Abstract
Background. The outbreak of the coronavirus disease 2019 (COVID-19) pandemic was associated with the provision of multiple guidelines for the dental profession. All elective procedures were restricted, and only emergency procedures were performed. There was fear and anxiety among dentists while performing aerosol-generating procedures (AGPs), as they were considered to pose a high risk of COVID-19 transmission.
Objectives. The aim of this study was to assess the risk of infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) during AGPs, and to examine the association between risk severity and the number of AGPs performed per day. The efficacy of personal protective equipment (PPE) was also assessed.
Material and methods. This cross-sectional cohort study was based on an online questionnaire form completed by 629 general and specialized dentists between January 1 and February 28, 2021. The collected data referred to the sources of COVID-19 infection, the type of PPE used and the number of AGPs performed each day by dental healthcare professionals (DHCPs). For each question, the absolute numbers of responses as well as percentages were calculated.
Results. Among the 629 DHCPs, 113 (17.97%) contracted COVID-19. The risk of contracting COVID-19 during AGPs was the same as in the case of non-AGPs, and the infection risk was not associated with the number of AGPs performed per day. The efficacy of a surgical mask with a face shield/eye goggles was higher in comparison with all other types of PPE. Differences in the infection risk across the different types of PPE used were statistically significant (p < 0.001).
Conclusions. The risk of COVID-19 transmission during AGPs is the same as in the case of non-AGPs. Thus, restrictions on the performance of elective AGPs should be lifted. On the other hand, the best protection during AGPs is provided by a surgical mask with a face shield/eye goggles.
Keywords: personal protective equipment, aerosol-generating procedures, COVID-19 transmission, dental healthcare professionals
Introduction
Coronavirus disease 2019 (COVID-19) was declared a pandemic by the World Health Organization (WHO) on March 11, 2020.1 This disease is caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2).2 It mainly affects the respiratory system, with symptoms varying from mild flu to severe pneumonia, which can ultimately lead to respiratory collapse.2 Other symptoms include the loss of taste and smell, headache, diarrhea, a sore throat, shortness of breath, and myalgia.2 As far as oral manifestations of COVID-19 are concerned, xerostomia seems to be the most prevalent, followed by oral and dental pain, ulcerations, pain in the jaw bones and joints, and halitosis. Some individuals experience 2 or more oral symptoms at one time.2 Global efforts were made to formulate a vaccine that would combat the virus, and prevent and contain the spread of COVID-19.3 Although vaccines are one of the most successful interventions to fight viral infections, they may be associated with some adverse effects.3 These include fatigue, redness at the injection site, limb pain, malaise, headache, muscle and joint pain, fever, and chills.3 As far as facial and oral manifestations are concerned, there is no significant association with COVID-19 vaccination.4
The SARS-CoV-2 virus underwent numerous mutations over time, resulting in various strains, such as Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), Delta (B.1.617.2), and Omicron (B.1.1.529).5 Further studies are needed to establish transmissibility, symptoms and treatment for the Omicron variant.6 The efficacy of vaccines is being studied, with lesser efficacy found against the Beta and Delta variants. Booster doses are being recommended to improve the protective efficacy of vaccines against Omicron and other variants. A number of treatment options are available for COVID-19, including plasma therapy, and antiviral therapy using remdesivir, hydroxychloroquine (with or without azithromycin) and lopinavir-ritonavir. Additional therapeutics include anti-fibrotics, anti-inflammatory cytokines, such as interleukin-6 receptor antagonists and complement antagonists, anti-infectives, non-steroidal anti-inflammatory drugs (NSAIDS), systemic corticosteroids, bronchodilators, and vasodilators.7 It has been demonstrated that azithromycin, a macrolide, provides antiviral and immunomodulatory effects in patients infected with SARS-CoV-2.8
The Centers for Disease Control and Prevention (CDC) has reported respiratory droplets, aerosols and close contact (less than 1 m) as major modes of transmission.9 A droplet can be transmitted by coughing, sneezing, speaking, singing, and via contact with the mucous membranes, especially of the nose, the eyes or the mouth. Droplets >5–10 µm in diameter or fomites in the immediate environment of the infected person can carry the virus.10, 11 Airborne transmission occurs through droplets <5 µm in diameter, which develop from the evaporation of larger droplets. They remain in the air for a longer period and can travel a distance of more than 1 m.12 Procedures that produce aerosols can also lead to airborne transmission.13 Aerosols refer to small particles (<5–10 µm in diameter) that are capable of travelling longer distances, and thus can be easily inhaled. However, larger droplets (>20 µm in diameter) fall under the influence of gravity and are too large to be inhaled. Intermediate droplets (10–20 µm in diameter) may either remain suspended in the air or settle down.14, 15, 16 As a result, most dental procedures generating aerosols pose a risk of transmitting COVID-19.17 Dental procedures that generate aerosols include ultrasonic scaling, tooth polishing, air polishing, air abrasion, the use of slow- and high-speed rotary instrumentation, the use of an air-water triple syringe,18 and intraoral radiographs.19 Furthermore, saliva contains high levels of SARS-CoV-2, which peak in the first week of infection and can easily contribute to the spread of the disease.10 At the beginning of the outbreak, there was no confirmed information on the transmission routes for SARS-CoV-2, and many healthcare workers were concerned about infecting their families and themselves.20 This created severe psychological stress, which indirectly affected the quality of treatment provided.20
More research is needed, however, to confirm the transmission routes for SARS-CoV-2 and to measure the risk of COVID-19 infection among dental healthcare professionals (DHCPs) who perform aerosol-generating procedures (AGPs). Therefore, the current study was conducted to establish whether AGPs increase the risk of SARS-CoV-2 transmission as well as to evaluate the efficacy of personal protective equipment (PPE) in order to alleviate the concerns and anxiety of DHCPs.
Material and methods
This cross-sectional cohort study was carried out between January 1 and February 28, 2021. The study was conducted using an online questionnaire form that was sent to DHCPs via electronic mail. The targeted DHCPs included general and specialized dentists working at 12 dental colleges and hospitals located in different provinces of Pakistan. Different regions of the country were sampled, as the number of people infected with COVID-19 varied across the provinces. The e-mail addresses of DHCPs were obtained from the human resources departments of dental colleges and hospitals. An invitation to participate in the study, along with a link to the questionnaire, was e-mailed to 1,000 DHCPs. Those who consented to participate were included in the study, resulting in 629 respondents in total. A total of 371 DHCPs did not respond to the initial e-mail. Ethics approval for the study was granted by the institutional Research and Ethics Committee at the Rashid Latif Medical Complex, Lahore, Pakistan (No. of approval: RLDC/006080/20). Table 1 shows the questionnaire, which was validated by conducting a pilot study, where 52 DHCPs at our institution answered the questions; the collected data was analyzed, and its internal consistency was evaluated by using Cronbach’s alpha, which was 0.85.
After the validation of the questionnaire, the data was collected. Data analysis was performed using Microsoft Excel® 2021 for Mac, v. 16.56 (Microsoft Corporation, Redmond, USA), and the statistical software package Stata 14 (StataCorp, College Station, USA). For each question, the absolute numbers of responses as well as percentages were calculated. The analysis of variance (ANOVA) tests were used to determine the efficacy of various types of PPE, and to assess the relationship between the number of AGPs performed per day and the risk of contracting COVID-19. The significance level was set at p < 0.05.
Results
The number of DHCPs who contracted COVID-19 (n = 113) accounted for 17.97% of the 629 participants. Among the 113 DHCPs who contracted COVID-19, 51 (45.13%) were male and 62 (54.87%) were female. The mean age of the participants was 43 ±9.63 years. The number of AGPs performed in a day by all DHCPs as well as the calculation of the infection risk are presented in Table 2.
The ANOVA tests showed no association between the number of AGPs performed per day and the risk of contracting COVID-19 (p > 0.05).
A total of 39 (6.20%) of the 629 DHCPs indicated that they acquired COVID-19 through AGPs, 37 (5.88%) through non-AGPs, and 37 (5.88%) did not know the origin of the infection (i.e., were unsure). Figure 1 illustrates the percentage of DHCPs who contracted COVID-19, together with the source of the infection.
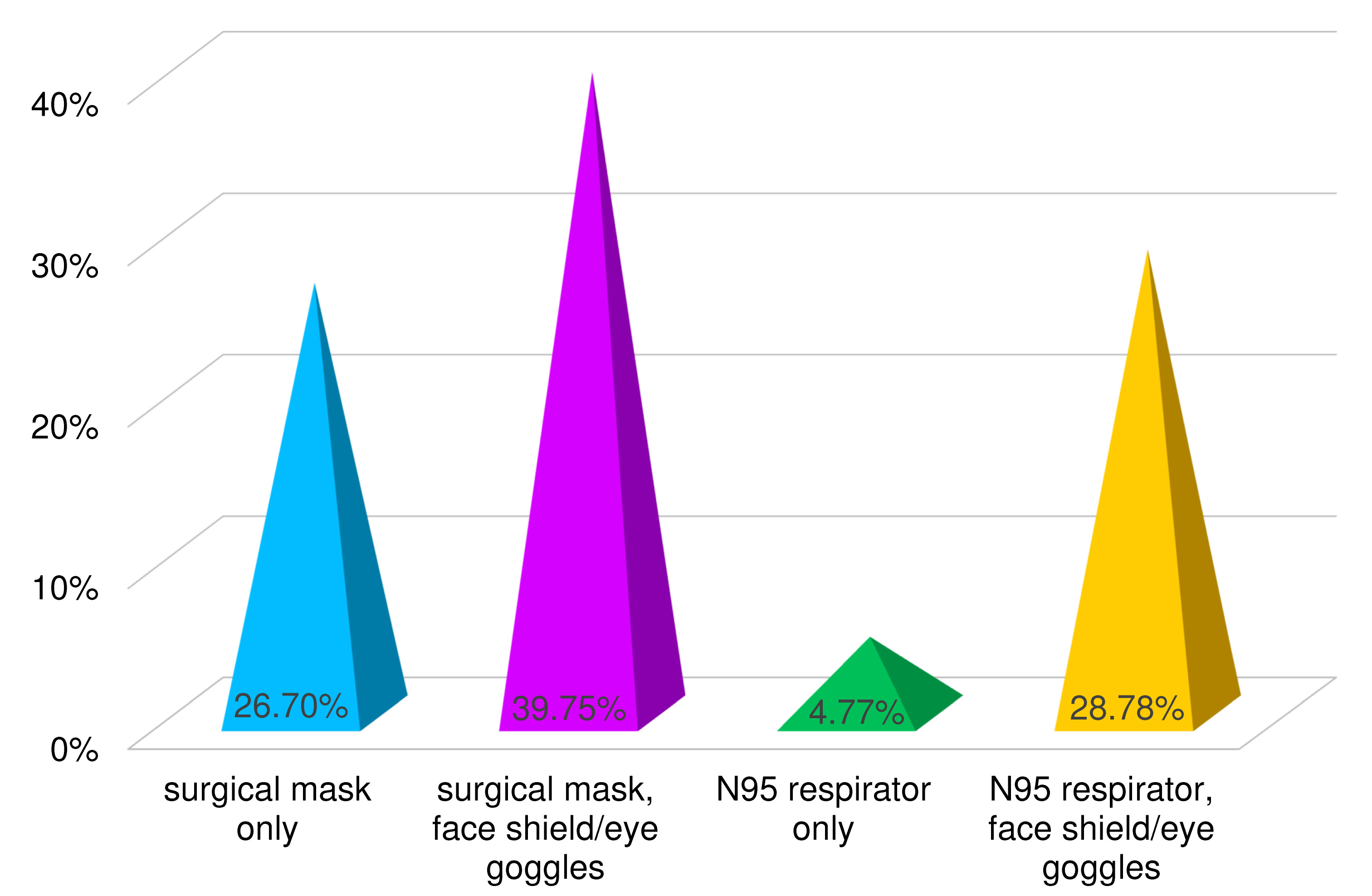
According to the obtained data, the PPE used by 39.75% of DHCPs included a surgical mask with a face shield/eye goggles, while 28.78% of DHCPs used an N95 respirator with a face shield/eye goggles. However, 26.70% and 4.77% of DHCPs used surgical masks and N95 respirators, respectively, without a protective face shield/eyewear (Figure 2).
Figure 3 shows the comparison of the different types of PPE used by the DHCPs who contracted and did not contract COVID-19. The ANOVA test showed significant differences between the types of PPE used with regard to the infection risk (p < 0.001). The DHCPs who wore surgical masks with face shields and eye goggles while performing dental procedures had maximum protection, as out of the 250 individuals who used them, only 25 developed COVID-19 (RR (relative risk) = 0.11). Using a surgical mask alone presented an RR of 0.18, using an N95 respirator with a face shield/eye goggles had an RR of 0.25, and using an N95 respirator alone had an RR of 5.00.
Discussion
The Occupational Safety and Health Administration has declared that all AGPs pose a very high risk of COVID-19 transmission from patients with known or suspected infection.1, 21, 22 However, the literature still lacks data on the estimation of the risk of COVID-19 spread among dentists and other healthcare professionals (HCPs) with regard to AGPs. Therefore, the aim of this study was to determine the transmission pattern for SARS-CoV-2 through AGPs and non-AGPs among DHCPs. The results of the current study reveal that 113 (17.97%) out of 629 DHCPs contracted COVID-19. Among the 113 DHCPs who contracted COVID-19, 39 (6.20%) reported that they had got infected through AGPs, whereas 37 (5.88%) related the contraction of the disease to non-AGPs, and the remaining 37 (5.88%) were unsure about the source of the infection. Given these results, it can be ascertained that AGPs pose no additional threat to DHCPs as compared to non-AGPs. The results of this study concur with Harding et al.’s review, which states that AGPs do not pose a greater threat of SARS-CoV-2 infection.23 Wong et al. also reported that in a Hong Kong hospital, 71 HCPs and 49 patients who had come into contact with a SARS-CoV-2-infected patient prior to testing were negative for COVID-19.24
The results of the current study also show that the transmission of COVID-19 is not associated with the number of AGPs performed per day, as 61.95% of DHCPs who developed COVID-19 were those who performed 1–3 AGPs in a day. There was a lower number of DHCPs who got infected after performing 4–5, 6–7 or >7 AGPs in a day. In the literature, there is no evidence linking the number of AGPs performed per day with the risk of contracting COVID-19 among DHCPs.
The efficacy of the PPE used by DHCPs was also assessed in the current study. All DHCPs used different types of PPE, depending upon their availability or affordability. The most interesting finding in this study was that, although all face masks prevent the transmission of airborne infections like COVID-19, surgical masks with face shields and eye goggles provided the greatest protection against COVID-19 infection during dental procedures, with an RR of 0.11.
A surgical mask used alone had an RR of 0.18, which was also found to be more efficacious as compared to an N95 respirator with a face shield and eye goggles (RR = 0.25) and an N95 respirator used alone (RR = 5.00). There is no evidence in the literature that coincides with the results of our study and shows a greater efficacy of surgical masks over N95 respirators. However, Johnson et al.25 and Loeb et al.26 reported an equal ability of surgical masks and N95 respirators to filter out the influenza virus. Likewise, the latest randomized controlled trial published by Radonovich et al. also demonstrates that there is no significant difference in the efficacy between surgical masks and N95 respirators.27 Offeddu et al.28 and Sommerstein et al.29 also reported similar results. Therefore, based on the findings of the current study, we advocate the use of surgical masks with face shields or eye goggles during AGPs, since they are cost-effective, convenient, easily obtainable, and safe for the user.
When using N95 masks, individuals may experience increased blood pressure, breathing resistance and heart rate, and diminished exercise performance.30 These masks are not recommended for people with severe pulmonary or cardiac disease, uncontrolled hypertension, or claustrophobia.30
Thus, this study helps to fill the knowledge gaps regarding the transmission routes for SARS-CoV-2, risk to DHCPs and the safety of AGPs. This void in the literature has created fear and uncertainty among DHCPs, which affected their ability to provide dental care when needed.
Conclusions
The illusion that AGPs are high-risk procedures during the COVID-19 pandemic can be set aside to some extent, as this study shows that the chances of contracting COVID-19 during AGPs are the same as in the case of non-AGPs, and that risk severity is not associated with the number of AGPs performed per day. While performing AGPs, a surgical mask with a face shield/eye goggles is the most efficacious PPE against SARS-CoV-2. However, it must be noted that this study used only subjective methods. More definitive conclusions can be drawn through objective methods. Nonetheless, this study will help to implement useful clinical interventions, prevent the wastage of PPE and other resources, and shift the focus to the quality of patient care. In light of these findings, we propose extending dental healthcare services to elective AGPs during the COVID-19 pandemic.
Ethics approval and consent to participate
The study was approved by the institutional Research and Ethics Committee at the Dental College of the Rashid Latif Medical Complex, Lahore, Pakistan (No. of approval: RLDC/006080/20). Written informed consent was obtained from all participants.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
ORCID iDs