Abstract
Background. During the coronavirus disease 2019 (COVID-19) pandemic, about 81% of the world’s population moved their workplace to a home office.
Objectives. The main objective of this cross-sectional pilot study was to determine the impact of working and/or learning from home during the COVID-19 pandemic on the head, the neck and orofacial health in university students, faculty and staff.
Material and methods. Participants from 4 universities were recruited for an online survey. The survey included 33 questions related to demographics, health issues before and during the lockdown, work/study from home, and the awareness of the health effects of the lockdown. Descriptive statistics and single logistic regression analysis were employed.
Results. A total of 96 subjects aged 26 ±10.5 years participated in the study. Of these, 60% did not consider their home workstation to be adequate. The development of new symptoms or the worsening of the pre-existing symptoms was observed in 67%, 24%, 59%, and 37% of the participants with regard to neck pain, temporomandibular joint (TMJ)-related issues, headaches, and parafunctional oral habits, respectively. In addition, 87% of the respondents reported that their oral habits were aggravated by neck pain and a bad posture. As compared to the faculty and the staff, the students were more likely to experience headaches or the exacerbation of the pre-existing headaches during the pandemic. In the survey, 91% of the participants reported an increased awareness of the impact of the lockdown on their head and neck, and orofacial health.
Conclusions. The present study helps understand the self-perceived effects of working and/or learning from home during the COVID-19 pandemic, and may facilitate implementing the appropriate models of treatment of the craniocervical-mandibular region during a pandemic.
Keywords: orofacial pain, COVID-19 pandemic, pandemic lockdown, head and neck posture
Introduction
In the middle of March 2020, the world declared a mandatory lockdown due to the coronavirus disease 2019 (COVID-19) pandemic. Consequently, universities implemented remote learning and teaching methods. University students, faculty and staff had to study/work from home. It was estimated that 81% of the world’s population transitioned from onsite to remote work in a home office during the lockdown.1 Although work from home ensured comfort and safety, it also resulted in many adverse effects on physical and mental health.2 A decrease in physical activity, increased sitting time and a decline in mental well-being are evidenced in self-report studies conducted among university students in the United States, the United Kingdom, Australia, Italy, and Spain.3, 4, 5, 6, 7
The COVID-19 pandemic was found to cause an increase in orofacial pain, including the intensification of bruxism (tooth grinding and/or clenching) and temporomandibular disorders (TMD).8 In the long run, the lack of an ergonomic office set-up at home may promote a faulty posture, which makes an individual more susceptible to neck pain, TMD, and orofacial pain.1 In a self-report study, 57% of participants declared using a four-leg kitchen chair without an adjustable height feature as part of their home office furniture.8 About 86% of respondents reported using a single non-adjustable tabletop, and the majority reported using a chair with a concave back. Only 60% of participants used in their home office a monitor that had adjustable height.8 Alterations in the head and neck posture can affect the forces exerted by the neck muscles, which must work harder to support the head in an unfavorable position.9 The forward head posture (FHP) can alter the position of the mandible, which in turn displaces the temporomandibular joint (TMJ) condyles to a more posterior position, compressing the innervated area of the joints and causing pain.10 In addition, the hyperactivity of the masticatory muscles has been observed for FHP when compared to a normal head posture.10
During the COVID-19 pandemic, an increased incidence of depression, anxiety and parafunctional habits was noted. Studies show a strong correlation between adverse psychological effects and orofacial pain, including TMD.8, 11 Patients with TMD were found to experience higher levels of stress, and report higher intensity of pain and pain-related disability.12, 13 An increase in myofascial pain in the masseter and temporalis muscles was observed in 78% of patients with TMD.14 Stress, anxiety and depression exacerbated parafunctional habits and sleeping difficulties, which are associated with TMD.14
University students are particularly vulnerable to stress, anxiety and depression due to the lack of coping mechanisms. Most university students live away from home15 and do not have a partner to help them manage their emotions, which may lead to higher levels of stress. University undergraduate students were affected differently by the COVID-19 pandemic than the working population, as the uncertain outlook added to their already stressful academic obligations.15 Additionally, university employees reported increased levels of stress and anxiety, and many admitted they lacked the proper coping strategies.16 The decline in their mental health was likely due to social isolation, managing their student’s emotions and having to monitor their children’ online learning at home.16
To the best of the authors’ knowledge, no previous study has explored the impact of the COVID-19 pandemic on the head, the neck and orofacial health in university students, faculty and staff. The objective of the present study was to determine the impact of working and/or learning from home during the COVID-19 pandemic on the craniocervical-mandibular system, including the head and neck posture, and the associated orofacial pain, including TMD, in university students, faculty and staff. It was meant to help understand the self-perceived effects of working and/or learning from home during the COVID-19 pandemic. The study may be used by clinicians to facilitate implementing the appropriate models of treatment, including the use of telehealth,17, 18 and the prevention of health-related problems involving the craniocervical-mandibular system in the period of a pandemic lockdown.
Material and methods
Study design
This cross-sectional, descriptive pilot study was approved by the Institutional Research Board at Florida International University, Miami, USA (approval No. IRB-21-0247), and followed the recommendations of the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Subjects and recruitment
A convenience sample of undergraduate and graduate students, faculty, and staff from 4 universities in the Miami-Dade County, FL, USA (Florida International University, University of Miami, Miami Dade College, and Barry University), participated in this study. The main aim of this survey was to generate hypotheses for future research; thus, a formal sample size calculation was not required. However, according to the literature on the sample size for survey studies,19, 20, 21 a sample size of approx. 100 participants is required if a 10% sampling error is accepted. Also, Krejcie and Morgan suggested that a sample size needed to be representative of a given population.22 In this context, a theoretical target population of 2,000 would require 322 participants. Since this was an exploratory pilot study involving 28% of this target sample, the size included was considered acceptable.
Recruitment posters were distributed around the university campuses, and the participants could access the survey through a QR code. The participants were also reached through social media platforms (Reddit, Facebook and Instagram) and email. The link to the survey was provided in the message to the potential participants. The survey was open for data collection from September 2021 to March 2022. Prior to completing and submitting the survey, the participants provided informed consent to participate in the study and authorized the researchers to analyze their responses. The participants were assured that no identifiable information would be published or released, and that participation was voluntary. In addition, they were informed that they would not receive any compensation for participating in the study.
Questionnaire
A questionnaire was created using the Qualtrics online survey software (Qualtrics, Provo, USA). The survey included 33 questions related to demographics, health issues before and during the lockdown, work/study from home, and the awareness of the health effects of the lockdown (the survey is available on request from the corresponding author). A variety of multiple-choice, ranking-scale and open-ended questions were included in the survey. The frequently used 5 multiple-choice alternatives (always, very often, sometimes, rarely, and never) were selected to improve the sensitivity of data and decrease bias. The final questions were chosen through discussions among the research team and were based on previous research evaluating the effect of the pandemic on orofacial pain, including TMD, and mental health.9, 12, 13, 14, 15 The main craniocervical-mandibular outcomes considered were neck pain, headaches, TMJ/jaw pain, and oral habits. The survey was reviewed and tested by the team by answering the questionnaire on Qualtrics to gather feedback for improvement and to refine the survey. Changes to the survey were implemented based on the received feedback. The questionnaire was considered to have face validity (based on the intuitive feeling that a measurement seems to be valid), and the assumption that the measurement is valid at face value was accepted.23 The online survey was designed to be completed in no longer than 10 min.
The survey contained questions related to the perceived stress, anxiety and depression based on the Perceived Stress Scale.24, 25, 26 These questions might help understand the potential relationship between the psychological effects of the COVID-19 pandemic and orofacial health, including the possible increase in orofacial pain and TMD.
Statistical analysis
Descriptive statistics were used to analyze the responses. Data was presented as the number of participants (n) and frequency (percentage). The open-ended question responses provided by some participants were also considered and presented under their respective topics. A cross-tabulation analysis was conducted using the Qualtrics analysis software. In addition, we explored univariate associations between some of the variables. The χ2 tests or univariate single logistic regression were employed to establish relationships between the onset/worsening of symptoms of neck pain, jaw pain, headaches, stress/anxiety, and oral habits and age, gender, the respondent status (students vs. faculty/staff), and the number of hours in front of the computer. The strength of the evidence against the null hypothesis (p-value) was interpreted based on the criteria proposed by Sterne and Smith.27 Increasing evidence against the null hypothesis was defined by decreasing p-values. All responses available for each of the questions were analyzed. The Stata® statistical software, v. 17, was used for all analyses.
Results
Demographics and characteristics
of the participants
A total of 96 subjects (N = 96) participated in this pilot study. The survey was completed by 96 subjects, but not all questions were fully answered by all. The majority of the participants were female (75.3%) with an age range of 18–69 years and an average age of 26 ±10.5 years. Of he total number of participants, 83.3% (n = 80) were students, and 16.7% (n = 16) were faculty and staff. The subjects’ demographics and characteristics and shown in Table 1.
Health issues before the lockdown
Before the lockdown, the majority of the respondents (54%) reported spending an average of 3–6 h per day in front of the computer. A total of 62% (n = 55) reported that they rarely or never had neck pain before the pandemic. Eleven percent (n = 10) reported having neck pain always or very often, and 27% (n = 24) reported experiencing it sometimes.
Only 14% (n = 13) reported having headaches always or very often before the pandemic. In contrast, 44% (n = 39) of the participants rarely or never had headaches before the pandemic.
The majority of the respondents (89%) reported rarely or never experiencing problems related to TMJs or jaw muscles before the pandemic. Only 8% (n = 7) self-reported that they had been diagnosed with TMD. No further information regarding the diagnostic tool and the professional who had made the diagnosis was collected. Only 14% (n = 11) reported always or very often experiencing bruxism (the grinding and/or clenching of the teeth). Over half of the participants, (58%, n = 43) reported rarely or never having parafunctional oral habits before the pandemic.
A total of 92% (n = 81) of the participants reported no history of TMD diagnosis or lock jaw. In relation to bruxism, 37% (n = 27) of the participants reported never having clenched or ground their teeth, and 22% (n = 16) reported infrequent clenching or grinding before the lockdown.
Home office changes and health issues during the lockdown
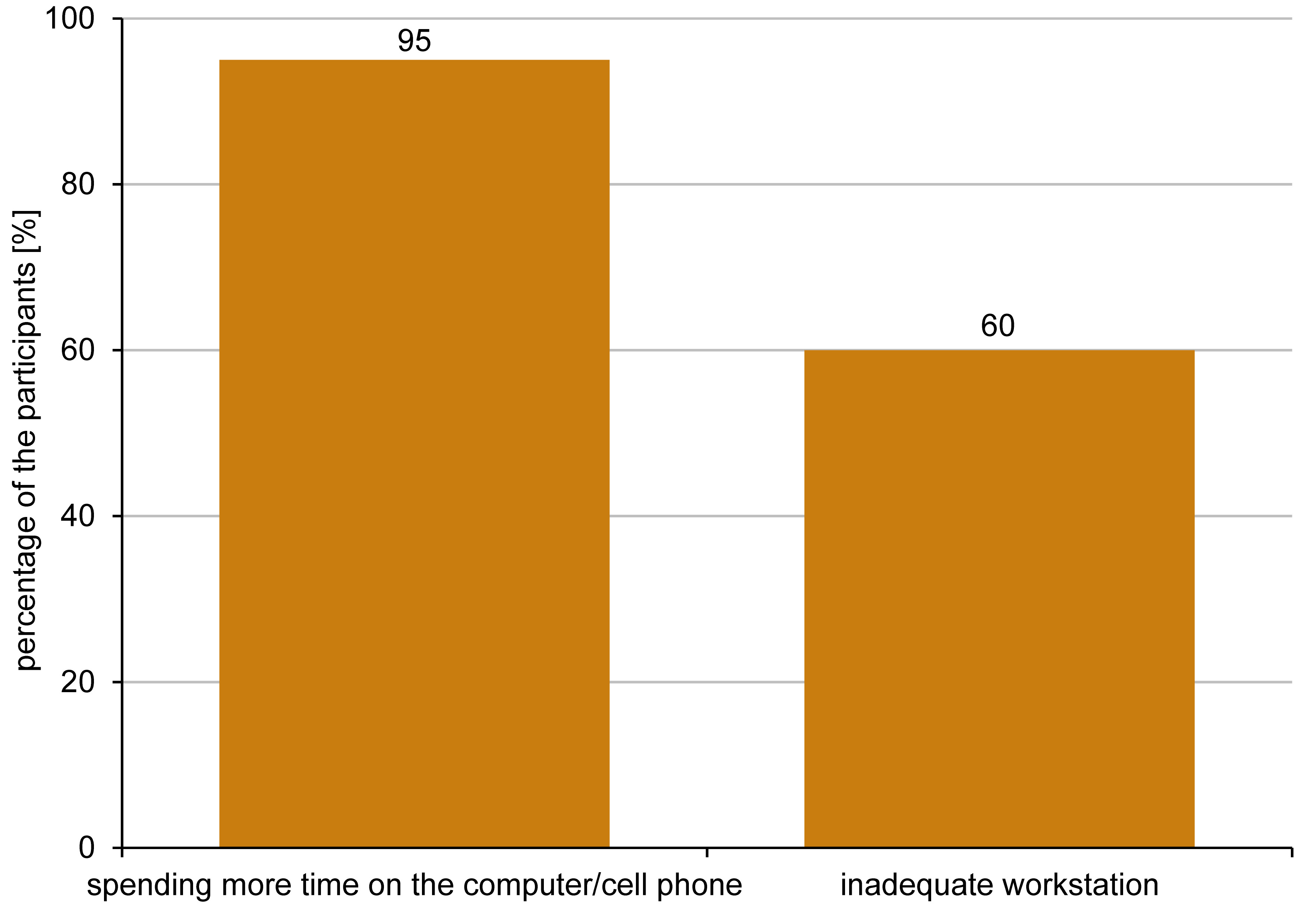
Of the total number of participants, 87% (n = 77) reported transitioning from onsite to remote work in a home office in full time, while 8% (n = 7) reported transition in half time after the pandemic started. Among those who reported moving their workplace to a home office, 95% (n = 79) reported that they felt they spent more time on their computer and cell phone than before the lockdown. A total of 84% (n = 73) reported spending at least 6 h in front of the computer per day during the pandemic. A total of 34% reported spending 8–10 h on the computer and the cell phone per day, while 22% reported more than 10 h. Additionally, about 60% (n = 50) of the participants felt that their workstation at home was not adequate for maintaining a proper posture in front of the computer (Figure 1). When examining the correlation between the time spent in front of the computer and symptoms in the head, neck and orofacial regions, it was found that the individuals who spent more than 6 h in front of the computer had 4.68 times higher odds of developing neck pain or getting worse neck pain during the pandemic (p = 0.012). Similarly, the subjects who spent more than 6 h in front of the computer had 4.79 times higher odds of developing headaches or getting worse headaches during the pandemic (p = 0.015) (Table 2).
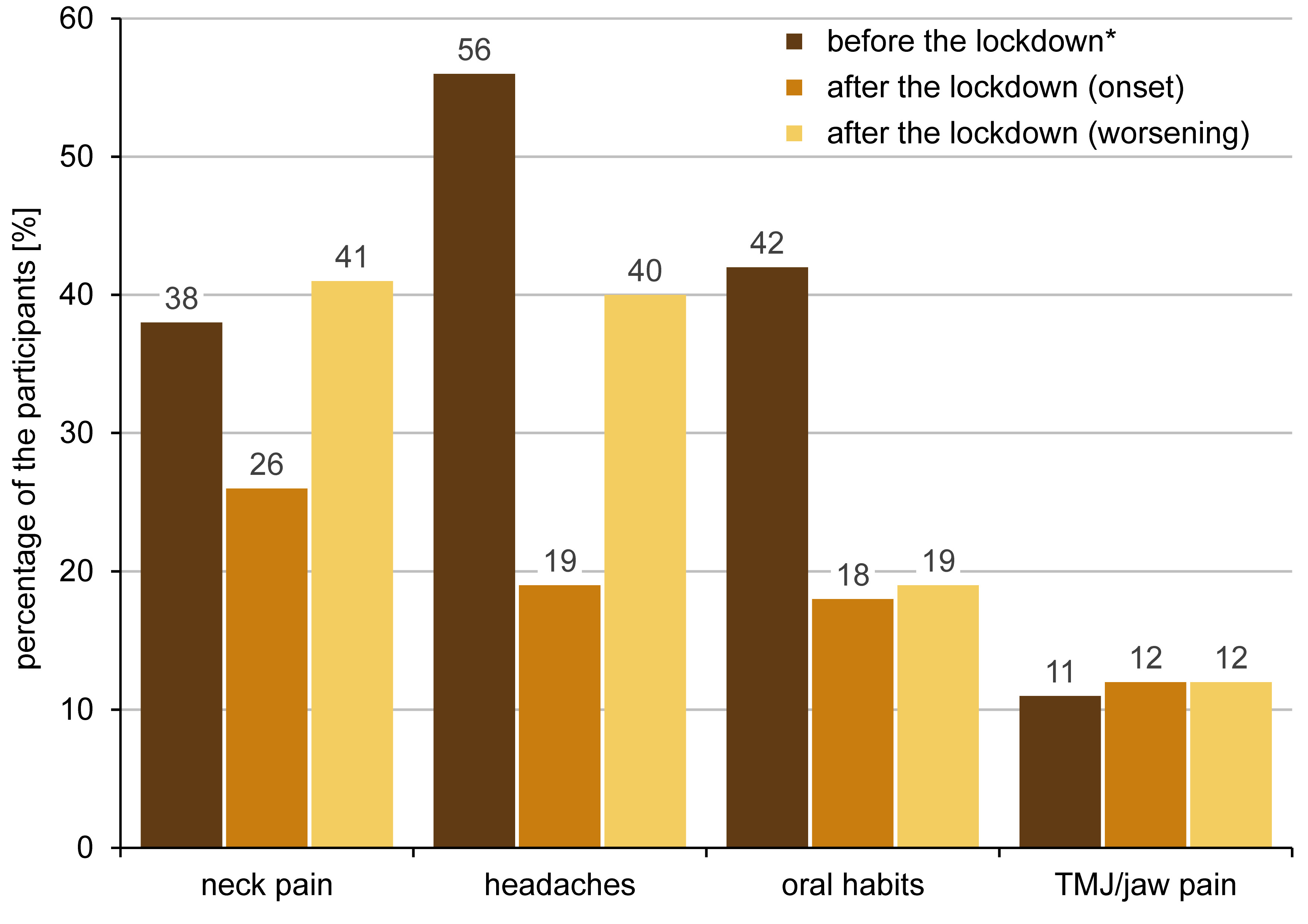
With the lockdown, 26% (n = 22) of the participants reported the onset of neck pain, and 41% (n = 35) reported the worsening of the already existing neck pain. Additionally, 37% of the participants reported the development or worsening of oral habits. The self-reported development of new symptoms and worsening of the pre-existing symptoms after the lockdown as compared to the state before the lockdown are shown in Figure 2. The graph illustrates answers “always”, “very often” and “sometimes” for before the lockdown data, and answers “yes, started during the pandemic” for after the lockdown (the onset of symptoms) data and “yes, my neck pain/headaches/oral habits/TMJ pain got worse during the pandemic” for the after the pandemic (the worsening of the already existing symptoms) data.
When examining the relationships between the onset/worsening of symptoms of neck pain, jaw pain, headaches, stress/anxiety, and oral habits and age, gender, the respondent status (students vs. faculty/staff), and the number of hours in front of the computer, weak evidence was found against the null hypothesis (of no association) in most cases. However, a significant association of the onset/worsening of headaches and stress/anxiety with gender was found. For example, during the pandemic, females were 3.33 times more likely to start with headaches or get worse headaches as compared to males (p = 0.021), and they were 3.08 times more likely to experience greater stress/anxiety (p = 0.037). There was moderate evidence against the null hypothesis, showing no significant association of the participant status (student vs. faculty/staff) with headaches. The students were 3.46 times more likely to start with headaches or get worse headaches during the pandemic than the faculty/staff (p = 0.060) (Table 2).
When asked whether their oral habits were aggravated due to neck pain or a slouched posture, 87% (n = 26) of the participants responded affirmatively. Additionally, when asked an open-ended question whether their TMJ/jaw pain was concomitant with neck pain, 5 out of 16 responded negatively. However, 9 were positive regarding the concomitant symptoms, with the answers including “Yes, I generally experience neck pain and jaw pain at the same time”, “I think jaw pain is a direct result of tension in my neck and shoulders, which is due to the extended periods of a poor posture”, “Yes, I think my posture affected my TMJ pain (I was always on the computer)”, and “I usually get a headache, neck pain and jaw pain contractions when spending too much time in front of a computer”. Two participants answered “I think TMJ/jaw pain was worsened by the stress related to my home situation” and “I believe it is because I started clenching my jaws and grinding my teeth more frequently”.
Stress, anxiety, sleeping difficulties,
and demotivation
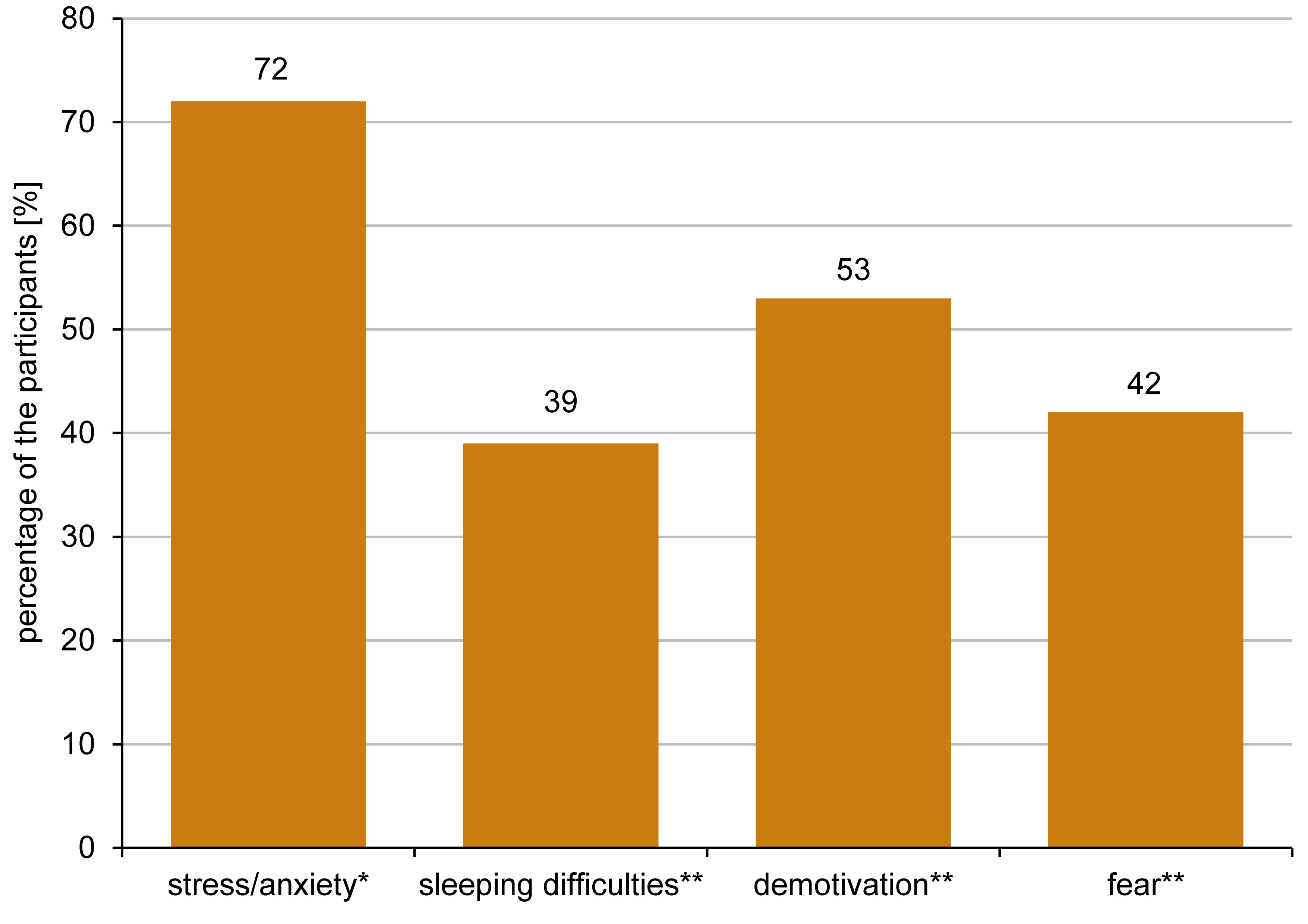
Most of the responders (72%, n = 59) reported experiencing increased stress, nervousness and/or anxiety since the beginning of the lockdown (answers “yes, very often” and “yes, sometimes”). Only 19.5% (n = 16) reported feeling the same, and 8.5% (n = 7) reported feeling more relaxed during the pandemic. As previously stated, females were 3.08 times more likely to experience greater stress/anxiety during the pandemic than males (p = 0.037).
Of the total number of respondents, 53% (n = 43) reported they became unmotivated to work/study from home (answers “yes” and “very often”). With regard to demotivation, 25% said “sometimes,” and 22% said “no”. Thirty-nine percent (n = 33) reported developing sleeping difficulties with the lockdown (answers “yes” and “very often”), while 38% said “no,” and 23% said “sometimes” in this regard.
When the participants were asked if they became fearful of their future regarding their studies/work, 42% (n = 34) reported “yes” or “very often,” and 23% responded “sometimes”. However, 68% (n = 56) were able to cope with the circumstances of the pandemic lockdown (answers “yes” or “most of the time”). Figure 3shows the effects of the lockdown on stress/anxiety, sleeping difficulties, demotivation, and fear, as reported by the participants.
Self-awareness
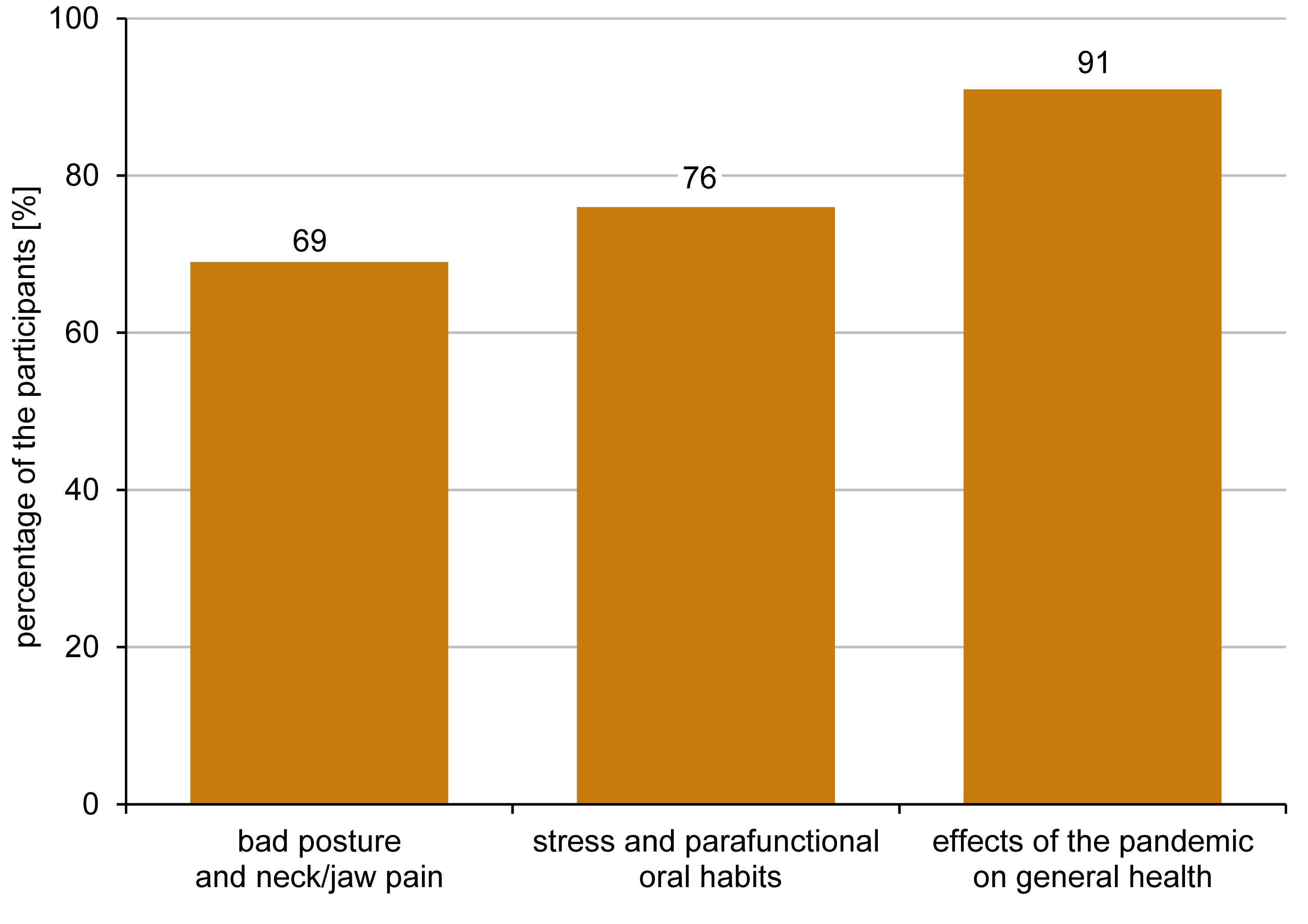
The questions related to self-awareness were collected at the end of the survey. When asked if they were aware that a bad posture could potentially cause neck pain and possibly pain to the head, including the jaw area, 31% (n = 25) of the participants responded “No”. Twenty-four percent (n = 19) of the respondents did not know that stress could cause parafunctional oral habits. After completing the survey, 63% of the participants agreed, and 28% somewhat agreed, that they were more aware of the possible impact of the COVID-19 pandemic on their general health, including the musculoskeletal conditions of the head and neck region (Figure 4).
Discussion
This study investigated the self-perceived impact of working and/or learning from home during the COVID-19 pandemic on the head and neck region and orofacial health of university students, faculty and staff in the Miami-Dade area in Florida, USA. The study also aimed to increase the awareness regarding the relationships between a bad posture, stress, parafunctional oral habits, and pain in the head and neck region, which might be aggravated during the lockdown.
The pandemic lockdown gave rise to health threats, economic uncertainty and social isolation, causing potential damage to people’s physical and mental health. According to the results of this study, 62% of the participants reported rarely or never experiencing neck pain, 44% rarely or never having headaches, 58% rarely or never having oral habits, and 89% rarely or never experiencing problems related to TMJ or jaw muscles before the pandemic. With the pandemic lockdown, the development of new symptoms or the worsening of the already existing symptoms, including neck pain, headaches, oral habits, and TMJ-related issues were substantial, as shown in Figure 2. Additionally, females were more likely to develop or get worse headaches, and be more stressed during the pandemic than males.
Most participants regarded their home workstations as inadequate for maintaining a proper posture. They reported a more slouched head and neck posture as compared to the period before the pandemic, as well as spending more time on the computer and/or the cell phone. The subjects who spent more than 6 h in front of the computer were more likely to experience the onset or worsening of neck pain and headaches during the pandemic. Filho et al. found that the number of work breaks and hours spent at the computer had a great effect on neck pain, even though no clinically relevant changes in the average neck pain intensity and neck disability were found.28 However, only 5 weeks of working from home was taken into consideration to investigate the effects on neck pain. The authors also found that there was very strong evidence that workstation ergonomics was poorer at home.28 It is important to mention that the results can be referred to home offices that are not necessarily related to the COVID-19 pandemic. According to some open-ended question answers from our study, some participants reported using the kitchen or dinner table, and even the bed or couch while working/studying at home, constantly looking down at the laptop screen, and not having a comfortable chair or a chair that provided support to their lower back. One participant mentioned feeling a significant worsening of shoulder pain during the pandemic and holding more tension in their shoulders and neck. This may have contributed to increased pain around the craniocervical-mandibular region, including neck pain, headaches and TMJ-related issues. On the other hand, another study showed improvement in headaches during the COVID-19 lockdown.29 According to the authors, the alleviation of migraines could be attributed to working from home and having fewer social responsibilities, as well as freedom to choose how to organize one’s schedule.29 Perhaps, the ability to adjust to changes while working from home also depends on an individual’s lifestyle and general level of adaptability. In this survey, nearly 9% of the participants felt more relaxed during the pandemic.
In addition, oral habits and TMJ/jaw pain were found to be correlated to neck pain and a bad posture, as reported by most of the participants. The increased level of stress/anxiety during the lockdown, as reported by 72% of the participants, and increased sleeping difficulties (40%), may have also contributed to a higher frequency of parafunctional oral habits and, in turn, TMJ-related issues. Dentistry students declared dissatisfaction with distance learning during the pandemic, which may have contributed to their increased levels of distress.30 In addition, in the present study, the students were more likely to start with or get worse headaches during the pandemic than the faculty and the staff. Previous studies have shown that the overwhelmingly quick transition from a normal lifestyle to a life of uncertainty during the pandemic lockdown could trigger increased levels of stress, anxiety and depression due to a fear of becoming infected with the virus, its impact on mental health and the concerns regarding personal finances.11, 12 Higher levels of psychological distress, anxiety and depressive symptoms were found in individuals with orofacial pain during the pandemic.31 Even though not evaluated in this study, symptoms of anxiety and depression may affect the adaptability of patients with orofacial pain, which may lead to suicidal behavior.32 Further studies are needed to examine the association between TMD/orofacial pain and suicidal behavior.32 Some participants reported worsened sleeping patterns, and some weight gain. However, 19.5% of the participants felt the same levels of stress, nervousness and anxiety before and during the lockdown, and 8.5% reported feeling more relaxed during the lockdown. Physical activity appeared to play a role in helping people better cope with the pandemic lockdown. According to open-ended question answers, some positive aspects of the lockdown reported by the participants included “Remote work has really made me deal with stress better”, “Focusing on physical activity and health more”, “The pandemic gave me years I needed to slow down and focus on improving my mental health. This has significantly improved my quality of life”, and “The pandemic motivated me to exercise more, and it helped me to cope with the pandemic”. The benefits of physical exercise are already acknowledged in the literature, and it is considered an effective approach to improving cardiorespiratory endurance in both people infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and non-infected individuals.33 Physical exercise can also improve antibody responses and the effects of the influenza vaccine.33 Identifying the activities performed by subjects to cope with the pandemic lockdown can be useful, and should be included in future studies.
Interestingly, 53% of the participants reported always or very often moving their jaw as a way to reposition the facial mask used during the pandemic. Of those reporting that their TMJ/jaw pain got worse during the pandemic, 71% admitted frequently adjusting the mask position in this way. Therefore, the use of masks may have increased the risk of worsening of the pre-existing TMJ/jaw-related problems. It is important to conduct additional studies on the effects of the use of masks on the repeated jaw movements and TMJ pain, as future pandemics are likely to happen. The increased awareness of the possible effects of mask use may help prevent mask-use-related issues.
In the present study, the majority of the participants agreed that the survey increased their overall awareness regarding the relationships between a bad posture, stress, oral habits, and pain in the head and neck region, which may be aggravated during the lockdown. This is important, as the risk of a new pandemic is higher now than ever before. Experts agree that the COVID-19 pandemic will likely not be the last one.34, 35 Therefore, we should learn from the lessons of the COVID-19 pandemic and make the necessary changes. The global health system should strengthen its capacity to prevent the effects of a lockdown and be prepared for the next public health emergency. This may involve putting more emphasis on physical activity, improving work ergonomics at home and increasing the awareness regarding the lockdown effects on health, including the head and neck posture and orofacial health. More investment in telehealth platforms is also recommended,36 as it can help support the above recommendations based on the results of the present study.
Limitations
This study presents some limitations. The response rate was limited, and the majority of the responders were students. Faculty and staff were represented by only 17% of the total group, which limits the representation of this population in the sample and, in turn, the generalizability of the study. The results of this study should be interpreted with caution because of the small sample size and low external validity. To ensure maximum participation, the survey was designed to be brief, taking no more than 10 min to be completed. However, the authors assume that the time period during which the data was collected may have affected the recruitment of participants. Students, faculty and staff were gradually going back to their in-person routines, and most faculty and staff continued working remotely for the majority of their time. Therefore, not all of them had access to the recruitment posters around the university. The recruitment method may have affected the participation of several potential subjects, even though it was not the only method used. Other strategies to increase participation should be considered in future studies. The conducted analysis was limited by the small sample size. With a larger sample, further analysis (i.e., regression) could be performed. Therefore, this is a pilot study indicating the effects of working and/or learning from home during the COVID-19 pandemic on university students, faculty and staff. This study is based on self-reported data, and therefore, it can affect the properties of the measurements, including clinical validity and reliability, and it may be subject to recall bias, since the participants had to remember some past, though recent, events. The variables studied, including a bad posture, neck pain, oral habits, and psychological effects, were limited by the participant’s knowledge and the clarity of the questions asked. This was a cross-sectional study, where data was collected at one point in time. However, the results of this study provide relevant information that can be used to guide more robust scientific research and the development of longitudinal studies, integrating further validated questionnaires, such as those for TMD or headache diagnosis, with larger sample sizes, and a better representation of faculty and staff. It can also be used to strengthen the prevention capacity with regard to the effects of a lockdown, based on the lessons learned from the COVID-19 pandemic.
Conclusions
This study helped understand the self-perceived effects of working and/or learning from home during the COVID-19 pandemic on the head and neck region and orofacial health. The findings revealed an increase in the onset or worsening of neck pain, headaches, TMJ/jaw pain, and oral habits in the university setting. The results may contribute to the development of the appropriate models of treatment of the craniocervical-mandibular region during pandemic lockdowns. The study also increased the awareness of the participants regarding the negative impact of the pandemic on physical and mental health, which may lead to decreased performance in work- or school-related activities.
Ethics approval and consent to participate
The study was approved by the Institutional Research Board at Florida International University, Miami, USA (approval No. IRB-21-0247). All participants provided written informed consent.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.