Abstract
Background. The sweet taste and bitter taste genes are thought to have an influence on obesity and caries, which are chronic diseases.
Objectives. The aim of the study was to investigate the effects of the polymorphisms of TAS2R38 (the bitter taste gene) and TAS1R2 (the sweet taste gene), which are the most important members of the taste gene family, on the dental status of obese and normal-weight children.
Material and methods. The study included 78 healthy children and 100 children diagnosed with obesity (5–16 years old). The anthropometric measurements and dental status of the children were evaluated. The decayed, missing and filled permanent/primary teeth (DMFT/dmft) index was determined using the standard methods recommended by the World Health Organization (WHO). Blood samples were collected from all subjects and were analyzed via the polymerase chain reaction (PCR) test, with the use of specific primers for the genetic analysis. Five single-nucleotide polymorphisms (SNPs) of the TAS2R38 and TAS1R2 genes were investigated. The truncated Poisson and truncated negative binomial modeling approaches were used with regard to the data.
Results. The DMFT/dmft scores were low in obese children and high in children who did not sense the bitter taste (non-tasters). While obese non-taster children had increased DMFT/dmft scores, normal-weight non-taster children had decreased DMFT/dmft scores.
Conclusions. The alanine, valine and isoleucine (AVI) as well as proline, alanine and valine (PAV) haplotypes of the TAS2R38 gene are associated with the DMFT/dmft index and obesity. This study showed that the DMFT/dmft scores were decreased in obese children. According to the haplotype analysis of the TAS2R38 gene, the DMFT/dmft scores were increased in non-tasters. When differentiating obese non-tasters and control non-tasters, DMFT/dmft increased in obese non-taster patients, while it decreased in control non-taster patients.
Keywords: genetic, childhood obesity, tooth decay, oral health, TAS2R38 polymorphism
Introduction
Caries and obesity are multifactorial diseases having a genetic, epigenetic and dietetic background.1 Like tooth decay, obesity has become an almost global epidemic among children.2 Consuming food with a high carbohydrate (CH) content is closely associated with obesity. Therefore, the CH-weighted eating habits represent a common problem related to tooth decay and obesity.3 There is an apparent correlation between caries and CH consumption as a severe risk factor for obesity.4
Carbohydrate consumption, which actively contributes to caries and obesity, may be affected by the genetic code determining our taste perception.5 The sense of taste helps humans predict whether the food they consume is beneficial or harmful. The taste has developed as a guide to identify the nutrients needed by the body.6 Humans can be categorized into 2 groups with regard to their reactions to the bitter taste – tasters and non-tasters. The most critical component responsible for the bitter taste is phenylthiocarbamide (PTC).7 Individuals sensitive to PTC are also susceptible to more than 10,000 other tastes, which is not observed in individuals who are not sensitive to PTC.8 The primary gene responsible for PTC sensitivity is TAS2R38, located on chromosome 7.9 The polymorphisms of the TAS2R38 bitter taste gene may lead to differences in how the taste of food is sensed. Therefore, any polymorphism of this gene may affect nutritional habits, which play significant roles in the development of tooth decay and obesity.10 Studies are being carried out to discover the effect of TAS2R38 on the body mass index (BMI).11 In a recent study, it was shown that the daily energy intake of the ‘non-taster’ group was higher in pre-adolescents as compared to the ‘taster’ group, which enjoys the PTC/6-n-propylthiouracil (PROP) taste.12 It indicates that TAS2R38 can be associated with increased BMI and obesity risk in children.13 Although the TAS2R38 polymorphisms have been studied in different populations, there is a lack of data with regard to the Turkish population.
Tooth decay, which is caused by many factors, is one of the most common chronic diseases of childhood. Tooth decay occurs as a result of the complex interaction of many environmental and genetic factors.14 The relationship between TAS2R38, obesity and caries has been stated in the literature.15 Studies on TAS2R38 show that low taste sensitivity is associated with a greater risk of caries as compared to high taste sensitivity, which suggests that TAS2R38 may be associated with caries.16 The TAS1R and TAS2R gene families encoding taste receptors are involved in the molecular mechanism of taste perception. The TAS1R gene family includes the genes encoding receptors that allow the perception of sweet taste; it comprises 3 taste receptor genes on chromosome 1 – TAS1R1, TAS1R2 and TAS1R3.17 The perception of the sweet taste is mediated by the heterodimeric G protein-coupled receptors encoded by TAS1R2 and TAS1R3.17 A significant relationship between TAS1R2 and caries was observed in a recent study.18 Yet another study, conducted on twins, showed that genetic differences between individuals influenced taste perception and nutritional habits.19 However, the research on the topic is still scarce in the literature.
The aim of the present study was to investigate the effects of obesity and the polymorphisms of the TAS2R38 and TAS1R2 genes, the major members of the taste gene family, on tooth decay in children through evaluating the caries levels in obese and non-taster children. To this end, 2 hypotheses were tested:
– hypothesis I: There is no difference in the incidence of tooth decay between children with obesity and those of normal weight; and
– hypothesis II: There is no difference in the incidence of tooth decay based on the occurence of the TAS2R38 bitter taste and TAS1R2 sweet taste gene polymorphisms.
Material and methods
This cross-sectional, observational study was approved by the Ethics Committee of the Health Sciences Institute at Atatürk University, Erzurum, Turkey (No. B.30.2.ATA.0A10000-617), and was supported by the Scientific Research Projects Commission at Atatürk University (project No. 2012/66 and 2012/375). The study was carried out in collaboration with the Department of Pediatric Endocrinology and the Department of Medical Genetics of the Faculty of Medicine, and the Department of Pediatric Dentistry of the Faculty of Dentistry at Atatürk University. All participants and their parents were informed about the study aims and procedures before any interventions were made, and written consent was obtained from all parents to confirm their approval for treatment. A patient follow-up form was completed for each participant, and the oral and general health status, weight and height measurements, regular medication use, previous dental treatment, and the eating habits over the previous 3 days were recorded. A total of 100 patients aged 5–16 years who had been diagnosed with obesity after referral to the Department of Pediatric Endocrinology were transferred to the pedodontist liable for the assessment of their oral care (MK). The blood samples (2 mL) obtained from the patients as part of routine examinations were collected into ethylenediaminetetraacetic acid (EDTA)-containing tubes and transferred to the Department of Medical Genetics for the genetic analysis. The control group comprised 78 healthy children aged 6–16 years who had been referred to the Department of Pediatric Dentistry and had no systemic disorders. The same procedures were followed for the control group.
Weight measurements were performed using an electronic scale with a ±100 g sensitivity range when the participants were wearing lightweight clothes. Each participant stood on the scale with both feet placed at the center of the platform and the value presented on the electronic screen was recorded in kg.
A steel tape measure was used to determine the height of the children while standing upright with their bare feet parallel and adjacent to each other, and with their shoulders and hips touching the wall. Height measurements were recorded in cm. The growth curves described for Turkish children were used to assess BMI,20 and the participants with BMI corresponding to the 95th percentile or above of age-specific limits were considered obese. The decayed, missing and filled teeth of the participants were identified, and the data was recorded for permanent and primary teeth based on the DMFT/dmft scale, respectively.
DNA isolation and SNP genotyping
Whole blood samples were taken from the children for DNA isolation. The blood samples were added by means of venipuncture into Vacutainer® EDTA tubes (BD, Franklin Lakes, USA) and used for manual DNA isolation, utilizing the QIAamp® DNA Blood Mini Kit (Qiagen, Hilden, Germany) according to the manufacturer’s instructions. A single-nucleotide polymorphism (SNP) identification assay (LightSNiP; TIB Molbiol, Berlin, Germany) employing the simple-probe fluorescence melting curve analysis (FMCA) was used to detect the TAS2R38 and TAS1R2 polymorphisms. The Rotor-Gene Q (Qiagen) was used in the polymerase chain reaction (PCR) and high-resolution FMCA procedures. A 20-microliter mixture was prepared for each SNP; it included 1 µL of LightSNiP reagent mix (TIB Molbiol), 2 µL of LightCycler® FastStart DNA Master HybProbe (Roche Diagnostics, Mannheim, Germany), 1.6 µL of MgCl2 (25 mM), and a volume of 50 ng DNA and H2O. The PCR program included the initial denaturation at 95°C for 10 min, followed by 45 cycles of 10-second denaturation at 95°C, 10-second annealing at 60°C and elongation at 72°C for 15 s. The high-resolution FMCA program included cycles at 95°C for 30 s, at 40°C for 120 s and a ramp to 75°C at a transition rate of 1.5°C/s, with the continuous collection of fluorescence. The amplification and melting curves were generated using the Rotor-Gene Q software. As a result of the analysis, the allelic discrimination of the SNPs was achieved.
Statistical analysis
The obtained data was analyzed with the use of the IBM SPSS Statistics for Windows software, v. 21.0 (IBM Corp., Armonk, USA). Descriptive statistics were calculated for each variable and expressed as mean ± standard deviation (M ±SD). First, the Kolmogorov–Smirnov and Levene tests were applied to determine whether the data showed normal distribution and the homogeneity of variances. The χ2 test was used to evaluate gender distribution for children in the obese and control groups. The one-way analysis of variance (ANOVA) was used to evaluate differences with regard to age, DMFT/dmft and body mass index percentile (BMIP). The abovementioned software package was used to analyze the data, and the results were evaluated at an alpha level of 0.05 within a 95% confidence interval (CI). The Poisson and negative binomial models were applied to the data, using the R program (https://www.r-project.org). The DMFT/dmft score was defined as the dependent variable, and obesity and the absence of the bitter taste were defined as the independent variables. Caries was modeled with the obesity and non-taster dummy variables by using the truncated Poisson and truncated negative binomial modeling approaches.
The obesity and non-taster dummy variables were created to denote obesity. Obese and non-taster children were coded as 1, and normal-weight children (control) and tasters were coded as 0. Obese non-tasters and control non-tasters were included in the model and labeled as the obese_non-taster and control_non-taster dummy variables (obese non-tasters and control non-tasters were coded as 1, and obese tasters and control tasters were coded as 0). Considering that the highest number of decayed teeth would be 28 in the study, given the maximum age of 16 years in the study population, both models were truncated in the right truncate. The Wald test was used to assess whether the model coefficients were statistically different from zero.21
Results
There were no statistically significant differences in gender distribution (p = 0.881) or the mean age (p = 0.312 and p = 0.165 for boys and girls, respectively) between the obese and control groups. No statistical difference was found between the groups in terms of DMFT/dmft. The mean BMIP value was significantly higher in the obese group than in the control group (p < 0.001) (Table 1).
TAS1R2 genotypes
and the DMFT/dmft score
When the genotypes of rs4920566 SNP were evaluated, the highest DMFT/dmft score was found in the AG heterozygous control group. When the genotypes of rs9701796 SNP were evaluated, the highest DMFT/dmft value was found in the CC homozygous obese group. However, the difference between the genotypes were not statistically significant (Table 2).
TAS2R38 genotypes
and the DMFT/dmft score
When the genotypes of rs713598 SNP were evaluated, the highest DMFT/dmft score was found in the homozygous control group. However, the difference between the genotypes was not statistically significant. When the genotypes of rs1726866 SNP and rs10246939 SNP were evaluated, the highest DMFT/dmft scores were observed in the homozygous control group, but the differences between the genotypes were not statistically significant (Table 3).
TAS2R38 haplotypes
and the DMFT/dmft score
When the TAS2R38 haplotypes were evaluated, no statistical differences were found between the control and obese groups. The highest DMFT/dmft score was found in the CC homozygous genotype in all 3 SNPs of the TAS2R38 gene (Table 3).
Haplotype frequency
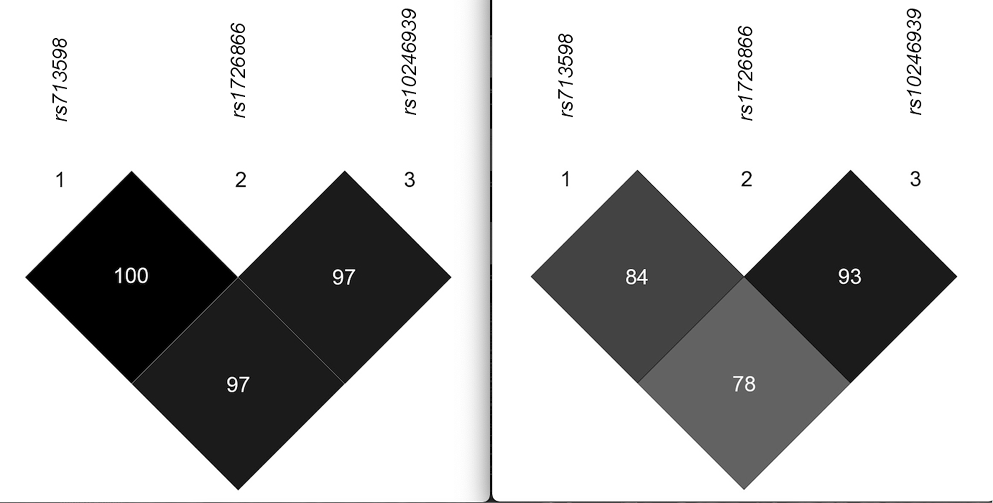
A total of 3 different SNPs of the TAS2R38 gene were evaluated and the linkage disequilibrium (LD) test was performed (Figure 1) to determine the haplotypes of the respondent children (Table 4). Partial tasters were included in the taster group.
Obesity, non-taster and the DMFT/dmft score
Among the studied SNPs, the rs713598 (C-G), rs1726866 (C-T) and rs10246939 (C-T) base changes were taken into consideration.13, 21 Children with the haplotype containing a combination of proline, alanine and valine (PAV) constituted the group highly sensitive to the bitter taste. In contrast, children with the haplotype containing the combination of alanine, valine and isoleucine (AVI) constituted the group with the inability to sense bitterness. Children partially sensitive to the bitter taste (i.e., those with haplotypes PAV/AAV, PAV/AVV) were included in the taster haplotype group (PAV) (Table 5). The mean DMFT/dmft scores for the obesity, non-taster, obese_non-taster, and control_non-taster variables are presented in Table 6. The mean DMFT/dmft score for the study population was 3.017, and of these children, 56.2% were obese and 73.5% were non-tasters. Among non-tasters, obese children constituted 42.7% and children with normal weight constituted 29.8% of the population.
Equation 1, which was created to determine the DMFT/dmft index, depending on the obesity and non-taster dummy variants of the child in the Poisson model analysis, is presented below21:
where:
e – constant;
*, *** – statistical significance level of 10% and 1%, respectively.
A minus sign in front of the coefficient indicates a decrease in DMFT/dmft, while a plus sign indicates an increase.
Obesity, obese non-taster, control non-taster and the DMFT/dmft score
The covariates adjusted according to obesity and the absence of the bitter taste data while constructing the Poisson and negative binomial models for the determination of the DMFT/dmft index are presented in Table 7. Before interpreting the analysis results, the likelihood ratio (LR) test was applied to the 2 competitor models. It was observed that the truncated negative binomial model was more compatible with the data.
Equation 2, which was created to determine the DMFT/dmft index, depending on the obesity, obese_non-taster and control_non-taster variants of the child in the Poisson model analysis, is presented below21:
where:
e – constant;
*, **, *** – statistical significance level of 10%, 5% and 1%, respectively.
A minus sign in front of the coefficient indicates a decrease in DMFT/dmft, while a plus sign indicates an increase.
According to Equation 1, the DMFT/dmft index was lower in obese children and higher in non-tasters. According to Equation 2, obesity reduces the DMFT/dmft index, although the index was increased in obese non-tasters and decreased in normal-weight non-tasters.
Discussion
It is important to determine individual risk factors for dental caries in order to create a specific treatment procedure for a particular patient.22 Considering the close association between obesity and the eating habits, researchers have identified a link between obesity and tooth decay.23 Studies to date have yielded controversial results regarding the relationship between obesity and tooth decay, and further studies are required to understand the link better. A previous systematic review demonstrated that 48% of the investigated studies had reported no significant relationship between BMI and tooth decay; in contrast, a positive and a negative relation was found in 35% and 19% of the same studies, respectively.24 Hong et al. reported a positive relationship between BMI and tooth decay in children aged 60–72 months.25 However, this relationship was not significant when age, genetic predisposition and the eating habits were excluded from the analysis.25 In the present study, a comparison of the DMFT/dmft index for obese and normal-weight children was made, revealing a decreased index value in obese children, and thus hypothesis I was rejected. There are several factors that can be considered responsible for the inverse relation noted between DMFT/dmft and obesity. Children with multiple untreated decayed teeth may be undernourished, as they suffer from severe pain. Also, as a cause of infection, restlessness and sleep problems, tooth decay may decrease life quality in these children, negatively affecting their growth and development. Furthermore, most of the control group subjects were referred to our clinic with a complaint of pain and the control group had a higher incidence of tooth decay than expected, which may have affected our findings.
Many studies have indicated that diet, overweight, low weight, caries, and obesity are interrelated in children. Two recent systematic reviews support this assumption.26, 27 Therefore, it is reasonable to think that dental caries and obesity may be related to sweet taste genetics. The sugar intake and taste preferences have been associated with the TAS1R2 polymorphisms in humans. While a high sugar intake has been linked with caries and obesity, few studies have examined the genetic background.28, 29 Various polymorphism studies of the TAS1R2 gene have revealed a significant relationship between caries and genotypes.29, 30 In the present study, the risk of caries was higher in normal-weight children; it may have been due not to the lower incidence of caries in obese children, but to the fact that the population already had a high risk of caries.
A meta-analysis study suggested that TAS2R38 rs713598 SNP might play an essential role in caries.31 However, our study did not show significant results in any of the 3 SNPs, which is similar to a study by Shimomura-Kuroki et al.32 Since the TAS2R38 gene haplotype analysis includes the genotype analysis, the results regarding haplotypes are more critical.33 The physiology of taste has not been fully clarified to date, although the possible effect of the biological mechanism of taste on tooth decay and obesity appears to be worth investigating.34 The results of the present study demonstrate that tooth decay is associated with 3 different polymorphisms of the TAS2R38 gene, and the taster and non-taster haplotypes formed by these polymorphisms in obese and normal-weight children. Furthermore, the eating habits and the preferred foods, as the major factors affecting obesity and closely related to tooth decay, may be influenced by bitter taste genetics. There have been few studies to date investigating the relationship between taste genes, obesity and tooth decay, and the conducted ones have failed to clarify the relationship fully.14, 16, 35
The potential links between taste genetics and various disorders have been investigated in several studies.36, 37, 38 Accordingly, there is a growing interest in the effects of the biological mechanisms involved in taste sensation on the development of tooth decay and obesity.32, 38, 39 Studies investigating the relationship between the TAS2R38 polymorphisms and tooth decay reported a lower incidence of tooth decay among tasters. Wendel et al. reported that TAS2R38 was the main gene associated with tooth decay.40 A study conducted on infants revealed that TAS2R38 and TAS1R2 controlled their nutritional preferences for the weaning foods.41 On the other hand, a study conducted on adults argued that this effect might change with age, maternal dietary practices and community habits.42 Individuals with the PAV haplotype have greater sensitivity to the bitter taste and better gustatory perception. Due to their ability to sense different flavors, their tendency to cariogenic foods may be reduced.36 In the present study, the participants were classified into tasters and non-tasters, based on the haplotype analysis of the TAS2R38 gene. Three haplotypes of this gene generated by 3 different SNPs were examined (the corresponding amino acids were A49P, V262A and I296V). In the investigated SNPs, the rs713598 (C-G), rs1726866 (C-T) and rs10246939 (C-T) base exchanges were taken into account. According to the present study results, tooth decay decreases in the presence of obesity and increases in the absence of the bitter taste. However, in the subgroup analysis of non-tasters, the DMFT/dmft index was raised in obese non-tasters and lowered in normal-weight, control non-tasters, and thus hypothesis II was rejected. The authors suggest an increased risk of caries in the obese non-taster group. Further research on this topis can be done. More studies may be needed to explain this issue more clearly. Accordingly, the authors are planning to conduct different studies involving the same patient population. For example, the level of taste can be evaluated by applying solutions of bitter taste and the results can be compared with the genetic analysis.
This study has some limitations, such as keeping the sample size low, and not investigating other causes of caries and obesity.
The topic of taste has not been given the attention it deserves in dentistry or other branches dealing with the sensation of taste. The sensation of taste is a field that is not yet fully understood and there are many gaps in the acquired knowledge. There are branches in medicine that deal directly with the 4 senses of sight (eye), hearing (ear), touch (skin), and smell (nose). However, no specialty field exists for the sense of taste (tongue). The sense of taste and its genetics require support from studies, including the present one.
Conclusions
The CC control homozygous genotype showed higher caries rates in all SNPs of the TAS2R38 gene, although not statistically significantly. Although there were no statistically significant differences in the DMFT/dmft index with regard to TAS1R2 rs9701796 SNP in both control and obese groups, a high DMFT/dmft score was observed in the CC homozygous genotype. This may suggest that the CC genotype of TAS2R38 and TAS1R2 is prone to caries. Advice including dietary recommendations, increased oral hygiene and controlled calorie intake can be given to children with the identified taste gene polymorphisms.
Ethics approval and consent to participate
This cross-sectional, observational study was approved by the Ethics Committee of the Health Sciences Institute at Atatürk University, Erzurum, Turkey (No. B.30.2.ATA.0A10000-617), and was supported by the Scientific Research Projects Commission at Atatürk University (project No. 2012/66 and 2012/375). The participants’ parents provided informed written consent prior to any investigation.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.