












Abstract
Background. Dentists are the first healthcare professionals to identify cases of domestic violence and abuse (DVA) with head and neck injuries.
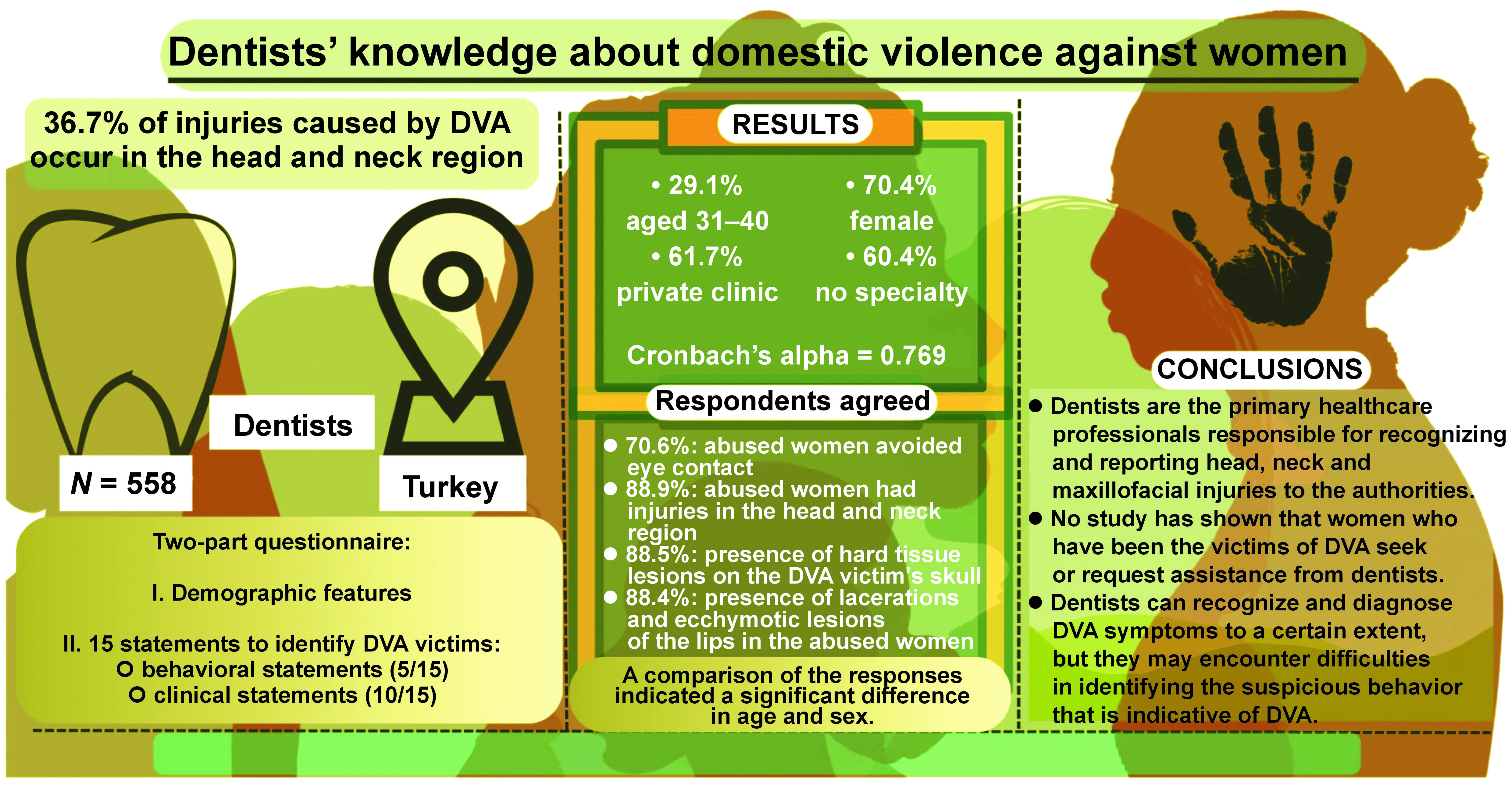
Objectives. The aim of this study was to assess dentists’ knowledge regarding behavioral and physical findings in female victims of DVA.
Material and methods. The study included 558 volunteer dentists who completed a two-part questionnaire designed to assess their knowledge and awareness of DVA against women. The first part of the questionnaire inquired about the participants’ demographic data, including age, sex, specialty, and the duration of professional practice. The second part assessed 15 statements on a 5-point Likert scale, concerning both behavioral (5/15) and clinical aspects (10/15) of DVA. For each statement, if a minimum of 70% of respondents selected the same option, it was interpreted as being agreed upon by the participants. The level of statistical significance was set at p < 0.05.
Results. Most of the participants were between the ages of 31 and 40 (29.1%). The study sample was predominantly female (70.4%), with 57.2% of the participants being married. The statement “Abused women tend to avoid eye contact” had the highest agreement rate (70.6%) for the behavioral assessments. However, the participants were mostly “undecided” on the remaining 4 statements in this section. In contrast, the agreement rate for 5 statements related to the clinical assessment of head, neck and intraoral injuries exceeded 70%. One-fifth of the behavioral assessment statements and half of the clinical assessment statements were negatively correlated with the age of the participants (p < 0.05).
Conclusions. The findings of this study indicate that dentists can recognize and diagnose DVA symptoms to a certain extent. However, they may encounter difficulties in identifying the suspicious behavior that is indicative of DVA.
Keywords: women, abuse, dentist, domestic violence, behavioral assessment
Introduction
The World Health Organization (WHO) defines violence as “the use of force that is likely to result in injury or loss to oneself, another person, a group, or society”.1 Although abuse is a public health problem that affects individuals, families and legal systems, it is the attitudes and behaviors of individuals that influence the physical, developmental and psychosocial well-being of others.2 Those at risk for violence and abuse include women, children, migrants, and individuals with various forms of vulnerability and discrimination, such as those in the LGBT+ community.3, 4 Several factors have been shown to influence violent behavior, including impulsive disorders, certain mental illnesses, trauma, inadequate cultural codes, inadequate education, poverty, unemployment, and patriarchal structures.4, 5
Women are subjected to domestic violence and abuse (DVA), especially in male-dominated societies, simply because of their gender. This social problem has existed since ancient times, from the moment that human beings first emerged into the world. According to the WHO, 35% of women globally are exposed to DVA.2 While DVA against women has been recognized as a violation of human rights for over 30 years, it is also a manifestation of historically unequal power relations between men and women. This phenomenon is observed globally and can be observed in every country and community.6
Domestic violence and abuse is associated not only with physical harm but also with psychological harm.2 Depending on the nature and extent of trauma, DVA can lead to adverse health consequences such as physical injuries, mental disorders, sexually transmitted diseases, and chronic diseases affecting various parts of the body. Additionally, cases of disability and death associated with limb loss have been reported in affected individuals.7
Previous studies have reported that injuries resulting from DVA occur with a frequency of 36.7% in the head and neck region.8 Oral and maxillofacial injuries are examined under the category of head and neck injuries. The most common type of head and neck injuries is a fracture of the teeth and/or jawbones, with the incisors being the most commonly damaged teeth.9 In addition, ecchymosis, swelling, lacerations, and rupture in the oral mucosa, temporomandibular joint problems, tooth mobility and migration, difficulty in chewing and speaking, restricted mouth opening, or tooth loss may occur.10 In cases of DVA, dentists have the responsibility not only to examine the victim but also to report the matter to the law enforcement authorities.11
Based on the assumption that dentists, who have medical and legal responsibilities, are competent to distinguish DVA-subjected women, the primary aim of the study was to determine the level of dentists’ knowledge about this issue.
Material and methods
The protocol of this cross-sectional, questionnaire-based study, conducted between January 3, 2022 and March 14, 2022, was approved by the Ethics Committee for Non-interventional Research of Istanbul Aydin University, Turkey (decision No. 2021/648).
Sample size and population
A power analysis was conducted based on the population of registered, actively practicing dentists in Turkey. The sample size was calculated based on the population of 43,199 dentists registered with the Turkish Dental Association, with a 5% margin of error and a confidence level (CI) between 90% and 99%. The study was to be completed with 298 dentists at a 90% CI or 384 dentists at a 95% CI. To increase the reliability of the study, 558 volunteers, registered as members of the Turkish Dental Association, were invited to participate in the study by completing a questionnaire that evaluated their knowledge and awareness of DVA against women.
All participants included in the study were required to have worked as a dentist for a minimum of 1 year, be a native Turkish speaker, be a member of the Turkish Dental Association, and volunteer to participate in the study.
Data collection
The data collection form, which was presented to the participants, was designed as a two-part questionnaire. The first part of the questionnaire was related to the demographic characteristics of the participants, including age, sex, marital status, the duration of professional practice, specialty, the type of workplace, and the city of work. In the second part, participants were invited to complete a recently developed questionnaire about DVA against women that contained a total of 15 statements within 2 distinct subdomains, structured based on the relevant sources (Table 1).12 This questionnaire was designed to evaluate the participants’ knowledge and awareness of DVA against women. The questionnaire statements were prepared based on the relevant studies, in Turkish and English, generated by using the keywords “domestic violence,” “abuse,” “head and neck injuries,” and “dentistry.” The participants were invited to answer the questions using a 5-point Likert scale, with scores corresponding to the following statements: 1. I strongly disagree; 2. I disagree; 3. I am undecided; 4. I agree; 5. I strongly agree.
The statements evaluating the level of dentists’ knowledge were developed and consulted upon with a panel consisting of an oral and maxillofacial surgeon, an oral and maxillofacial radiologist, a periodontist, a dentist, a psychiatrist, and a clinical psychologist. The questionnaire was based on Lawshe’s technique.13 The developed questionnaire was sent via e-mail to 5 randomly selected dentists who were not participating in the study and were employed at the Dental and Oral Health Application and Research Center of Istanbul Aydin University. After receiving the dentists’ feedback, the questionnaire was revised to incorporate minor changes. Subsequently, the Google Forms link to the questionnaire was forwarded to all registered members of the Turkish Dental Association via the member e-mail system. In order to prevent bias and avoid repeated inclusion of participants in the study, one of the study authors (SEM) had access to the list of participants. The procedure was conducted in compliance with the relevant data protection regulations (Turkish Personal Data Protection Law No. 6698).
Statistical analysis
The statistical analysis was performed using the IBM SPSS Statistics for Windows software, v. 24.0 (IBM Corp., Armonk, USA). Descriptive statistics were presented as numbers and percentages for categorical variables. Cronbach’s alpha, the internal consistency test for reliability analysis, was used, and an α value of ≥0.7 and <0.8 was considered acceptable. In the case of independent groups, the ratio was compared using the χ2 test. Spearman’s correlation analysis was conducted to observe the nature of the relationships between the variables. The results were analyzed with a 95% CI and a significance level of p < 0.05.
Results
The majority of dentists who participated in the study were between 31 and 40 years of age (29.1%), while the lowest level of participation was among those aged ≥51 years (21.6%). The study sample was predominantly female (70.4%), with 57.2% of the participants being married. The majority of the participants worked in Istanbul (58.2%), and 61.7% worked in private or outpatient clinics; 38.0% of the participants have worked as dentists for 1–10 years, 31.3% had been in their profession for 11–20 years, and 60.4% had no specialty (Table 2).
The responses to the second part of the questionnaire are summarized in Table 3. The internal consistency of the questionnaire was determined with Cronbach’s alpha of 0.769. With regard to statements 1 and 7 (St. 1 and St. 7), most of the respondents (70.6%) claimed that abused women avoided eye contact, while 88.9% agreed that female abuse was evident by the presence of bruises and injuries at the head and neck region (Table 3). Additionally, the presence of hard tissue lesions at the base of the patient’s skull (St. 8; 88.9%), and the presence of hemorrhages, lacerations and ecchymotic lesions of the lips (St. 9; 85.4%) were identified as indicators of abuse by the majority of the participants (Table 3).
A statistically significant difference was observed in response rates for St. 7 (p = 0.001), St. 8 (p = 0.032), St. 9 (p = 0.006), St. 10 (p = 0.004), and St. 13 (p = 0.003) in relation to age (Table 4). With regard to the remaining statements, no statistically significant difference was identified with respect to the age of the participants and the duration of professional practice (p ≥ 0.05). The proportion of “I disagree” responses was high among the participants older than 50 years for St. 7–9 and St. 13 (p < 0.05), while the proportion of “I am undecided” responses was high among participants below the age of 31 for St. 7–9 and St. 13 (p < 0.05). The proportion of “I strongly disagree” responses for St. 10 was high among participants older than 50 years, whereas the proportion of “I strongly agree” responses was high among those below the age of 31.
As shown in Table 4, a statistically significant difference was observed in response rates for St. 7 (p = 0.020), St. 8 (p = 0.022), St. 9 (p = 0.006), St. 10 (p = 0.049), and St. 13 (p = 0.034) in relation to the duration of professional practice. Accordingly, the proportion of “I disagree” responses among the participants who had been in the profession longer than 30 years was the highest for St. 8, St. 9 and St. 13 (p < 0.05). Moreover, for St. 7, St. 8 and St. 13, the proportion of “I am undecided” responses was the highest among the participants with less than 11 years of experience (p < 0.05). With regard to St. 10, the proportion of “I strongly disagree” responses among the participants with over 30 years of experience and the proportion of “I strongly agree” responses among the participants with less than 11 years of experience were the highest.
A comparison of response rates according to specialty revealed that only St. 4 and St. 5 of the behavioral assessment statements (p = 0.014 and p = 0.024, respectively) and all of the clinical assessment statements (except for St. 9 and St. 14) were significant (p < 0.05). The responses to the statements did not differ significantly with respect to sex (except for St. 7–10 and St. 13), marital status (except for St. 7), type of workplace (except for St. 13), and city of work (p ≥ 0.05) (Table 5, Table 6).
Table 7 shows that St. 1, St. 7, St. 8, St. 9, St. 13, and St. 15 were negatively correlated with age (p < 0.05), while St. 7, St. 8, St. 9, and St. 13 demonstrated a negative association with the duration of professional practice (p < 0.05). All behavioral assessment statements and the remaining clinical assessment statements showed no correlation with the duration of professional practice (p ≥ 0.05).
Discussion
All individuals can be victims of violence, irrespective of their level of education or socioeconomic status. All instances of domestic violence represent a global health problem and are a violation of women’s rights.14 Women who are subjected to DVA exhibit anxiety or unusual behaviors during routine dental examinations and show the effects of trauma in the acute phase.15 Domestic violence and abuse can take many forms, including neglect, as well as physical, sexual, or psychological violence. The presence of physical findings such as edema, skin bruises, fractures, cuts, burns, and scalp injuries can serve as diagnostic and investigable symptoms. As dentists do not frequently encounter cases of DVA in routine clinical practice, their ability to diagnose potential incidents of DVA is limited when patients do not disclose the cause.16
The analysis of the behavioral assessment responses (St. 1–5) revealed a deficiency in the participants’ understanding and awareness of the psychological state of the abused women. Moreover, it is concerning that when participants encountered a woman who was distracted (St. 4) or unaware of her identity, location, or time (St. 5), they were uncertain as to whether the abuse had occurred. When a person is disoriented or confused to the point of being unaware of their own identity, any healthcare professional would be wise to assume that the individual could have been the victim of a violent or abusive act or may require urgent medical attention. Although the psychological evaluation of the DVA victim is not the primary responsibility of the dentist, it is important to recognize that behavioral findings can shed light on clinical findings.
A recent study by de Macedo Bernardino et al. demonstrated that physical assault against women was more prevalent than other forms of DVA (85.2%), and that women were more likely to be abused in their own homes (74.2%).17 The authors found that 45.8% of cases exhibited trauma to the oral and maxillofacial regions, characterized by injuries. Other studies have reported that trauma to the oropharyngeal area was associated with other instances of violent acts that affected an individual’s quality of life, resulting in scarring, difficulty in mastication, or a tendency to avoid close relationships with other men.18
A study conducted in South Asia revealed that 50.4% of women who were victims of DVA had frequent bruises, abrasions and lacerations of the jaw.19 Although facial and soft tissue injuries are typically considered serious, they can have aesthetic and functional consequences for women who are victims of DVA.20 A study conducted in 22,822 Turkish households (88% response rate) with women aged 15 to 59 years found that 39% of the women had experienced physical DVA.21 According to the results of the 2015 survey on domestic violence against women in Turkey, 36% of women had been subjected to physical DVA.22 The results of the abovementioned studies demonstrate that DVA remains a serious problem in developing countries.19, 20, 21, 22
The responses given in this study to the statements about the clinical findings show the competence of dentists in recognizing cases of DVA. There was a substantial consensus among participants in response to statements regarding the extraoral areas of the head and neck trauma (St. 6–8), indicating a high level of familiarity with the injured body region. There was a strong agreement among participants for St. 9 and St. 13, which pertained to clinical assessments of both the intraoral and perioral areas. A consensus was reached for St. 11 and St. 15, suggesting that these statements were accepted by the majority of the participants (≥60%). On the other hand, the rate of undecided respondents, which exceeded 25% for both statements, should be taken into account when interpreting the outcomes. With regard to the clinical assessment statements, half of the participants agreed upon St. 14. However, more than one-third of the participants were undecided and could not make a clear assessment of the case described in this statement. The majority of the participants disagreed or were undecided on their response regarding St. 12. Therefore, it was assumed that either the content of St. 12 was not clearly defined to the participants or that the participants responded to this statement with connotations of some clinical conditions other than those described in St. 12. The findings of this study indicate that dentists are capable of detecting physical symptoms in women who are likely to be victims of DVA. However, even professionals with high sociocultural and educational qualifications may encounter difficulties in recognizing behavioral changes associated with DVA.
Many clinicians refer to the process of screening for DVA as “opening Pandora’s box”.23 Clinicians state that the observation of the victim’s behavior is a key factor in diagnosing the presence of abuse,24 but many medical professionals believe this is not common among their patients.25, 26 In some studies, the majority of women indicated that they would prefer medical professionals to ask them directly about the abuse or to respond to the victim’s signs.27 The majority of dentists (87%) reported that they had never treated such patients, 18% stated that they had never encountered a patient with apparent head and neck trauma, and 23% indicated that cases of DVA were not within their scope of practice.28
Despite the existence of different sub-social groups in Turkey, the Turkish family structure is mostly patriarchal. The members of the family perceive this structure as different and unique when compared to the rest of society. For this reason, women who are subjected to DVA often accept the situation in silence, fearful of further damaging their families. In cases where clinical findings point to DVA, the victim’s reluctance to disclose the truth may result in health professionals avoiding formal reporting. On the other hand, in cases where DVA is disclosed, they could, unfortunately, be ignored and disregarded by some medical, legal and social authorities due to the belief that reporting the issue might negatively impact the image of the Turkish family structure. Therefore, it should be anticipated that the sociocultural characteristics of the society in which the participants were brought up will also be reflected in their responses.
A substantial number of women who have experienced abuse require dental treatment. Dentists, given their focus on the orofacial area, play an important role in identifying such women and ensuring that they receive the necessary assistance.29, 30 Many studies have shown that training on this subject improves dentists’ understanding and changes their attitude towards DVA.31, 32 Dentists need to pay attention to the signs of DVA and provide support to those who have been victimized. It has been reported that healthcare professionals who have encountered cases of DVA in their professional practice have difficulty reporting these cases to the relevant authorities.10 Although approx. 6,000,000 people in the United States are affected by this problem, the actual reporting rate is quite low.33 While there are many causes for this under-reporting rate, the main reason is the inadequate training of healthcare professionals in recognizing and diagnosing DVA. In a study by McDowell et al., it was found that physicians were uncertain about the procedure for reporting suspected cases of abuse when they encountered them.34 As a necessary consequence, the authors recommend that educational courses and practical training with a multidisciplinary perspective be introduced into the curriculum to establish or improve dentists’ proficiency in assessing the psychological, social, legal, and physical aspects of sensitive cases such as DVA.
Limitations
Despite the strengths of our study, it has some limitations. Given that the target population was dentists and the objective was to achieve a high participation rate, not all aspects of DVA against women were assessed. Although we informed all participants that the study was designed not to evaluate individual knowledge levels, the structure of self-reported responses in the study could not entirely exclude the idealistic approach. Considering that the number of female dentists in Turkey is quite high, another limitation of this study is the possibility of selective perception bias due to the high proportion of female participants. The Turkish family structure and sociocultural factors may have influenced the responses and introduce bias. In this regard, the potential influence of geographical and sociocultural factors on the external validity of the results should be considered. Thus, the outcomes may not be generalizable to dentists in other countries.
Conclusions
In comparison to other healthcare professionals, the level of responsibility attributed to dentists in the context of DVA against women is quite low. This situation calls for interdisciplinary training. When confronted with suspicious situations concerning violence, dentists do not fully comprehend their potential role in preventing more serious assaults. No study has shown that women who have been victims of DVA seek or request assistance from dentists. Dentists are the primary healthcare professionals responsible for recognizing and reporting head, neck and maxillofacial injuries to the authorities. The identification of women who have been victims of DVA enables dentists to provide the necessary care and protection to such individuals.
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee for Non-interventional Research of Istanbul Aydin University, Turkey (decision No. 2021/648).
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.