Abstract
Background. Periodontal diseases (PDs) are one of the most common chronic diseases affecting overall oral functions, and their association with adverse pregnancy outcomes (APOs) has been an area of interest since the late 90s.
Objectives. The present hospital-based case–control study aimed to find any association between maternal chronic periodontitis (CP) and preterm birth (PTB) and low birth weight (LBW) by comparing the periodontal parameters in patients with normal birth, PTB and LBW.
Material and methods. The participants of the study were females that had delivered a live baby (n = 1,200). They were classified as either cases or controls. The cases were defined as PTB if the delivery was before 37 weeks of gestation, and as LBW if the infant weighed <2,500 g. The others were controls. The intraoral examination, which included recording the periodontal status, was conducted within 3 days of delivery. Detailed medical history and demographic data were recorded for the determination of the confounding factors. The multivariable dependence of PTB and LBW on both the categorical and continuous data was analyzed using a multivariate logistic regression analysis. Adjusted odds ratios (AORs) with a 95% confidence interval (CI) for the risk of PTB and LBW were calculated.
Results. A strong association with PTB was found for a high plaque index (PI) score (AOR = 1.61; p < 0.001; 95% CI: 1.26–2.07) and a mean pocket probing depth (PPD) ≥4 mm (AOR: 4.32; p < 0.001; 95% CI: 3.09–6.02). A strong association with LBW was found for a high PI score (AOR = 2.02; p < 0.001; 95% CI: 1.43–2.83) and a mean PPD ≥4 mm (AOR: 8.70; p < 0.001; 95% CI: 6.01–12.59). A high PI score and a mean PPD ≥4 mm were independent risk factors for PTB and LBW.
Conclusions. The presence of deep pockets and inadequate plaque control in pregnant females increased the risk of APOs.
Keywords: adverse pregnancy outcomes, low birth weight, maternal chronic periodontitis, preterm birth
Introduction
Periodontitis is amongst the most prevalent chronic diseases globally, affecting approx. 743 million people, with an 11.2% prevalence of severe periodontitis.1 The majority of this population come from developing countries. Along with dental caries, periodontal diseases (PDs) are the most common chronic diseases affecting overall oral functions and reducing the quality of life; they have been identified as a global epidemic.2 A Global Burden of Disease (GBD) study revealed an average increase by 45.6% in the prevalence of chronic oral diseases from 1990 to 2010, which is comparable to other non-communicable diseases (NCDs), and adds to the financial burden of the individual.2 Periodontitis and the major NCDs, like heart disease, diabetes, cancer, and chronic respiratory disease, have common risk factors and social determinants.1 The association between periodontitis and the abovementioned diseases has been an area of interest since the early 90s.3, 4 Such an association has also been explored in a range of other diseases and conditions, including adverse pregnancy outcomes (APOs), chronic kidney disease, rheumatoid arthritis, dementia, metabolic syndrome, and certain forms of cancer.2 Many NCDs affect the body in the 3rd and 4th decades of life, but APOs affect newborns. Adverse pregnancy outcomes are a rising concern due to increasing neonatal and infant mortality rates despite medical care and treatment modality advancements.5 They include preterm birth (PTB), low birth weight (LBW), miscarriage, and early pregnancy loss. Preeclampsia and PTB are major causes of maternal, perinatal and neonatal morbidity and mortality.6
Periodontal infection and subsequent inflammation are not limited to the oral cavity. Bacteria and bacterial antigens are systemically dispersed via the pathway of the ulcerated sulcular epithelium3 and trigger significant systemic inflammation. Leukocytes, endothelial cells and hepatocytes respond to bacteria and virulence factors by secreting pro-inflammatory immune mediators, such as cytokines, chemokines and C-reactive protein (CRP). Soluble antigens from the periodontal inflammatory lesion may enter the bloodstream and react to form a macromolecular complex with the circulating antibodies. These immune complexes can be deposited at various sites in the body and give rise to acute and chronic inflammatory reactions.7
During the normal course of pregnancy, as gestation progresses, the amniotic fluid concentrations of prostaglandin E2 (PGE2) and inflammatory cytokines, such as tumor necrosis factor alpha (TNF-α) and interleukin (IL)-1β, rise steadily until reaching a critical threshold level that induces the rupture of the amniotic sac membranes, uterine contractions, cervical dilation, and delivery. The process can be modified by external stimuli, including infection and inflammatory stressors.8 It has been postulated that the levels of periodontal inflammatory mediators slowly increase and affect the fetomaternal unit.9 Also, there is evidence for the presence of periodontal pathogens in the amniotic fluid and the placental tissues.10, 11 It is an established fact that there is an increased tendency toward periodontitis during pregnancy due to the effects of hormones,12 which consequently affects the quality of life of pregnant females.13 A hospital-based survey revealed a 43% prevalence of periodontitis among pregnant females aged between 19 and 35 years.14
To our knowledge, no study investigating the association between APOs and chronic periodontitis (CP) in pregnant females has been published so far. Based on the prevalence of periodontitis in pregnant females and the evidence reviewed above, the present study was conducted in a single hospital14 to assess the association between CP in pregnant females and APOs.
Material and methods
The present case–control study was conducted in the Department of Obstetrics and Gynecology (ObGy) of the Civil Hospital, Ahmedabad, India. The study was approved by the Institutional Ethics Committee at the Government Dental College and Hospital, Civil Hospital in Ahmedabad (No. IECGDCH/S.10/2017 dated 18/3/2017), the Head of the ObGy Department and the Medical Superintendent of the Civil Hospital. The data was collected from 3 wards of the ObGy Department. The nature and purpose of the study were explained to all the participating patients, and written consent was obtained from all. The study is reported according to the STrengthening the Reporting of OBservational studies in Epidemiology (STROBE) statement.
Study design
The selected period for data collection was between April 2017 and December 2017. There were a total of 6 examiners divided into 3 groups of two, with 1 group assigned to each ward. One examiner reviewed the medical history of all patients who had delivered a live baby, while the other examiner conducted an intraoral examination after obtaining consent and considering patient comfort. All intraoral examinations were done within 72 h of delivery.4 The 2 appointed examiners per ward were blinded to the patient’s medical and dental records, respectively. A total of 1,500 medical records were examined, with 74 females not consenting to participation or a dental checkup and 226 excluded after reviewing their medical records. The data was collected for the remaining 1,200 patients. The prevalence of PTB and/or LBW cases for this population was unknown (Figure 1).
Inclusion criteria
A total of 1,200 females met the inclusion criteria based on medical records and case definition. The patients were aged 18–36 years, had given birth to a live infant and provided consent for an intraoral examination. Three examiners (NP, DG and RP) examined their medical records, and noted the demographic data and medical history, including the patients’ conditions during pregnancy and delivery, and the medical records of the infants. An obstetrician reviewed all medical data to determine if the patients met the inclusion or exclusion criteria.
Case definition (primary outcome)
Cases were patients with an infant with (I) PTB or (II) LBW. Preterm birth is defined as childbirth that takes place within 259 days of the mother’s last menstrual period (LMP) or 37 completed weeks of gestation, and LBW is an infant birth weight of less than 2,500 g.15 Controls included patients who had given birth to a live infant after 259 days since the mother’s LMP or after 37 completed weeks of gestation, and the infant’s birth weight was ≥2,500 g. Gestational age was determined in the 1st trimester through the obstetric criteria based on the date of LMP and/or ultrasound.16 The information regarding the patient’s name, case number, maternal age, socioeconomic status (SES) (modified Kuppuswamy scale),17 chronic hypertension status, diabetes, urinary tract infection (UTI), parity (number of times a female patient has given birth to a fetus with a gestational age of 24 weeks or more, regardless of whether the child was born alive or stillborn), smoking during pregnancy, drug and/or alcohol use during pregnancy, past gynecological history, as well as the infant’s birth weight and gestational age, was collected from the medical records of all the patients who had delivered a live infant. Chronic hypertension was defined as systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg, confirmed by multiple measurements, and detected before conception or 20 weeks of gestation.18
Intraoral examination – disease definition (secondary outcome)
The intraoral examination was conducted by 3 qualified examiners, with one appointed to each ward (KSV, NB and SS). Inter and intra-examiner calibration was done before the commencement of the study under the supervision of another researcher (NVB). The examiners were unaware of the patient’s medical status, and the infant’s birth weight and gestational age. The intraoral examination included recording the plaque index (PI) (Silness and Löe), the gingival index (GI) (Löe and Silness), the pocket probing depth (PPD), and clinical attachment loss (CAL) around all present teeth, excluding third molars. The PPD and CAL were measured at 6 sites of the tooth (midbuccal, buccomesial, buccodistal, midlingual, mesiolingual, and distolingual). The patients were classified as having CP according to the Centers for Disease Control and Prevention and the American Academy of Periodontology (CDC-AAP) definition of periodontitis: no periodontitis – no evidence of mild, moderate or severe periodontitis; mild periodontitis – ≥2 interproximal sites with CAL ≥ 3 mm (not at the same tooth) and ≥2 interproximal sites with PPD ≥ 4 mm (not at the same tooth), or 1 interproximal site with PPD ≥ 5 mm; moderate periodontitis – ≥2 interproximal sites with CAL ≥ 4 mm (not at the same tooth) or ≥2 interproximal sites with PPD ≥ 5 mm (not at the same tooth); and severe periodontitis – ≥2 interproximal sites with CAL ≥ 6 mm (not at the same tooth) and at least 1 interproximal site with PPD ≥ 5 mm.19, 20 On average, 20 patients were examined in each ward, using sterile instruments. The CP15 University of North Carolina probe (UNC-15) (Equinox Instruments Ltd, Lincoln, UK) was used to record GI, PPD and CAL. A data operator simultaneously entered the medical records and the intraoral examination data into a data sheet, matching the case numbers.
Exclusion criteria
Patients were excluded from the study if they had undergone in vitro fertilization, had had multiple gestations, spontaneous abortion in the current gestation, elective and/or induced preterm delivery because of maternal and/or fetal conditions, had any medical condition requiring antibiotic prophylaxis for dental treatment, gestational diabetes, human immunodeficiency virus (HIV) infection, UTI, heart disease, renal disease, hypertensive disorders of pregnancy occurring after 20 weeks of gestation, any dental treatment during the period of gestation, or did not consent to an intraoral examination.
Statistical analysis
After collecting the data, they were compiled, coded and entered into a Microsoft Excel 2019 spreadsheet. The descriptive analysis was presented as mean (M) and standard deviation (SD) or as proportions. The proportions between the groups were compared with the χ2 test. The data distribution was tested using the Kolmogorov–Smirnov test. Based on the normal distribution of the data, Student’s t test and the Mann–Whitney U test were applied to assess differences between the group means. A logistic regression analysis was performed, with PTB and LBW as dependent variables with regard to both the categorical (age, SES, hypertension, diabetes, UTI, previous PTB, PPD < 4 mm or PPD ≥ 4 mm, and CAL: no periodontitis or having periodontitis) and continuous data (PI and GI). A backward stepwise method was used to select independent variables, with an entry at p = 0.05 and a removal at p = 0.10. Adjusted odds ratios (AORs) with a 95% confidence interval (CI) for the risk of PTB and LBW were calculated. All analyses employed IBM SPSS Statistics for Windows, v. 22.0 (IBM Corp., Armonk, USA). A p-value less than 0.05 was considered statistically significant.
Results
There were 628 PTB cases and 279 LBW cases amongst 1,200 live births (Table 1 and Table 2, respectively, Figure 2). The prevalence of PTB was 52.3%, and for LBW it was 23.3%. There were 258 cases which were both PTB and LBW (Table 1). The mean patient age was 25.09 ±3.19 years. A total of 618 patients had a previous history of PTB – 46.0% in the PTB group and 18.0% in the LBW group (Table 1 and Table 2, respectively). The average gestational age was 36.64 ±1.47 weeks (37.75 ±0.54 weeks in the control group and 35.64 ±1.32 weeks in PTB case group) (Table 1). The average infant birth weight was 2,715.07 ±366.06 g, with 2,860.80 ±263.33 g for controls and 2,234.01 ±214.11 g for LBW cases (Table 2).
Table 3 and Table 4 describe the periodontal status of patients in the PTB and LBW groups, respectively. The difference in PI was highly significant, with the score being higher for the PTB (p < 0.001) and LBW (p < 0.001) groups as compared to controls. The same trend was observed for the GI scores. The mean PPD was 4.79 ±1.28 mm in the PTB group and 4.54 ±1.06 mm in the LBW group, with both values being significantly different when compared with controls (p < 0.001). The prevalence of CP was 53.2% in the sample, with 423 cases among the 628 PTB patients and 251 cases among the 279 LBW patients. When compared, the difference between controls and cases was highly significant (p < 0.001).The periodontal parameters for the control and case groups according to gestational age and the infant birth weight are graphically presented in Figure 3, Figure 4 and Figure 5, Figure 6, respectively.
Table 5 and Table 6 show the results of the logistic regression analysis with regard to risk factors and PTB and LBW, respectively. After the stepwise elimination of insignificant predictors, the factors which had a significant effect on PTB were as follows: a previous history of PTB (AOR = 0.59; p < 0.001; 95% CI: 0.46–0.76); hypertension (AOR = 0.63; p = 0.050; 95% CI: 0.39–1.02); UTI (yes) (AOR = 0.46; p < 0.001; 95% CI: 0.32–0.66); PI (AOR = 1.61; p < 0.001; 95% CI: 1.26–2.07); and PPD (≥4 mm) (AOR = 4.32; p < 0.001; 95% CI: 3.09–6.02) (Table 5). After the stepwise elimination of insignificant predictors, the factors with a significant effect on LBW were as follows: age of 26–30 years (AOR = 0.55; p = 0.004; 95% CI: 0.36–0.83); a previous history of PTB (AOR = 0.68; p = 0.050; 95% CI: 0.47–1.00); UTI (yes) (AOR = 0.37; p < 0.001; 95% CI: 0.21–0.65); PI (AOR = 2.02; p < 0.001; 95% CI: 1.43–2.83); and PPD (≥4 mm) (AOR = 8.70; p < 0.001; 95% CI: 6.01–12.59) (Table 6).
Discussion
The purpose of the present study was to find an association between CP and PTB and LBW in pregnant females admitted to the ObGy Department of the Civil Hospital, Ahmedabad, India. Preterm birth is a major cause of child mortality, and it is associated with emotional and economic burden.5 According to the national, regional and global estimates of the PTB rates in 2010, with time trends since 1990 for selected countries,21 India is among the 10 countries of the world with the highest number of the estimated PTB cases, which accounts for 60% of all PTBs globally. There are 3.6 million PTBs in India annually, 303,600 babies do not survive, and most deaths are due to prematurity.22 According to the results of another hospital-based case–control study conducted in Ahmedabad, India, there was a 30% prevalence of LBW, and 644 out of 1,317 LBW babies were preterm born.23 In a community-based study designed to identify possible risk factors for PTB in selected districts of Gujarat, India, the proportion of preterm babies out of a total of 2,009 deliveries was 8.9%.24 The prevalence of PTB (52.3%) and LBW (23.3%) was found to be high in our sample. Despite excluding the confounding factors for PTB and LBW, the high prevalence warrants more in-depth research to find other factors affecting gestation time and the birth weight.
The demographic data of the present study shows that the majority of the included patients belonged to SES III and IV. The modified Kuppuswamy scale is commonly used to measure SES in urban and peri-urban communities, and is based on the educational level, occupation and monthly income of the head of the family.17 The 2017 update of the scale was used for this sample, as the data collection period was between April 2017 and December 2017. According to this scale, SES III and IV refer to the middle and upper lower classes. Of the 628 PTB patients, 90.13% were from SES III (253; 40.29%) and IV (313; 49.84%), and of the 279 LBW participants, 93.55% were from SES III (91; 32.62%) and IV (170; 60.93%). The Civil Hospital in Ahmedabad is a government multispecialty hospital that provides free treatment to patients below the poverty line and offers affordable treatment charges for patients from all SES classes, which can explain the higher number of patients from SES III and IV. Adverse socioeconomic factors are associated with an increased risk of PTB11, 25 and LBW.26 For the present sample, the logistic regression analysis assessing risk factors for PTB showed high ORs for SES III (OR = 4.23; 95% CI: 0.67–26.93) and SES IV (OR = 4.97; 95% CI: 0.78–31.62), though the result was not significant. Moreover, SES as a risk factor did not affect PTB or LBW in this sample, perhaps due to the public health measures taken by the government to improve female reproductive health. The initiated integrated programs have made medical care accessible to females, especially those with a low SES,27, 28 which has helped considerably to reduce maternal malnutrition and improved public awareness in recent years. When considering the results for SES II, it was found to affect PTB (OR = 6.57; p = 0.050; 95% CI: 0.99–43.49). Since the sample size in SES II was 100 and included 56 PTB patients, and the difference was significant, it warrants further research with regard to SES II affecting PTB.
Another factor that was found to affect the incidence of PTB and LBW was maternal age. The incidence increases in the extremes of female reproductive life, i.e., less than 18 and more than 36 years of age.11 In the present sample, more patients were aged less than 30 years, which can be attributed to the social and cultural practices followed by the rural and semi-urban population residing in the areas around Ahmedabad. The patients in the 26–30 age group were less likely to have a baby with LBW (AOR = 0.55; p = 0.004; 95% CI: 0.36–0.83) as compared to other age groups.
Out of 1,200 patients, 618 had a history of PTB, with 284 in the PTB group and 111 in the LBW group. The patients with a history of PTB had a reduced chance of having PTB (AOR = 0.59; p < 0.001; 95% CI: 0.46–0.76) and LBW (AOR = 0.68; p = 0.050; 95% CI: 0.47–1.00). However, other studies found previous PTB to be a significant risk factor for PTB and LBW,16, 29, 30 since they obtained higher ORs than the current study. According to Meis et al., previous PTB is a significant predictor of PTB.31 There were 258 (41.08%) cases of LBW in the PTB group. The composite term PTLBW is no longer used in the obstetrics literature, as it may incorporate diversified underlying etiologies.32 Therefore, this factor was not included in the regression analysis.
Chronic hypertension significantly affects APOs, as confirmed by a meta-analysis of 55 studies that included 795,221 pregnancies, spanning 4 decades.33 Urinary tract infection during pregnancy is a frequent finding and is an independent risk factor for APOs.34 During pregnancy, immunological changes help to promote tolerance to the fetus and protect the mother against infection. However, females are more susceptible to infection and the effects of the toxins produced by microorganisms.34 According to a study published in 2008, asymptomatic bacteriuria is one of the most common causes of preterm labor.35 A possible explanation for this finding could be that UTI may increase the release of inflammatory chemokines and cytokines, which can stimulate uterine contractions, cause the premature rupture of membranes and induce PTB.35 In the present sample, there were 88 patients with hypertension, though the presence of hypertension reduced the risk of PTB (AOR = 0.63; p = 0.050; 95% CI: 0.39–1.02). Furthermore, UTI reduced the risk of PTB (AOR = 0.46; p < 0.001; 95% CI: 0.32–0.66) and LBW (AOR = 0.37; p < 0.001; 95% CI: 0.21–0.65). These results warrant an in-depth study of the effects of these factors on pregnant females.
The overall prevalence of CP in the sample was 53.17% – 67.36% in the PTB group and 89.96% in the LBW group. The first clinical study on the association between APOs and the periodontal status in humans was a case–control study conducted by Offenbacher et al. in 1996.4 Since then, numerous studies have evaluated the association between maternal periodontal infection and APOs, and many systematic reviews and meta-analyses have also evaluated and discussed the link in detail.6, 15, 36, 37 In a study conducted in the same hospital, the prevalence of CP in patients aged between 19 and 35 years was 43%, and 41.1% had poor oral hygiene.14 These discrepancies can be explained by the definition of CP. The study by Gupta et al.14 used Russell’s periodontal index to categorize periodontitis, whereas the present study classified CP using the criteria described in the ‘Material and methods’ section, with only CAL used to define and classify CP severity.
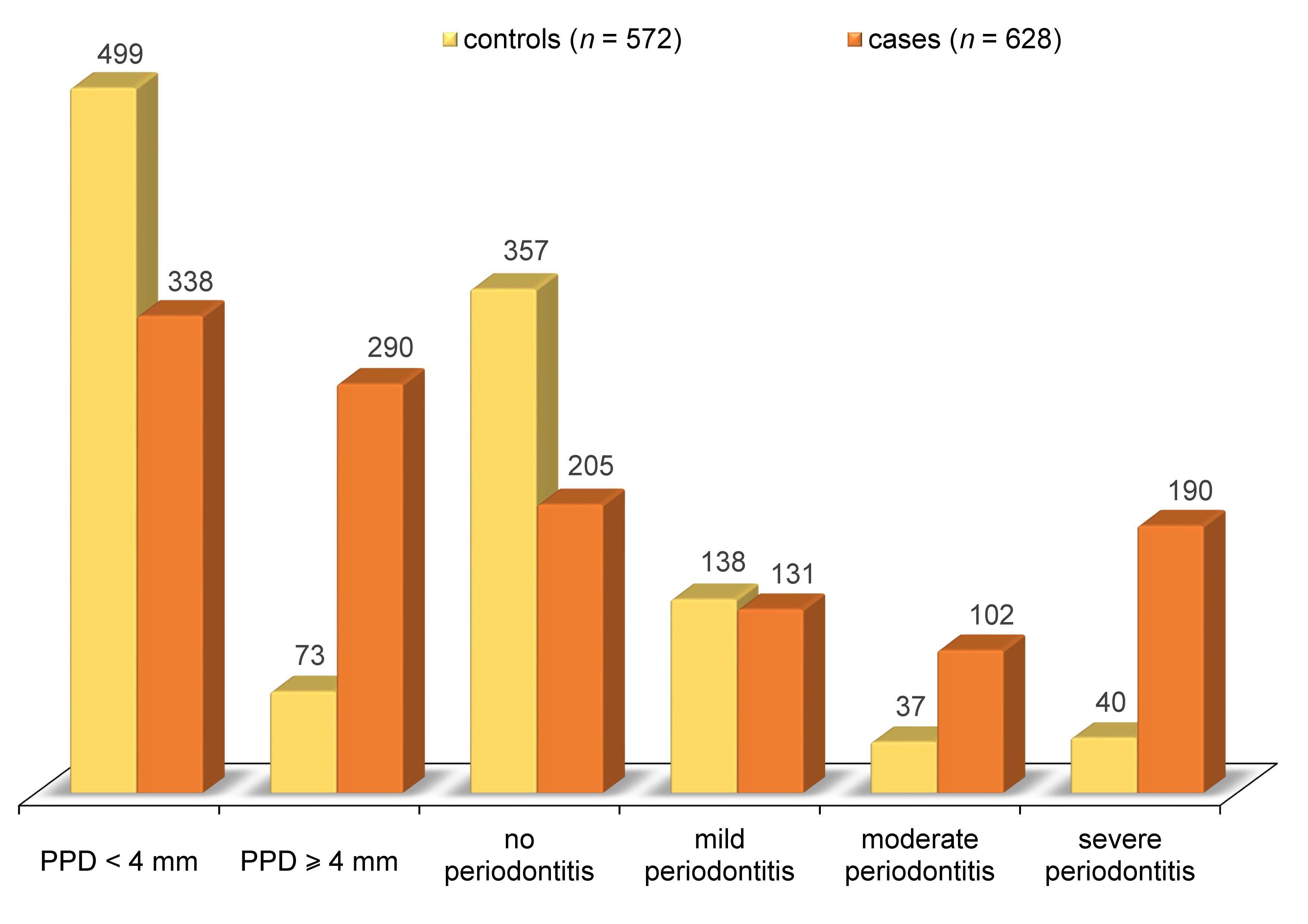
The differences in the PI and GI scores between the control and the PTB and LBW groups were highly significant, with higher scores among cases. The mean PPD in the PTB group (4.79 ±1.28 mm) was significantly higher than in controls. Of 363 cases, 290 had a mean PPD ≥4 mm. The mean PPD in the LBW group (4.54 ±1.06 mm) was significantly higher than in controls. Out of 363 cases, 202 had a mean PPD ≥4 mm. When CP severity was compared between controls and PTB and LBW cases, a higher number of PTB cases had moderate and severe CP, and more LBW cases had severe CP, with the differences being statistically significant.
Approximately 30–40% of preterm delivery cases are thought to be due to different infections.10 The possible mechanisms by which periodontal infection affect APOs include the translocation of periodontal pathogens to the feto-placental unit (metastatic infection),7 and the effects of inflammatory mediators, such as IL-1, IL-6, IL-8, TNF-α, and PGE2, on the feto-placental unit (metastatic inflammation).7, 38 According to a systematic review, patients with APOs had higher levels of inflammatory mediators in GCF.39 In addition, a cross-sectional study including 120 females (60 normal births and 60 PTBs) concluded that those with PTB demonstrated worse periodontal parameters and significantly increased GCF levels of IL-6 and PGE2 as compared to normal births.9 In the present study, inflammatory markers were not evaluated with regard to PTB, LBW and normal births.
The human placenta is known to have its own specific microbiome, yet many studies have also found evidence for the presence of periodontal pathogens, such as Porphyromonas gingivalis, in it.38, 40 Furthermore, there is a tendency toward pregnancy gingivitis during pregnancy, as gingival tissues are sensitive to hormonal changes and the slightest increase in plaque accumulation can cause an exaggerated response. However, gingivitis during pregnancy is not clinically or histologically different from gingivitis in non-pregnant persons. González-Jaranay et al. found an increase in the PI (O’Leary) and GI (Ainamo and Bay) scores during pregnancy in females who reached a full term, as well as a slight increase after delivery.41 Radnai et al. also demonstrated higher mean PI scores in the study group (0.79) than in the control group (0.67), though the difference was not significant (p = 0.141).42
For the present study, PPD ≥ 4 mm was considered one of the parameters of a gingival response to plaque accumulation. According to Lindhe et al., the optimal response to periodontal surgery was observed in pockets deeper than 4 mm; also during the maintenance phase, high plaque scores were noticed in patients with residual pockets greater than 4 mm.43 Therefore, 4 mm was considered to be the critical PPD value. Patients with a mean PPD ≥4 mm had at least a few pockets deeper than 4 mm. This may have led to more plaque accumulation, which is a critical factor for eliciting a systemic inflammatory response. A reasonable biological model explaining the relationship between periodontitis and other diseases is that periodontitis causes inflammatory burden through bacteremia, which elicits a systemic inflammatory response or cross-reactivity, resulting in an autoimmune reaction. If the surface area of the pocket is calculated, a minimum area of 50 cm2 allows the penetration of bacterial products into host tissues.42 Hence, it can be interpreted as the larger the amount of the inflamed periodontal tissue (i.e., the deeper the periodontal pockets), the greater the chance of periodontitis eliciting a systemic response. As such, the periodontal inflamed surface area (PISA) may be considered the main contributor to any systemic inflammatory burden posed by periodontitis.44 In the present sample, the high PI scores in the PTB (AOR = 1.61; p < 0.001; 95% CI: 1.26–2.07) and LBW (AOR = 2.02; p < 0.001; 95% CI: 1.43–2.83) groups, as well as PPD ≥ 4 mm in the PTB (AOR = 4.32; p < 0.001; 95% CI: 3.09–6.02) and LBW (AOR = 8.70; p < 0.001; 95% CI: 6.01–12.59) groups, significantly increased the risk of PTB and LBW, and were significant predictors of PTB and LBW after the stepwise elimination of insignificant predictors.
In the current sample, the presence of CP significantly increased the risk of PTB (OR = 4.23; p < 0.001; 95% CI: 2.99–5.98) and LBW (OR = 7.84; p < 0.001; 95% CI: 5.33–11.53), though it was eliminated as an independent risk factor after adjustment. An explanation for this observation is that CAL may not be the most appropriate clinical assessment measure when the goal is to assess periodontitis as a cause of the systemic inflammatory responses associated with systemic diseases or conditions.45 Indeed, CAL results from the chronic inflammatory infection and host response caused by the plaque microorganisms harbored in deep pockets. Hence, the observations of this sample divert attention toward the systemic effects of a local inflammatory response instead of the disease as a singular entity.
López et al. found a significant association between PD and PTB (RR (risk ratio) = 3.5; p = 0.006; 95% CI: 1.30–9.10), and PD to be the only risk factor for LBW (RR = 3.5; p = 0.028; 95% CI: 1.06–11.4).46 Radnai et al. studied the association between early periodontitis and PTB, and found that patients with periodontitis had a 5.46 times greater chance of preterm delivery or LBW than periodontally healthy females.42 Siqueira et al. showed a risk association between CP and PTB, LBW and intrauterine growth restriction (IUGR).16 Khader et al. assessed the association between PD severity and PTB and LBW among females in Northern Jordan, and found that the ORs associated with a 1-millimeter increase in the mean PPD and CAL were 2.04 (95% CI: 1.59–2.61) and 2.21 (95% CI: 1.66–3.00), respectively.47 Gesase et al. found that PD was significantly associated with LBW (AOR = 2.41; 95% CI: 1.34–4.33) and PTB (OR = 2.32; 95% CI: 1.33–4.27).48 On the other hand, many studies included in a recent systematic review and meta-analysis reported that periodontitis was not a risk factor for PTB or LBW.49 However, they concluded that PD significantly increased the risk of APOs.49 Nonetheless, large prospective, blinded cohort studies with standardized PD diagnostic criteria and the adequate control of the confounding factors are still required to confirm the relationship between PD and AOPs.
A systematic review and meta-analysis by Manrique-Corredor et al. showed that 60% of the assessed studies observed a positive association between maternal periodontitis and PTB.50 They also found heterogeneity in the definition of CP. Researchers have compared the different definitions used to diagnose CP, slightly underestimating the extent of the disease and obtaining higher ORs, though ORs decreased when the criteria became stricter. Clinical attachment loss, one of the parameters for classifying periodontitis severity and extent, is the measure of the total disease and not of the current disease activity.42 Given that the present study found a high PI score and a mean PPD ≥4 mm to be independent risk factors, even a shallow pocket is a source of microorganisms and would account for the total inflammatory burden.44 However, it can be evaluated further by conducting microbiological investigations and mapping the levels of inflammatory mediators in future studies, this being a limitation of the present study.
Conclusions
The present study found that a high PI score and a mean PPD ≥4 mm significantly increased the risk of PTB and LBW. Even though the prevalence of PTB/LBW is higher in the extremes of reproductive age, the present study found a high prevalence of PTB/LBW in the <36 age group. More efforts can be made to study the association between CP (CAL) severity and PTB and LBW in a larger sample.
Ethics approval and consent to participate
The study was approved by the Institutional Ethics Committee at the Government Dental College and Hospital, Civil Hospital in Ahmedabad (No. IECGDCH/S.10/2017 dated 18/3/2017), the Head of the ObGy Department and the Medical Superintendent of the Civil Hospital. The informed written consent was obtained from all participants.
Data availability
All data generated and/or analyzed during this study is included in this published article.
Consent for publication
Not applicable.