Abstract
Background. Changes in the color of the teeth are a common dental finding associated with clinical and esthetic problems. Especially, the discoloration of primary teeth can cause parental concern and have a negative effect on social interactions between preschool children.
Objectives. The aim of the study was to evaluate the effect of pediatric drugs and an oral rinse on the discoloration of primary teeth.
Material and methods. Similar to medication intake recommendations, 7 primary teeth in each group were immersed for 1 min in one of 11 different solutions at 8-hour intervals for 1 week. The color values were obtained using a spectrophotometer (VITA EasyShade®) at baseline and after 1 week. The color change (ΔE*) values were calculated according to the CIELab system. The statistical analysis was conducted using the one-way analysis of variance (ANOVA) and Tukey’s post hoc tests at a p-value <0.05.
Results. When comparing values L*, a* and b* at baseline and day 7, a statistically significant difference was found in the a* value for the teeth immersed in pseudoephedrine (p = 0.012). There were also statistically significant differences with regard to color change at day 7 (ΔE*7) between the pseudoephedrine and chlorhexidine as well as pseudoephedrine and control groups (p = 0.034 and p = 0.030, respectively).
Conclusions. The ΔE*7 value for pseudoephedrine was 3.7 after 1 week, indicating that it may have the potential to cause significant tooth discoloration when used for a long period. Clinicians and children’s families should be aware of the fact that some pediatric drugs can cause tooth discoloration.
Keywords: pediatric, discoloration, drugs, primary teeth
Introduction
Tooth discoloration is a common dental finding associated with clinical and esthetic problems.1 The discoloration of primary teeth can cause parental concern and have a negative effect on social interactions between preschool children.2 Pigment accumulation can be caused by exogenous (foods, beverages and metals) and endogenous factors (systemic diseases or pulp necrosis).3
Cationic antiseptics, such as chlorhexidine and cetylpyridinium chloride, and other mouthwashes may cause staining after prolonged exposure.4 However, most evidence suggests that in an anionic diet,5, 6 the activated chromogens are a possible cause of staining.7 Some systemic drugs, e.g., minocycline, doxycycline, amox-clav (amoxicillin + clavulanic acid), and linezolid,8, 9 have also been shown to cause either extrinsic or intrinsic staining. The pH value, color and viscosity of the drug can play a role in the discoloration of the teeth.8, 9
In the treatment of pediatric patients, liquid pharmaceutical dosage forms, such as syrups, solutions and suspensions, are preferred.10 Although these liquid medications generally have a short duration of usage, they can be used chronically in diseases like respiratory allergies, asthma, attention deficit disorder, and epilepsy. Repetitive use for recurrent diseases, such as tonsillitis, otitis media, sinusitis, and allergic rhinitis, can also lead to significant exposure.11 The use of medications is particularly high in children under the age of 2.12 An increased exposure to such medications leads to tooth discoloration.13
Despite the presence of various types of measurements assessing tooth discoloration, the wavelength dispersive spectrophotometry is considered to be the most accurate method to evaluate tooth staining.2 The spectrophotometer is used to measure the tooth color by evaluating 3 color components independent of the surface being studied.14 These measurements are preferred, as they are more reproducible and objective than visual assessment.15
Although many studies discuss the influence of medications on the discoloration of permanent teeth, few studies refer to primary teeth.2, 9 This is an important subject, since primary teeth are different from permanent teeth in some respects – they have pores of a higher volume, thinner and more irregular calcific enamel, and lower mineral content – which makes them more prone to discoloration.16
The objective of the present study was to evaluate the effect of drugs containing sweeteners and colorants on primary teeth. This study aimed to raise awareness about the use of prescription drugs that cause tooth discoloration, as determined by their chemical and physical properties, and the duration of usage.
Null hypothesis (H0): Different types of pediatric drugs and oral rinses will not cause the discoloration of primary teeth.
Material and methods
This study was approved by the Scientific Research Ethics Committee at the Faculty of Medicine of Karadeniz Technical University, Trabzon, Turkey (No. 2017/86). The approval from the ethics committee was in compliance with the Declaration of Helsinki.
Teeth used
A total of 84 healthy, non-carious primary incisor teeth that had been recently extracted due to pre-shedding mobility were used in this study. Informed consent for the use of the extracted teeth was obtained from the parents of each patient. Teeth with developmental defects, enamel restorations, extrinsic/intrinsic stains, or white spot lesions were excluded from the study. Upon the collection of the teeth, they were placed in 0.5% chloramine T solution (Norateks Chemical Industry, Istanbul, Turkey) for 2 months. Prior to use, the teeth were cleaned with pumice water (Imipomza®; Imicryl, Konya, Turkey) by using a polishing brush (FlexiBrush®; Cosmedent, Chicago, USA) with a low-speed handpiece (KaVo Dental, Biberach an der Riss, Germany).
pH measurement
The medicines and solutions to be tested were prepared. The pH of these solutions was measured using a pH meter (HI 2211 pH/ORP meter; Hanna Instruments, Woonsocket, USA) before starting the experiment (Table 1).
Immersion cycles
The teeth were randomly divided into 12 groups (n = 7), with one group determined as the control group, and immersed in an electrolyte solution (sodium chloride (0.4 g/L), potassium chloride (0.4 g/L), calcium chloride-H2O (0.795 g/L), sodium dihydrogen phosphate-H2O (0.69 g/L), sodium sulfate-9 H2O (0.005 g/L), and 1,000 mL distilled water). The color of each tooth was measured at baseline and 1 week after immersion. Before the measurements, each tooth was washed with distilled water for 30 s, cleaned with a soft toothbrush (Colgate® Kids Barbie toothbrush; Colgate Palmolive, Mumbai, India) and gently air-dried.
Each test group was immersed for 1 min in a different pediatric drug solution and 1 oral rinse 3 times a day at 8-hour intervals for 1 week. After each immersion cycle, the teeth were washed with distilled water and kept in an electrolyte solution until the next cycle. The drug solutions and the electrolyte solution were refreshed every day.
Shade assessment
The color values for each sample were recorded by means of a spectrophotometer (VITA EasyShade®; Ivoclar Vivadent, Ellwangen, Germany), using the Commission internationale de l’éclairage (CIE) L*a*b* system, where the L* value measures the lightness or brightness of an object, a* is the measure of redness (positive) or greenness (negative), and b* is the measure of yellowness (positive) or blueness (negative).17
During the measurements, the teeth were placed in a viewing booth, which was completely covered with neutral gray cardboard and had a 5,500 K fluorescent lamp that imitated daylight at the top. The color measurements were taken at the center of the vestibular surface of the tooth. Three measurements were taken for each tooth and the average of these measurements was recorded. By using the L*, a* and b* numerical values, the color change (ΔE*) values were calculated with the following formula (Equation 1).
where:
ΔL* – difference between the L* values measured
at different times on the same tooth;
Δa* – difference between the a* values measured
at different times on the same tooth; and
Δb* – difference between the b* values measured
at different times on the same tooth.
Statistical analysis
The statistical analysis was performed using the SPSS Statistics for Windows software, v. 17.0 (SPSS Inc., Chicago, USA). The normality of the data was tested using the Shapiro–Wilk test. The one-way analysis of variance (ANOVA) and Tukey’s post hoc tests were used for comparing the ΔE* values among different groups. The paired sample t tests were used for comparing the L*, a* and b* values at baseline and day 7. Both kinds of tests were conducted with a significance level set at p < 0.05.
Results
Shade assessment analysis
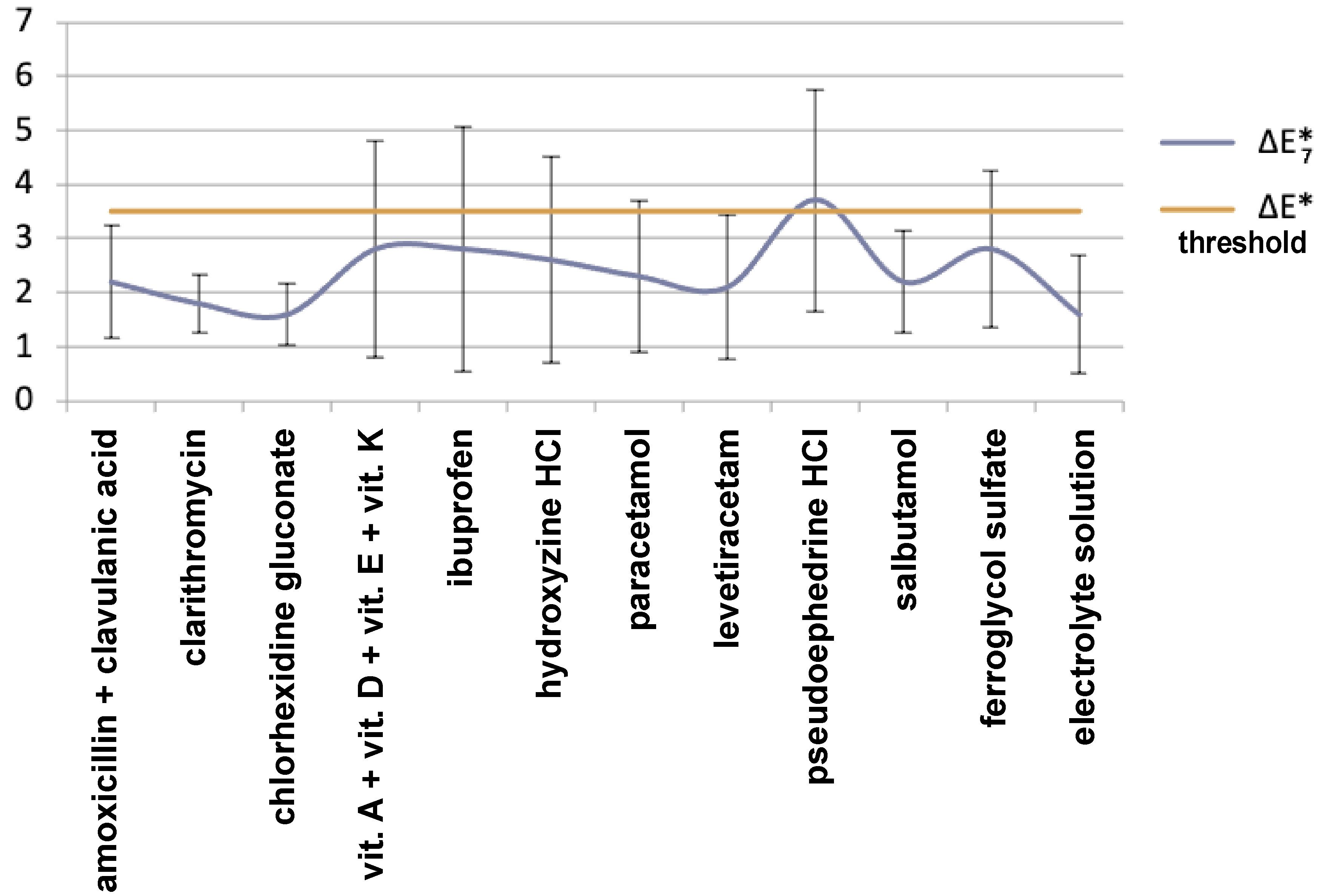
The one-way ANOVA revealed that there were statistically significant differences with regard to color change at day 7 (ΔE*7) between the pseudoephedrine and chlorhexidine as well as pseudoephedrine and control groups (p = 0.034 and p = 0.03, respectively) (Table 2). Considering changes in the L*, a* and b* values between baseline and day 7 (ΔL*, Δa* and Δb*) in each group, a statistically significant difference was found in the a* value for the sample immersed in the pseudoephedrine drug solution (p = 0.012). There were no statistically significant differences in the L*, a* and b* values for the samples immersed in the other drug solutions or for the control group (p > 0.05) (Table 3). The highest and lowest ΔE*7 values were found for pseudoephedrine (3.7) and chlorhexidine (1.6), respectively (Table 2).
pH measurement analysis
The pH values of the evaluated drugs ranged from 2.76 (pseudoephedrine) to 6.62 (paracetamol). Clarithromycin, Ferro Sanol® B, Nutrigen® Omega-3, ibuprofen, hydroxyzine, salbutamol, and pseudoephedrine had pH below the critical value (5.5), while amoxicillin + clavulanic acid, levetiracetam, paracetamol, and benzidamine HCl + chlorhexidine gluconate had the pH values above 5.5 (Table 1).
Discussion
The null hypothesis (H0) was rejected. No significant differences were found in the L*, a* and b* values for the teeth immersed in various drug solutions except for the teeth immersed in pseudoephedrine. These results can be related to many factors, such as the structure of the teeth, their susceptibility to coloring, the pH value, color and viscosity of the drug, and oral rinses.18
The systemic or local usage of pediatric drugs can cause erosion, caries as well as tooth discoloration related to such factors as the pH value, acidic component and viscosity of the drug.
These problems may affect primary dentition, which is important for a child’s psychology, nutrition, speaking, esthetics, and permanent dentition.19, 20, 21 Generally, researchers have studied the discoloration of dental materials and permanent dentition by medications6, 7, 8, 18, 22; however, there is limited knowledge about the effects on primary dentition.2, 9 The commonly used pediatric drugs may influence the texture of primary teeth and result in their discoloration.
Saliva is known to be a protective factor against the development of erosion and caries in the teeth. The protein-based pellicle covers the surface of the tooth and prevents contact between the tooth surface and acids that can cause demineralization.23, 24 Investigators have reported that some drugs, iron salts and certain antimicrobials can cause the extrinsic discoloration of the teeth, which is reduced by brushing over the pellicle.21, 22 Moreira et al. reported the discoloration of bovine teeth caused by different mouthwashes.25 The alcohol-containing types of mouthwash can produce more significant changes as compared to other oral rinses. The alcohol content and a low pH value are associated with the demineralization of the teeth. The lack of significant differences in the group of oral rinses containing 0.15% benzydamine HCl and 0.12% chlorhexidine gluconate is thought to be related to not using any foods or drinks that would cause the pellicle formation; chlorhexidine causes discoloration through the plaque formed on the tooth surface.19, 20 In this study, the use of an electrolyte solution rather than artificial saliva may have prevented the pellicle formation on the observed teeth. This can be considered a limitation of the study, and can be associated with color changes that may not be clinically relevant.
Tüzüner et al. reported that different types of drugs were associated with the potential risk of discoloring dental materials.18 Ayaz et al. observed that anti-asthmatic drugs caused the discoloration of dental materials.17 In the present study, similar to previous research,2, 8, 19, 20 all drug groups caused color alterations, but only the pseudoephedrine group reached statistical significance. When comparing primary and permanent dentition, primary teeth have pores of a higher volume, thinner and more irregular calcific enamel, lower mineral content, and a different chemical composition of the pellicle.16 Thus, the structure of the teeth, the enamel and dentin thickness, the color of dentin, and/or microcracks may be related to discoloration26 and affect the color changes observed on the tooth surface.27 Due to these natural differences, in the current study, discoloration was found to be statistically significant only in the pseudoephedrine group. Additionally, each tooth can display a range of colors from the gingival margin to the incisal edge,28 and thus may show different degrees of discoloration when compared with another tooth despite the same oral conditions. To eliminate this effect, the color values were measured at the same surface area in each tooth in our study.
Pani et al. reported that the different iron syrups evaluated in terms of their effects on primary teeth, including syrups of a low iron content, caused less discoloration than other drug groups.2 Although the reasons for the discoloration caused by iron drugs are not clear, the most plausible theory is linked to the pellicle. Among the etiological factors, dietary components, beverages and medications are indicated in all populations, while in children, chromogenic bacteria are also considered.28 Besides, the lesser color change due to the iron-containing medication, Ferro Sanol B, observed in the present study can be related to the shorter time of its usage. Prior to the color analysis of each sample, the teeth were cleaned with the help of a soft toothbrush. Therefore, it is thought that the initial discoloration may have been decreased.29
As mentioned above, investigators have reported that drugs of lower pH or a higher sugar content may demineralize the teeth, and cause erosion and caries.16, 21, 30 Thus, low-pH drugs can cause changes in the tooth surface properties, like roughness,11, 20 and enhance the adhesion of color pigments.22 It is known that rough surfaces retain stains better than smooth surfaces.22 In the present study, the pH values of each drug were measured and the lowest pH value was noted for pseudoephedrine. Therefore, the significant discoloration observed in the pseudoephedrine group can be related to the drug having lower pH as compared to other drug groups, which affected the tooth surface and increased the adhesion of colorants, in accordance with the colorant absorption theory.22
In the present study, even though there was no difference in the L*, a* and b* values at the end of day 7 (p > 0.05), the color of the teeth in the pseudoephedrine group turned reddish, as observed with an increase in only the a* value (p = 0.012; p < 0.05). This red color may be related to the color of pigments and their absorption by the tooth surface. Ponceau 4R (Food Red 7, Acid Red 18, E124) is a water-soluble, sulfonated azo dye widely used in the food industry to provide the red color.31 The raspberry essence, and particularly Ponceau 4R, are the ingredients responsible for the red color of pseudoephedrine. It is thought that Ponceau 4R, which has an absorbance at 510 nm wavelength, causes apparent discoloration that does not go away with brushing due to the percolation of pseudoephedrine into the dentinal tubules.
The ΔE* value indicates whether there is a color change between 2 time periods.25 This refers to perceptibility and acceptability thresholds for color differences in dental matching. Clinical color matching can be graded according to the ΔE* values. The ΔE* value represents the numerical distance between the coordinates L*, a* and b* and the relative color variations an observer reports for the materials.22 According to Dancy et al., when the ΔE* value is 0, it indicates a perfect color difference, 0.5–1.5 means very good, 1–2 means good , 2–3.5 refers to a clinically detectable change, and more than 3.5 to an unacceptable change in color.32
According to the findings of our study, the sample immersed in pseudoephedrine exceeded the limit of a clinically acceptable color change (ΔE* > 3.5) (Figure 1). This can be explained by the fact that colorants in this drug had different polarities. Components with a higher polarity are eluted first, while those with a lower polarity are eluted later. Although there are yellow colorants in both coffee and tea, discoloration by coffee has been reported to be more profound due to the absorption and adsorption of its polar colorants into/onto the surface of materials.33 Similarly in our study, although some discoloration could be removed by brushing, the polar colorants of pseudoephedrine were absorbed into and adsorbed onto the surface of teeth to a greater extent.
In our study, the teeth were kept in 0.5% chloramine T solution. This is the recommended solution for infection control in research projects, as it does not affect the organic phase of dentin. However, it may influence the bonding strength to dentin with a long-term use.34 This should be kept in mind, as it may have negatively affected the in vitro conditions of our study.
No regular brushing of the teeth was performed in the present study. However, after each immersion cycle, the samples were placed in an electrolyte solution, following immersion in distilled water. This procedure was meant to imitate the drinking of water or rinsing with water after the intake of each drug. In future studies, brushing may be recommended to determine how much true staining will occur. In this study, brushing was conducted only before the measurements – at baseline and day 7. In the latter case, it was performed to check the tenacity of the stains and whether they were reversible. In this study, the drugs were evaluated for a duration of 1 week. However, some drugs are used for longer periods of time, which may have a greater effect on the discoloration of primary teeth. In vivo studies are recommended to further evaluate the effect of various drugs on tooth discoloration.
Conclusions
Within the limitations of the present study, it can be reported that, contrary to H0, pseudoephedrine caused the discoloration of primary teeth. It produced a statistically significant difference in the a* value after 1 week of use as compared to baseline. This situation should be taken into consideration by the physicians prescribing this drug.
Ethics approval and consent to participate
This study was approved by the Scientific Research Ethics Committee at the Faculty of Medicine of Karadeniz Technical University, Trabzon, Turkey (No. 2017/86). The approval from the ethics committee was in compliance with the Declaration of Helsinki. Informed consent was obtained from the parents of each participant.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.