Abstract
Background. Intracapsular injections are a recognized therapeutic method for temporomandibular joint (TMJ) pain and limited mandibular mobility. Among many injectables, injectable platelet-rich fibrin (I-PRF) is noteworthy for its safety, promising clinical results and potential regenerative effects. The minimal invasiveness of a single injection makes it attractive as compared to arthrocentesis or a series of administrations.
Objectives. This single-arm, open-label clinical trial aimed to verify the research hypothesis that a single administration of I-PRF into TMJ relieves articular pain.
Material and methods. The study sample included adults with a history of TMJ articular pain treatment. A single injection of I-PRF into the affected TMJ was performed. Each patient assessed (1) articular pain within the last 7 days, (2) the articular pain provoked by a physical examination, (3) muscular pain, (4) headache, and (5) neck pain before and 14 days after the intervention. The investigator measured (6) pain-free and (7) maximal voluntary mandibular abduction.
Results. The study sample included 33 patients and 44 TMJs. No adverse events were observed at the recipient sites (TMJs). The treatment reduced the spontaneous articular pain by 0.5 ±1.5 and the provoked articular pain by 1.2 ±1.9 visual analog scale (VAS) points, with the differences being statistically significant (p < 0.05). Improvement was observed in 39–48% of Wilkes II–V patients, and 5–14% experienced deterioration up to 2 VAS points. Mandibular mobility decreased by an average of 1–2 mm, and no statistically significant effect on muscle pain, headache or neck pain was recorded.
Conclusions. A single intra-articular injection of I-PRF into TMJ brings statistically significant articular pain relief, regardless of the assessment method. In non-respondents, subsequent administrations may be considered.
Keywords: temporomandibular joint, temporomandibular disorders, intra-articular injections, injectable platelet-rich fibrin, I-PRF
Introduction
Temporomandibular joint (TMJ) pain is an interdisciplinary problem affecting 14.6–21.1% of the Polish population.1, 2, 3 A single TMJ is divided by an articular disc and the articular surfaces are covered with cartilage, constantly absorbing friction and loads. The overload and microtrauma of the joint surfaces induce inflammation. The secretion of pro-inflammatory cytokines into the joint cavities deteriorates the composition of the synovial fluid, further intensifying the inflammation and, consequently, causing damage to the articular cartilage cells, leading to the degradation of the joint surfaces, which is related to age and gender.4, 5 Degeneration can lead to the pain, stiffness and limited mobility of the joints.6
The treatment of TMJ pain should be preceded by meticulous and properly directed diagnostics, with regard to the presence of etiological factors, which include those of a psychological nature, systemic diseases and local problems, such as injuries or their consequences.7, 8, 9, 10, 11, 12 While the priority is to exclude the etiological factors of TMJ pain, symptomatic treatment is used in cases of diagnostic difficulties, contraindications to causal treatment and advanced degeneration. Among the surgical methods, the least invasive is intra-articular injections, which, according to the current state of knowledge, are expected not only to relieve pain, but also stimulate the regeneration of the articular surfaces.13, 14
Injectable platelet-rich fibrin (I-PRF) is an autologous blood product containing platelets, growth factors and leukocytes.15 So far, it has been successfully used in treating wounds, especially intraoral ones, and in regenerative medicine.15, 16 The intra-articular administration of I-PRF has been shown to stimulate the regeneration of the cartilage cells and stop the degradation of the joint surfaces.17, 18 It is worth noting, however, that the intra-articular injection of I-PRF is a relatively new technique, and its exact effect on the articular cartilage is still being studied.14
The demonstrated long-term effect of I-PRF on the cartilage tissue justifies administering this self-derived preparation into the cavities of TMJs.14, 19 Intra-articular intervention is reserved primarily for severe TMJ pain, not responding to less invasive treatment. Immediate pain relief from hyaluronic acid or platelet-rich plasma (PRP) administered in one session using a single injection has been confirmed.20, 21 The effectiveness of I-PRF in the ad hoc articular pain relief is also presumed, but this needs to be proven.
This study aimed to verify the research hypothesis that a single administration of I-PRF into the TMJ cavity has an analgesic effect.
Material and methods
The study was designed as a single-arm, open-label clinical trial. It was conducted following the Declaration of Helsinki, and the protocol was approved by the Ethics Committee at the Świętokrzyska Chamber of Physicians, Kielce, Poland (1/2022-VIII). Informed consent to treatment and to participate in the study was obtained from each patient before enrollment in the study. The study protocol was registered in the ClinicalTrials.gov database: NCT05883982. This report was prepared under the CONSORT guidelines.22
The patients were recruited from among those diagnosed with TMJ pain and referred for intra-articular I-PRF injections by orthodontists and prosthodontists. A maxillofacial surgeon (M.S.) confirmed articular pain attributed to the presence of arthritis, disc displacement or degenerative joint disease under the International Classification of Orofacial Pain (ICOP) 2020 protocol (diagnoses 3.2.1 to 3.2.3).23 The detailed inclusion and exclusion criteria are presented in Table 1. Due to the pilot nature of the study, the patients interrupted their current treatment for only 2 weeks. The study was conducted solely at the Maxillofacial Surgery Clinic, NZOZ (non-public health service institution) Ars Medica in Kielce, Poland.
Venous blood was collected into a vacuum tube. Then, I-PRF was acquired according to the protocol for the iFuge D06 centrifuge (Neuation Technologies, Kalol, India): 630 rpm, 3 min. After skin disinfection, approx. 0.4 mL of I-PRF was administered to the upper TMJ compartment, each time by the same operator (M.S.). The TMJ area was not priorly injected with a local anesthetic.
The patients subjectively rated the greatest pain intensity over the last 7 days on an 11-point (0–10) visual analog scale (VAS). The exception was the assessment of the pain provoked by a physical examination, which concerned the severity of pain immediately after the examination. Each type of pain was defined for a specific side of the body, and therefore assigned to a specific TMJ. The range of mandibular abduction was examined between the points of incision superius and incision inferius or their equivalents in prosthetic restorations.
Changes in the spontaneous and provoked TMJ pain were the primary outcomes of this study, and the rest were secondary outcomes. The initial assessment of symptom severity as well as the intervention were carried out at the first and sole examination at the second medical appointment.
The size of the sample resulted from the recruitment time. Sample power calculations were performed based on reference results of Albilia et al. (33/48 respondent TMJs).19
The values of the following variables were collected: muscle, head and neck pain; spontaneous and provoked TMJ pain; and painless and maximal volunteer mandibular abduction. The following were calculated: extremes; decreased, non-changed and increased cases; extreme, median (Me) and mean (M) differences. The subgroups were created depending on the treatment response and the Wilkes stage.
The following software was used: Sample Size Calculator (https://clincalc.com/stats/samplesize.aspx; ClinCalc, Chicago, USA); MedCalc (MedCalc Software, Ostend, Belgium); Microsoft Office (Microsoft Corporation, Redmond, USA); Google Workspace (Google, Mountain View, USA); and LibreOffice (The Document Foundation, Berlin, Germany).
Results
Recruitment lasted from January 1 to June 30, 2023. The intervention and follow-up dates varied among the patients, but each patient was included in the study for 14 days. Of the 34 patients admitted during the recruitment period, one was rejected after completing the 1st questionnaire and after the 1st physical examination. In the discussed case, habitual dislocation of the mandible was diagnosed.
Ultimately, the study group consisted of 33 patients and 44 TMJs. The study group included 25 women and 8 men, all Polish. Particular diagnoses in the Wilkes scale concerned the following numbers of joints: Wilkes II – 29 joints; Wilkes III – 4 joints; Wilkes IV – 9 joints; and Wilkes V – 2 joints. The following comorbidities were diagnosed: general osteoarthritis – 6 patients; and ankylosing spondylitis – 1 patient. The entire sample was included in the analyses. The sample power was 80%.
Two weeks after the administration of I-PRF, the spontaneous pain decreased in 17 (38.6%) TMJs, no change was observed in 21 (47.7%) TMJs, and the pain worsened in 6 (13.6%) TMJs. The average change in pain intensity expressed on an 11-point VAS was −0.45 ±1.47. The decrease in the intensity of subjective pain reported by the patients was statistically significant (p < 0.05) (Figure 1).
In the group of 27 non-respondent TMJs, there was no change in the intensity of the spontaneous joint pain or an increase to a maximum of 2 VAS points (4 joints in 4 different patients). The average change in the non-respondent TMJs was 0.37 ±0.74 VAS points (Me = 0).
In the 17 respondent TMJs, the maximum improvement was −6 VAS points in 1 joint in a patient treated bilaterally. Contralaterally, an improvement of −4 VAS points was observed in the same patient. The average improvement among the respondent TMJs was −1.76 ±1.39 points on the VAS scale (Me = −1).
In the subgroup of 29 Wilkes II TMJs, the change in spontaneous pain intensity was from −6 to 2 VAS points. Improvement occurred in 11 TMJs, no changes were observed in 12 TMJs, and deterioration occurred in 6 TMJs. The average change in pain intensity was −0.34 ±1.67 VAS points (Me = 0) and was not statistically significant (p = 0.280).
In the subgroup of 15 Wilkes III–V TMJs, the change in spontaneous pain intensity ranged from −3 to 0 VAS points. There was improvement in 6 TMJs, there were no changes in 9 TMJs, and the pain did not worsen in any TMJ. The average change in the intensity of the unprovoked pain was −0.67 ±0.98 VAS points (Me = 0) and was statistically significant (p < 0.05).
Articular pain assessed by the patient immediately after the physical examination decreased after I-PRF administration and 2 weeks of follow-up in 21 (47.7%) TMJs, remained unchanged in 21 (47.7%) TMJs, and worsened in 2 (4.5%) TMJs. On average, the pain provoked by the examination changed by −1.16 ±1.90 (p < 0.05) (Figure 1).
Of the 23 non-respondent TMJs, 2 showed a deterioration of 1 and 2 VAS points. The first patient showed no contralateral change in the provoked pain domain and no change bilaterally in the spontaneous pain. The other patient was injected unilaterally and showed an improvement of −1 VAS point in the assessment of the spontaneous pain.
The respondent TMJs showed a decrease in the provoked pain up to −8 VAS points in a patient injected unilaterally. The same patient rated the spontaneous joint pain both before and after the intervention at 10 VAS points, which showed no change in this domain. The mean improvement in the joint pain measured after the physical examination in the group of the respondent TMJs was −2.57 ±1.89 (Me = −2).
In the Wilkes II subgroup, the provoked articular pain score varied from −4 to 1 VAS points. Improvement concerned 14 TMJs, in 14 TMJs there were no changes in pain intensity, and 1 case of deterioration was observed. The average improvement was −0.86 ±1.22 VAS points (Me = 0) and was statistically significant (p < 0.05).
In the Wilkes III–V subgroup, the articular pain score varied from −8 to 2 VAS points after the physical examination. Improvement concerned 7 TMJs, 7 TMJs showed no changes in pain intensity, and 1 case of deterioration was recorded. The average improvement was −1.73 ±2.76 VAS points (Me = 0). It was statistically significant (p < 0.05).
The mean pain intensity values for the masticatory muscles, head and neck were 3.86 ±2.47 (Me = 3), 2.75 ±2.49 (Me = 3) and 2.41 ±2.41 (Me = 2), respectively, before the intervention, and 3.86 ±2.59 (Me = 3), 2.75 ±2.68 (Me = 2) and 2.48 ±2.09 (Me = 2.5) after the intervention, without statistically significant differences (p = 1.000, p = 1.000 and p = 0.700, respectively) (Figure 1).
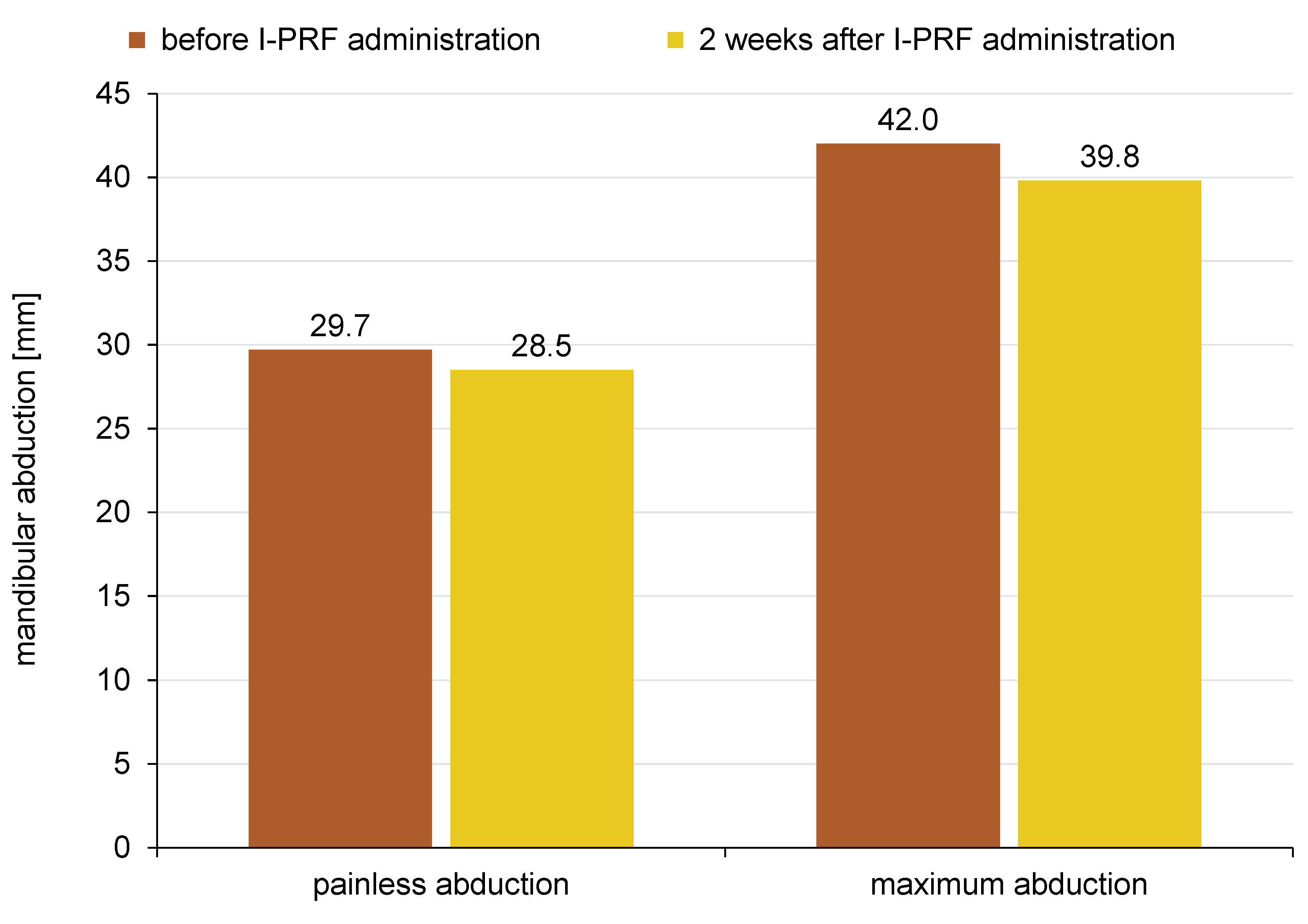
The range of painless jaw abduction changed by an average of −1.2 ±6.8 mm (Me = 0 mm) as compared to the pre-intervention value. This change was not statistically significant (p = 0.220). The maximum mouth opening changed statistically significantly (p < 0.05) by an average of −2.2 ±5.8 mm (Me = −1 mm) (Figure 2).
No adverse events were observed at the recipient sites (TMJs). Some patients reported transient pain and bruising at the donor sites (elbow bends), which did not differ from typical symptoms after venous blood collection from this area.
Discussion
A single administration of I-PRF to TMJ statistically significantly reduced articular pain at a 2-week follow-up by −0.5 to −1.2 VAS points, depending on the assessment method. Between 39% and 48% of Wilkes II–V patients reported the alleviation of pain after a single intervention, and the non-respondents experienced no change in pain intensity or experienced worsening pain (5–14% of the patients). The deterioration did not exceed 2 VAS points. Regardless of the measurement method, the range of jaw mobility slightly decreased at a 2-week follow-up.
The sources of potential bias were: (1) a small sample size; (2) the lack of control group; (3) a short follow-up period; (4) the open-label design; and (5) subjective pain measures. The small study sample was due to recruitment limitations, which was open for 6 months, and included patients eligible for the study and willing to participate in it. All other limitations resulted from the pilot nature of the study. Moreover, the study included patients with general diseases, which could have increased the heterogeneity of the results.
Differences in the assessment of the intensity of the spontaneous pain and the assessment of the pain provoked by a physical examination were up to 10 VAS points at the same visit. The average differences between these variables were 2.36 (SE (standard error) = 0.48; p < 0.05) and 3.07 (SE = 0.38; p < 0.05) VAS points before and after the intervention, respectively, with the provoked pain lower each time. Although the pain associated with performing daily activities is of primary importance to the patient, it can be assumed that the assessment after a specific physical examination protocol may be more repeatable.
The individual consideration of treatment effectiveness allows us to note that despite the satisfactory difference in averages, the number of non-respondent TMJs is significant and cannot be underestimated. Our own experience and that of other researchers indicate that many patients respond to injection therapy only after a series of administrations, and the initial lack of effect does not mean failure.20, 21, 24, 25 In our material, a slight increase in pain (up to 2 VAS points) was observed in some patients. It is believed that initially, intra-articular intervention causes the mechanical irritation of the tissues, which results in inflammation.26 This theory is also supported by a slight, statistically significant decrease in the range of jaw mobility in the study group. Intra-articular injections generally increase the range of jaw abduction, but initially, it may be slightly limited.27
The equal average values of muscle pain and headache observed in the study sample during the 1st and 2nd medical interviews are coincidental. The intensity of both types of pain in individual patients changed slightly, increasing and decreasing. However, in both domains, the sums of the VAS scores before and after the intervention turned out to be equal and gave equal means.
In the current state of knowledge, there is a solid theoretical basis for using subsequent generations of centrifuged blood products.24, 28, 29, 30 Injectable PRF seems to have a more favorable composition than its predecessors, plasma rich in growth factors (PRGF) and PRP.24, 28, 29, 30 Primary research on the intra-articular administration of I-PRF into TMJ is summarized in a review and presents promising results.14 These encourage future clinical trials on I-PRF. Larger samples, control groups and longer follow-up periods will be crucial to determine the long-term safety and efficacy of the treatment in question.
Another task is to search for the most effective protocol for administering I-PRF. The number of administrations, the time interval between them, and the appropriateness of preceding the first or each administration with arthrocentesis require clarification. This study proposed the least invasive protocol, i.e., the injection of an I-PRF amount smaller than the volume of the articular cavity, without additional burdensome co-interventions, such as administering an anesthetic or rinsing the joint. The study showed that 86–95% of patients experienced improvement or no deterioration, which justifies the search for a more extensive protocol. First of all, using a series of injections is worth considering.
Conclusions
A single injection of I-PRF into the articular cavity of TMJ brings statistically significant joint pain relief, regardless of the method of its examination. These results and the lack of reported complications provide rational grounds to consider the administration of I-PRF intra-articularly in patients with TMJ pain. A single injection of I-PRF into TMJ revealed no statistically significant effect on muscle pain, headache and neck pain.
Trial registration
The study protocol was registered in the ClinicalTrials.gov database: NCT05883982.
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee at the Świętokrzyska Chamber of Physicians, Kielce, Poland (1/2022-VIII). Informed consent to treatment and to participate in the study was obtained from each patient before enrollment in the study.
Data availability
The datasets supporting the findings of the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.