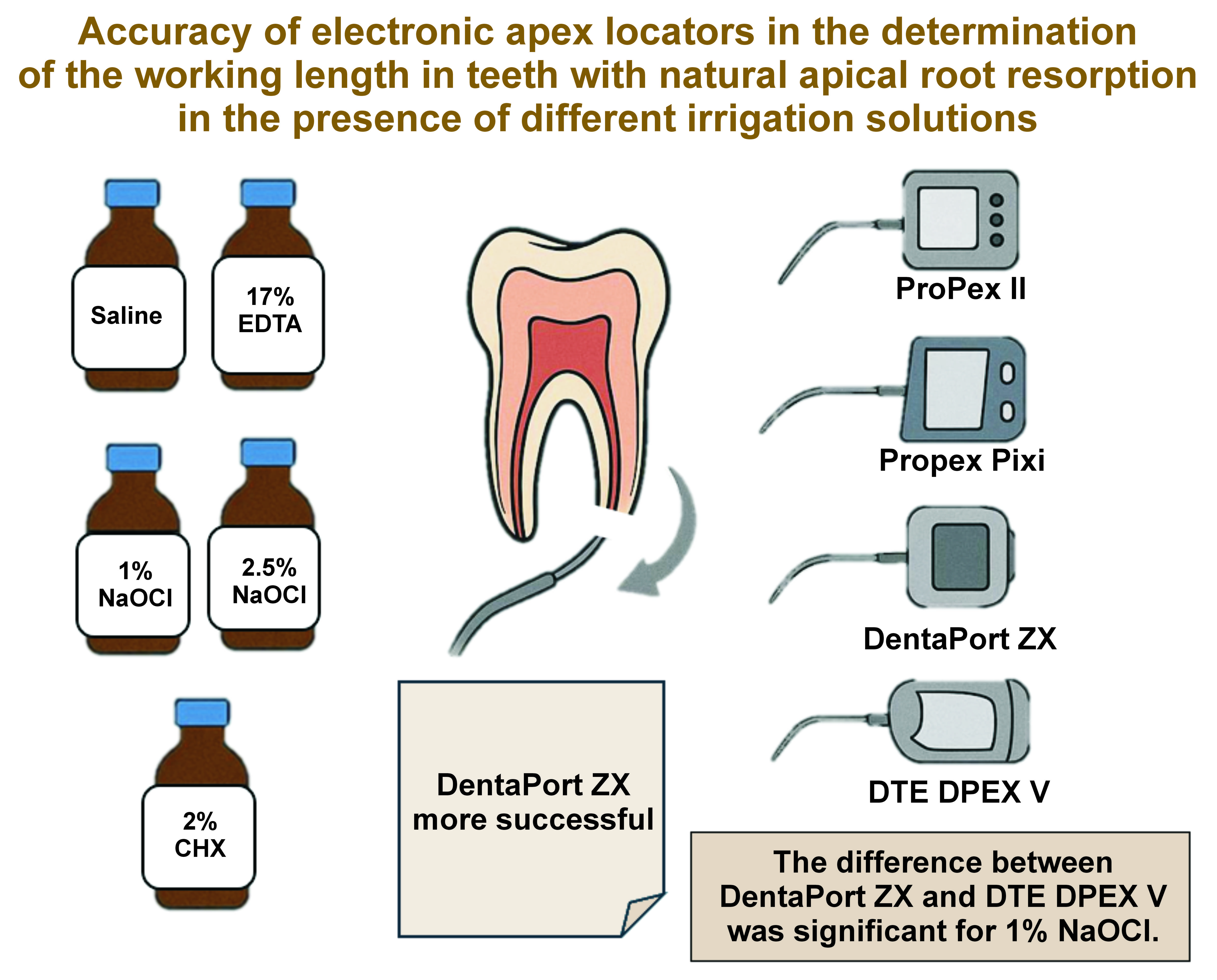
Objectives. The purpose of the present study was to evaluate the accuracy of 4 different electronic apex locators (EALs) – ProPex® II, Propex Pixi®, DentaPort ZX, and DTE DPEX V – in the determination of WL in teeth with natural apical RR in the presence of different irrigation solutions (ISs).
Material and methods. A total of 36 teeth with natural apical RR were included in the study. The actual length (AL) was determined under a stereomicroscope at ×15 magnification. Afterward, the electronic length (EL) was established by using 4 different EALs in the presence of different ISs. The ISs used in the measurements were freshly prepared, and 6 groups were organized based on the solution used. The control group was marked as group 1. For groups 2–6, 1% sodium hypochlorite (NaOCl), 2.5% NaOCl, saline, 2% chlorhexidine (CHX), and 17% ethylenediaminetetraacetic acid (EDTA) were used, respectively. After each measurement, the roots were washed with 5 mL of distilled water and dried with paper points before the same teeth were used in the subsequent group. The absolute length was subtracted from EL for each tooth to calculate the difference. The data was analyzed statistically.
Results. For each device, there were no significant differences in the success rates between the ISs used. In group 1, there were no significant differences among the 4 EALs. In group 2, DentaPort ZX was significantly more successful than DTE DPEX V (p = 0.037). There were no significant differences among EALs in groups 3–6.
Conclusions. The difference between DentaPort ZX and DTE DPEX V was statistically significant in group 2 (1% NaOCl).
Keywords: electronic apex locators, irrigation solution, natural root resorption
Introduction
Root resorption (RR) is a pathological process that concludes with the destruction of dental hard tissues, such as cement and dentin. In primary teeth, RR is usually physiological, but in permanent teeth, it can be pathological – it may occur at the inner surface of the root canal space (internal RR), the outer surface of the root (external RR), or both sides of the root together.1
External RR is often a consequence of severe dental trauma, pulpal infection, primary occlusal pressure, or orthodontic tooth movement leading to the loss of anatomical root formation. External RR is usually diagnosed through clinical and radiographical examinations, without any clinical symptoms.2, 3 Although external RR is common, there is no generally accepted treatment protocol. The treatment process varies according to the patient’s symptoms. Root canal treatment (RCT) is accepted in symptomatic patients, while follow-up is sufficient in asymptomatic patients.
Working length (WL) determination is of utmost importance in RCT. The working length is expressed as either 0.5–2.0 mm short of the radiographic apex or the extension of the apical constriction.4 An adequate WL ensures the disinfection of the whole root canal and prevents damage to the periapical tissues.5 The measurement of WL can be acquired in various ways, e.g., by using an electronic apex locator (EAL).6 Among the common methods of WL determination is the radiographic method. However, it has several disadvantages, such as distortion and the superposition of anatomical structures.7
The determination of WL with EALs is a well-known technique employed in permanent teeth. The accuracy of EALs is affected by various factors. The most important ones are the moisture content in root canals, irrigation solutions (ISs) and the diameter of the apical foramen.8 Irrigation solutions are used to clean and disinfect the canal and are vital in RCT. To clean the root canal of a tooth, many materials have been used, the most common being sodium hypochlorite (NaOCl), chlorhexidine (CHX) and ethylenediaminetetraacetic acid (EDTA).9 In addition, a recent study showed that most of dental professionals preferred the use of the full-strength NaOCI concentration as the main IS.10 However, the presence of ISs in the root canal space may impact the performance of EALs.7, 8, 9, 11
Although there are studies in the literature showing the accuracy of EALs in the determination of WL in primary teeth with apical RR and permanent teeth with artificial RR,12, 13 no study has investigated the accuracy of EALs in the determination of WL in permanent teeth with natural RR.
The present study evaluated the effects of different ISs on the accuracy of 4 different EALs in the determination of WL in extracted teeth with natural apical RR. The null hypothesis was that there would be no differences with regard to different ISs between EAL measurements during RR.
Material and methods
The Clinical Research Ethics Committee of Akdeniz University, Antalya, Turkey, reviewed and approved the study design (No. of approval: KAEK-476).
The G*Power program, v. 3.1.9.7 (https://www.psychologie.hhu.de/arbeitsgruppen/allgemeine-psychologie-und-arbeitspsychologie/gpower) was used to determine the sample size. The total sample size was calculated as 36 for each EAL, with an alpha value of 0.05, power of 80% and an effect size of 0.6.
The inclusion criteria were as follows: permanent single- or multi-rooted teeth with external RR in the apical third of the root; the single-rooted teeth extracted due to periodontal or orthodontic reasons; the multi-rooted teeth extracted, as they could not be restored. After the inspection of the teeth under a stereomicroscope (Stemi; Carl Zeiss, Jena, Germany), teeth after RCT, or with cracks and fracture lines were excluded from the study. Five teeth were excluded because of the fractured roots. The remnants of hard and soft tissues on the teeth were removed with the help of a scaler. To prevent the teeth from drying, they were stored in saline solution during the study period.
Determination of the actual length
The incisal edges or cusps of the included teeth were flattened to create a stable and reliable coronal reference point after the endodontic access cavities were prepared in all teeth. Using a stereomicroscope at ×15 magnification, a #20 K-type file was advanced until it could be seen apically, at the start of the resorption area. The first time the file was noticed, a rubber stopper was attached to the incisal edge of the tooth, and then the length between the tip of the file and the rubber stopper was measured with an endometer and recorded as the actual length (AL). This procedure was repeated 3 times for each tooth to prevent operator failures.
Determination of the electronic length
Four different EALs were used: ProPex® II (Dentsply Maillefer, Ballaigues, Switzerland); Propex Pixi® (Dentsply Maillefer); DentaPort ZX (J. Morita Tokyo, Saitama, Japan); and DTE DPEX V (Guilin Woodpecker Medical Instruments, Guilin, China).
Alginate was prepared according to the manufacturer’s instructions. The lip clip of the each EAL was placed in the alginate and the teeth were embedded in the alginate impression model at the cementoenamel junction (CEJ). The ISs were freshly prepared, and 6 groups were organized based on the solution used:
– group 1 (control, no solution): After the root canals were dried with paper points, EL was determined by using the 4 different EALs. A #20 K-file was proceeded throughout the canal until the signals ‘Apex’ for ProPex II, ‘0.0’ for Propex Pixi, ‘0.0’ for DentaPort ZX, and ‘0.0’ for DTE DPEX V occurred on the EALs to confine the apical resorption area. The rubber stopper was attached when the signals were persistently perceived on the screen of the device for 5 s, and then the length between the tip of the file and the rubber stopper was measured with an endometer and recorded as the electronic length (EL). This procedure was repeated 3 times for each tooth;
– group 2 (1% NaOCl): For each tooth, 5 mL of freshly prepared 1% NaOCl was used as IS. The EL values were determined using the same electronic measurement method as in group 1;
– group 3 (2.5% NaOCl): For each tooth, 5 mL of freshly prepared 2.5% NaOCl was used as IS. The EL values were determined using the same electronic measurement method as in group 1;
– group 4 (saline): Saline in the amount of 5 mL was used as IS. The EL values were determined using the same electronic measurement method as in group 1;
– group 5 (2% CHX): For each tooth, 5 mL of freshly prepared 2% CHX was used as IS. The EL values were determined using the same electronic measurement method as in group 1; and
– group 6 (17% EDTA): For each tooth, 5 mL of freshly prepared 17% EDTA was used as IS. The EL values were determined using the same electronic measurement method as in group 1.
The same teeth were used in all groups. After using each IS, the root canals were irrigated with 5 mL of distilled water to prevent the interaction of fluids and dried with a paper point before using the next IS. The procedures were performed on separate days for each group. For all 6 groups, the procedures were performed by a single operator.
Statistical analysis
The deviation of WL was calculated by subtracting AL from EL for each tooth (EL − AL). The difference was negative (−) when the electronic measurement was shorter than AL and positive (+) when the electronic measurement was longer than AL, whilst (0) indicated coinciding measurements. Statistical analysis was conducted to evaluate the deviation between the recorded AL values and the EL values, how much the obtained WLs deviated from the resorption area (*0 points), and whether this deviation was significant. The accuracy of WL determination methods was assessed with a tolerance of ±1 mm. The possible differences between the acceptable measurements obtained by means of EALs were analyzed with the χ2 test. To control for type I errors, Bonferroni’s correction was used in pairwise comparisons, using standard statistical software – IBM SPSS Statistics for Windows, v. 25.0 (IBM Corp., Armonk, USA). The significance level was set at 5% for all tests.
Results
In this study, 36 teeth with natural RR were evaluated. The accuracy of 4 EALs depending on the IS used within the tolerance range of ±1 mm is shown in detail in Table 1. In group 1, there were no significant differences among the 4 EALs and the most successful results were obtained by Propex II. In group 2, DentaPort ZX was significantly more successful than DTE DPEX V (p = 0.037). There were no significant differences among EALs in groups 3–6. The success rates for each EAL in the study groups are shown in Table 2. Additionally, there were no significant differences in the success rates among the ISs for each device (Table 3).
Discussion
The determination of WL is an important step in RCT. An accurate WL measurement enables the adequate and complete instrumentation and filling of root canals. Although radiographic images are used for assessing WL in RCT, EALs are considered effective tools for determining the WL of the root canal.14 There are various in vitro and in vivo studies in the literature that show the efficacy and accuracy of EALs in primary and permanent teeth.15, 16, 17
In this study, alginate was used to create an environment to simulate the clinical conditions during the EAL measurements. Although, in some studies, various materials such as gelatin, agar, floral sponge, and saline have been used,18, 19 the performance of alginate has been found to be superior in mimicking the tooth and surrounding tissues due to its colloidal consistency. In addition, the good electroconductive properties, low cost, availability, and easy preparation of alginate made it the preferred medium in this in vitro study.
Studies examining the accuracy of EALs provided different clinically acceptable margins of error in locating the apical foramen.20, 21, 22 Goldberg et al. investigated the accuracy of Root ZX in teeth with simulated resorption, adopting a tolerance range of ±0.5 mm, ±1 mm and ±1.5 mm, and the success rates of Root ZX were 62.7%, 94.0% and 100.0%, respectively.21 Thus far, a tolerance range of ±0.5 mm has been accepted in some studies.6, 22 However, a tolerance range of ±1.0 mm has been found clinically more appropriate due to the wide anatomical variation in the apical region.20 As a result of apical RR, apical constriction disappears, and thus, the determination of WL becomes difficult in teeth with apical RR. In the present study, the tolerance range was determined as ±1.0 mm.
Many studies in the literature have shown the accuracy of EALs in determining WL.23, 24, 25 Somma et al. used 3 EALs (DentaPort ZX, Raypex 5 and ProPex II) to evaluate their accuracy in vivo.23 Although the best results were acquired with DentaPort ZX, there was no significant difference among the devices.23 Oliveira et al. assessed Root ZX II, Raypex 6, Apex ID, ProPex II, and Propex Pixi in their study, and found no differences between the devices, as well.24 These results are consistent with our study. In our study, a significant difference was found only in group 2 (1% NaOCl), and the most accurate measurements were obtained with DentaPort ZX in this group. Furthermore, the success rate of DentaPort ZX was higher in comparison with all other devices. Since there were statistically significant differences between EAL measurements with regard to different ISs, the null hypothesis was rejected.
There is no consensus on the accuracy of EAL measurements regarding the apical foramen diameter and the file size. Shacham et al. indicated that more accurate results could be obtained with EAL when the difference between the size of the file used for measurement and the apical foramen diameter of the canal was reduced.6 Also, it was reported that an apical foramen diameter greater than 0.6 mm led to erroneous EAL results.6 In addition, Kolanu et al. indicated that the accuracy of Propex Pixi decreased with an increased apical foramen diameter.26 Akisue et al. also showed in their study that a larger apical foramen diameter caused a lower accuracy of EAL.25 To obtain more accurate results, they recommended the use of a file suitable for the diameter of the apical foramen.25 In this study, to attain more accurate results, electronic measurements were made using a #20 K-type file, since the apical foramen was enlarged due to RR.
The chemomechanical preparation of root canals is an important step in RCT. Removing the infected pulp, bacteria and microbial products from the canals cannot be achieved by preparation with endodontic instruments only. Thus, ISs play a vital role in the complete disinfection of the root canal space. In clinical practice, the most often used IS is NaOCl at different concentrations, such as 1%, 2.5% or 5%. In routine RCT, CHX at a concentration of 2% and EDTA at a concentration of 17% are the other commonly used ISs.27 In this study, 1% NaOCl, 2.5% NaOCl, 0.9% saline, 2% CHX, and 17% EDTA were used as ISs during EAL measurements, as these ISs are used more frequently in daily clinical practice.
Prasad et al. investigated the accuracy of electronic measurements made with EALs (Root ZX and iRoot) in the presence of saline, NaOCl, CHX, and EDTA.28 They showed that the presence of ISs in the root canal marginally affected the accuracy of the EALs, with the difference being non-significant.28
Baruah et al. used 0.1% octenidine dihydrochloride (OCT), 2% CHX, and heated and unheated 5% NaOCl as ISs in a study that compared Root ZX Mini and ProPex II.29 It was revealed that the presence of ISs in the canal increased the reliability of EALs. Root ZX Mini was more consistent than ProPex II in the presence of various ISs. Nonetheless, no significant difference was found between the EALs.29 In the present study, the success rate of DentaPort ZX was higher than Propex II in the presence of all irrigants, as well.
Since RR develops physiologically in primary teeth, it is very difficult to determine WL accurately when performing RCT in primary teeth. In order to prevent damage to permanent teeth, the WL of primary teeth should be carefully determined. An in vitro study by Tosun et al. investigated the accuracy of EALs with a tolerance range of ±1 mm in primary teeth with and without apical RR, and indicated that the presence of apical RR affected the performance of EALs.17 Goldberg et al. evaluated the accuracy of Root ZX in permanent single-rooted teeth with simulated apical RR; the roots of the teeth were irrigated with normal saline solution.21 The researchers reported that the accuracy of Root ZX was 94.0% within 1 mm of the direct visual measurement.21 To make a consistent comparison with previous studies, the tolerance range was set as ±1 mm in the present study, as well.
Limitations
This in vitro study has various limitations, such as the absence of oral fluids and tissues. Also, as it is difficult to find teeth with natural RR, and single- or multi-rooted teeth were not differentiated in this study. Thus, the results of this study should be verified by clinical studies.
Conclusions
DentaPort ZX was more successful than DTE DPEX V in group 2 (1% NaOCl). In addition, none of the ISs affected the performance of EALs.
Ethics approval and consent to participate
The Clinical Research Ethics Committee of Akdeniz University, Antalya, Turkey, reviewed and approved the study design (No. of approval: KAEK-476).
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.