Abstract
Background. Dental caries is an infectious microbial disease of the teeth, affecting mostly young children. It is caused by the interplay of numerous factors that are more common in susceptible and lower-income groups. Therefore, there is a dire need for a simple yet effective method of treating dental caries.
Objectives. The aim of the study was to compare the effectiveness of 38% silver diamine fluoride (SDF) and atraumatic restorative treatment (ART) in the treatment of dental caries in a school setting.
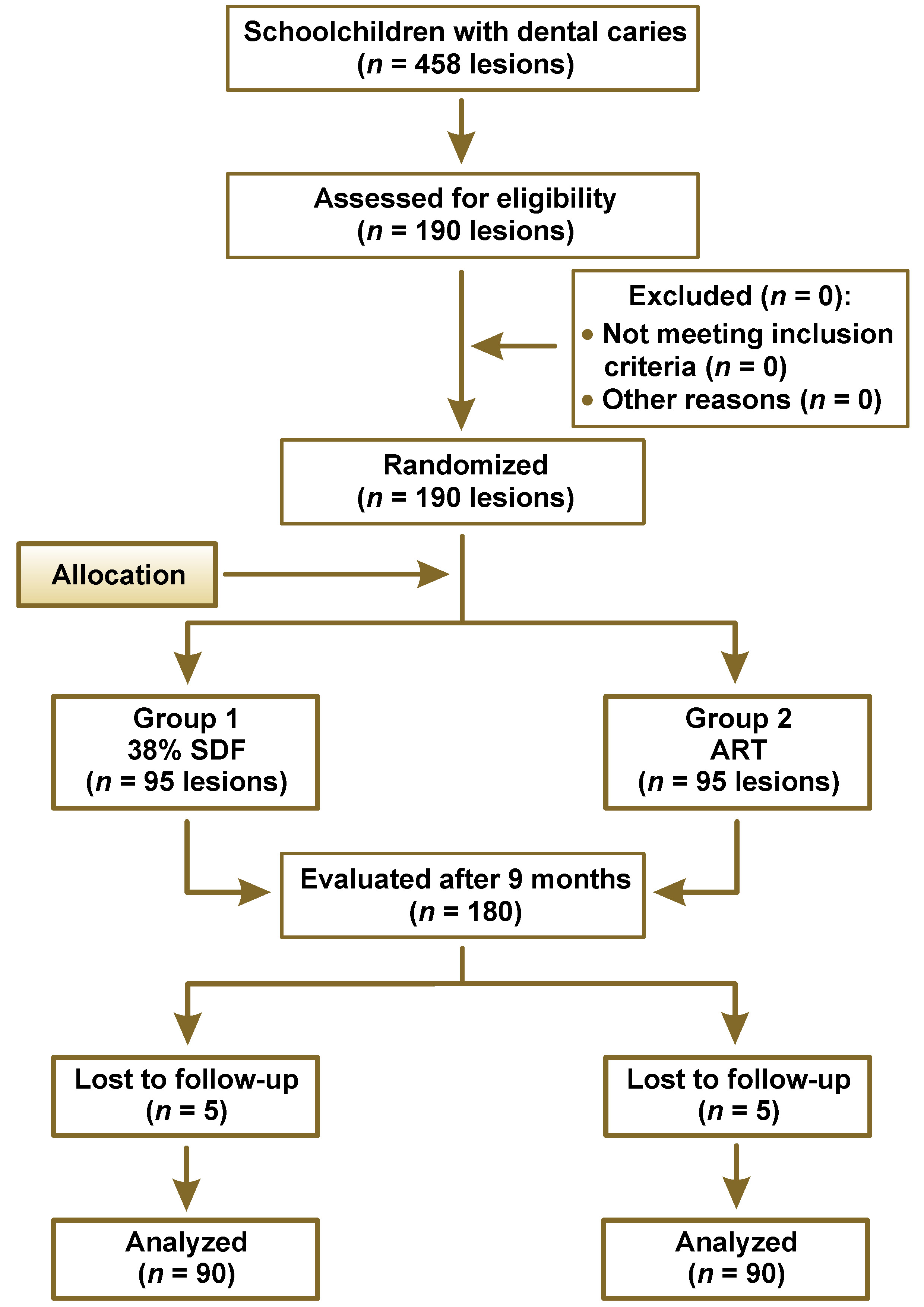
Material and methods. A randomized clinical trial (RCT) using a parallel-group design was conducted among schoolchildren aged 6–12 years. Oral hygiene practices and sugar exposure were recorded at baseline. In the schoolchildren, 190 dental caries lesions were restored using 38% SDF (group 1) or ART (group 2). The χ2 test and the Kaplan–Meier survival analysis were done to assess the 2 treatment modalities. The RCT was carried out and reported in accordance with the CONSORT (Consolidated Standards of Reporting Trials) checklist.
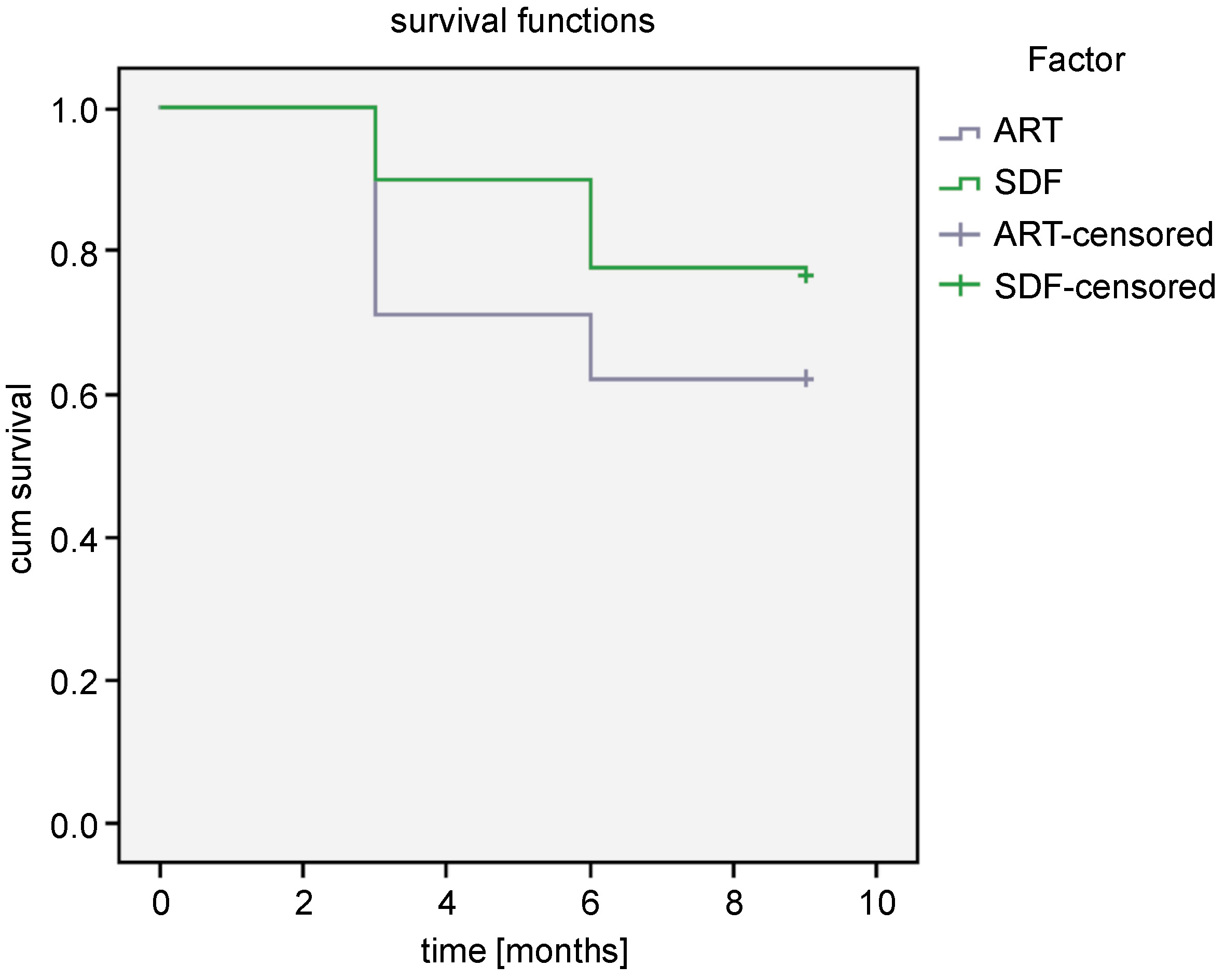
Results. A total of 190 children fulfilled the inclusion criteria and the mean age of the study population was 9.3 ±1.3 years. The majority of the participants brushed their teeth once daily, using a toothbrush, rinsed their mouth after meals and had optimal sugar exposure. In measuring the outcome of the interventions after 9 months, 58.9% of the participants from group 1 had their restorations intact as compared to 47.8% in group 2, and this was found to be statistically significant (p = 0.004). The survival analysis using the log rank test showed 38% SDF to be better in comparison with ART.
Conclusions. This study indicated that SDF was better at arresting caries, and hence it can be considered a viable treatment option in areas with limited access to oral healthcare.
Keywords: dental caries, silver diamine fluoride, dental atraumatic restorative treatment, dental care for children
Introduction
Dental caries is an infectious microbial disease of the teeth, affecting mostly young children. It is caused by the interplay of numerous factors, and is more common in susceptible and lower-income groups. Especially in areas with limited access to dental services, the treatment of dental caries is a serious concern. Untreated dental caries has a negative influence on self-esteem, the intake of food and sleep, and it also hampers daily activities.1 Therefore, there is a dire need for a simple yet effective method of treating dental caries. Usually, the treatment of caries requires technologically advanced dental equipment as well as a skilled and well-trained professional, thus making it an expensive treatment modality.1 Developing and underdeveloped countries present with unmet needs due to the underutilization of the available services. Moreover, carrying out the treatment procedures poses a challenge with regard to children due to their limited adaptive capability.2
The use of rotary instruments causes vibrations and noise, and increases the temperature of the cut surface, raising the anxiety of an already distressed pediatric patient. It also poses the risk of pulpal exposure, weakening the tooth structure and postoperative pulpal pain. Due to the scarcity of equipment and trained manpower in most underdeveloped or developing regions, the conventional restorative dentistry is not a viable treatment option.3
Atraumatic restorative treatment (ART) came into picture in 1985 to surpass the shortcomings of the conventional restorative treatment, specifically targeting those who did not have access to dental care.3, 4 Atraumatic restorative treatment involves the excavation of carious tissue only with the use of hand instruments, thereby foregoing the use of electrically operated equipment, followed by the insertion of a filling material, such as glass ionomer cement (GIC), resin-modified GIC (RMGIC), composite resins, and compomers.3, 5 It is a biologically favorable approach with the conservation of the tooth structure by removing only the demineralized dentin while providing restorative care away from the traditional dental set-up, thus lowering the cost of dental care.6, 7, 8
However, the provision of ART also requires the participation of skilled and trained manpower, which is still a challenge in areas with limited access to dental care. In recent times, the use of minimally invasive dentistry and caries-arresting treatment has gained worldwide acceptance. For the remineralization of carious lesions, fluorides have been used extensively. Silver diamine fluoride (SDF) with the molecular formula Ag(NH3)2F was approved by the US Food and Drug Administration (FDA) in 2014 and since then, it has been used as an effective caries-arresting material.
Different studies conducted by Chu and Lo,9 Llodra et al.10 and Yee et al.11 found that SDF could serve as a substitute for restorations that require technique-sensitive procedures, and could effectively arrest caries. In a clinical trial conducted by Zhi et al., it was observed that SDF arrested 70% of carious lesions in the primary anterior teeth of Chinese preschool children.1 The application of SDF was considered to be painless, comfortable and acceptable in taste by the parents of children in a study conducted by Clemens et al.12 The use of SDF offers a dual advantage of remineralization and antimicrobial effect due to the fluoride and silver content, respectively, without the need of using instruments for the excavation of carious tissue.
However, the use of SDF causes the discoloration of the teeth, which may not be esthetically pleasing. This warrants a search for an effective restorative material that can enhance the cosmetic appearance. Glass ionomer cement can be used, as it is tooth-colored and contains a high concentration of fluoride ions, which aids in arresting active caries by remineralizing carious lesions and preventing further caries development.
Therefore, the present study aimed to compare SDF with ART as the positive control. The null hypothesis assumed that there would be no difference in the effectiveness of 38% SDF and ART in terms of arresting dental caries in schoolchildren.
Material and methods
A randomized parallel-arm clinical trial was carried out to compare the effectiveness of 38% SDF and ART in the treatment of dental caries. The trial was registered at Clinical Trials Registry – India (www.ctri.nic.in) (REF/2020/06/034629).
Ethical consideration
Informed written consent was obtained from the parents before clinical examinations and verbal assent from the children at the time of the procedure. The Ethical Review Board of the Institute of Medical Sciences and SUM Hospital at Siksha ‘O’ Anusandhan Deemed to be University, Bhubaneswar, India, granted the ethical clearance for the study (ref. No. DMR/IMS.SH/SOA/180316).
Study population
The study was conducted in the public schools belonging to the district of Khordha, Odisha, India. Schoolchildren aged 6–12 years were considered for the study, as dental caries prevalence is usually higher in this age group.13, 14 The sample size was calculated after a pilot study on 10 patients. Using the G*Power statistical software, v. 3.1.9.4 (https://www.psychologie.hhu.de/arbeitsgruppen/allgemeine-psychologie-und-arbeitspsychologie/gpower), at a power of 90% with an effect size d = 0.5 and a two-tailed type I error of 0.05, the sample size was set at 172 dental caries lesions, with 86 lesions in group 1 and group 2 each. The sample size was increased by 10% to 190 to account for any loss due to follow-up/attrition.15
Children with a minimum of 1 carious lesion, code V and VI, not involving the pulp, according to International Caries Detection and Assessment System (ICDAS), in any of the completely erupted permanent molars were recruited to the study.16 Only occlusal lesions were included. The information regarding SDF and ART was given to the parents, and a written consent was obtained from them. The children were also explained the procedures and their verbal consent was sought. Those children who did not fulfil the age criteria or presented with pain, tooth mobility, signs of pulpal involvement, or the destruction of more than ⅓ of the crown were excluded.
Study design
The study was conducted in 3 phases over a period of 11 months. It was a prospective parallel randomized clinical trial (RCT) with a follow-up at 3, 6 and 9 months. The study participants were randomly allocated into 2 groups according to a sequence of random numbers, which was generated using Microsoft® Excel, v. 2007 (Microsoft Corporation, Redmond, USA).
Data collection
Permission was obtained and a schedule was prepared in consultation with the school authorities regarding the sequence of interventions to be carried out on the premises of 6 selected schools. Oral hygiene practices, like the frequency of tooth brushing, brushing aids, the oral rinsing habit, and sugar exposure, were recorded through a self-designed questionnaire at baseline.
Restoration of the teeth in the SDF group
In the children from group 1 (SDF), the identified carious lesion in the affected tooth was efficiently isolated, and petroleum jelly was applied to protect the adjacent teeth and mucosa. Silver diamine fluoride (FAgamin® Silver Diamine Fluoride 38%; Milestone Healthcare, Raipur, India) was applied directly to the lesion with a micro-brush and left for 2 min, and then the tooth was cleaned using a dampened cotton pellet. The treated tooth was restored with GIC (Fuji® IX; GC Corporation, Tokyo, Japan). Excess was removed using a cement carver after checking for high points by asking the patient to bite gently. The parents were instructed to prohibit the child from eating or drinking for 30 min after the application.12, 17, 18
Restoration of the teeth in the ART group
In the children from group 2 (ART), carious dentin was removed with spoon excavators of different sizes – small (Ash 153/154), medium (Ash 131/132) and large (Ash 127/128), depending on the cavity size. Caries was removed using circular scooping motions and the cavity was widened with a dental hatchet (Ash 10-6-12). The prepared cavity was conditioned for 10–15 s, using a dentin conditioner that comprised 10% polyacrylic acid. Glass ionomer cement (Fuji IX; GC Corporation) was mixed according to the manufacturer’s instructions and the cavity was filled in increments, using the blunt end of the carver (Ash 6). The finger-press technique was used to contour the excessive restorative material along the slopes of the cusps. The operating area was kept moisture-free for 2 min and the bite was checked for occlusion. Post-restorative instructions were to avoid the intake of food and drinks for a minimum of 1 h.3, 5, 7, 19
Follow-up examination
The follow-up examinations were carried out at 3-, 6- and 9-month intervals by one of the researchers (DS). The evaluation was done using the community periodontal index (CPI)-probe (WHO-probe) and a mouth mirror. The treated lesions were classified according to the evaluation scores which were modified from those used by Francis et al.20: score 1 – the restoration intact, covering all pits and fissures; score 2 – the restoration partially lost, the tooth is sound (no active/soft caries); score 3 – the restoration partially lost, the tooth is carious(active/soft caries); score 4 – the restoration completely lost, the tooth is sound; and score 5 – the restoration completely lost, the tooth is carious. The tooth was considered sound if its surface felt hard and shiny on gentle probing, and carious in case of soft, demineralized surface. The teeth with the restorations lost and with caries were restored using the conventional treatment in hospital. Due to the loss to follow-up, only 180 restorations were available after 9 months (Figure 1).
Statistical analysis
All the collected data was recorded and entered into a Microsoft Excel sheet. The descriptive and inferential analyses were done with the use of the IBM SPSS Statistics for Windows software, v. 23.0 (IBM Corp., Armonk, USA), by one of the researchers (IM), who was blinded to the treatment options and the evaluation scores. Statistical significance was fixed at a p-value <0.05. The χ2 test was used to assess differences between the treatment modalities. The Kaplan–Meier survival analysis was performed using the log rank test to check the survival of both kinds of restorations.
Results
A prospective RCT was conducted to evaluate the effectiveness of 38% SDF with GIC and ART among 6–12-year-old schoolchildren. The demographic variables of the participants are depicted in Table 1. The 2 groups did not differ significantly with regard to these variables at baseline.
In measuring the outcome of the interventions, 58.9% of the participants from group 1 had their restorations intact as compared to 47.8% in group 2, and this was found to be statistically significant (p = 0.004) (Table 2). In Table 3, the most common evaluation score among all restorations was ‘an intact restoration covering all pits and fissures’ (53.3%), followed by score 2 (a sound tooth with a partial loss of the restoration). There were no decayed teeth with a complete loss of the restoration (score 5) in group 1. The arrest of dental caries was also better with 38% SDF, as the percentage of carious teeth with the loss of the restoration was 5.6% in comparison with 16.7% in the ART group (p = 0.025). The survival analysis using the log rank test showed 38% SDF to be better in comparison with ART (Table 4, Figure 2).
Discussion
Untreated carious lesions and the underutilization of oral healthcare services are important community health problems in developing and underdeveloped countries. Children are often afraid of anesthetic procedures, long treatment duration and the use of numerous instruments. Hence, treatment involving minimal intervention that is less technique-sensitive is preferred over the conventional dental caries treatment procedures. Many minimally invasive techniques, like ART, which includes the excavation of carious tissue with hand instruments, followed by restoration, have been used for treating dental caries in children and adults. On the other hand, recently, SDF has gained attention because of its caries-arresting and remineralizing effectiveness that is achieved without the excavation of soft carious tissue.21 A study conducted by Clemens et al. suggested that SDF was the preferred method for arresting active caries lesions in primary teeth among 2–5-year-old children.12 Similar findings were also reported in studies by Chu and Lo9 and Mei et al.,22 where the application of 38% SDF was better at arresting caries in comparison with fluoride varnish. Yee et al. found SDF to be an effective caries-arresting agent in 3–9-year-old children in Nepal after a follow-up of 12 months.11 Another study by Llodra et al. compared the effectiveness of 38% SDF with ART in the permanent teeth of 6-year-old children; the authors found that SDF reduced caries incidence by 79%.10 Since the application of SDF is simple and does not require training, it can be implemented by primary healthcare workers in areas of low dental accessibility.
The outcome of the restorations was measured and compared between the 2 techniques after 9 months. Caries arrest by SDF was evaluated with scores that estimated the retention or loss of the restorative material, sound or carious soft dentin, along with its color and consistency, which was similar to the studies carried out by Llodra et al.10 and Fung et al.23 This evaluation was done using the WHO probe, similar to the studies by Zhi et al.1 and Dos Santos et al.24 There was no major difference between SDF and ART with respect to score 1, where the restoration was intact, but there was a significant difference between the 2 modalities, with SDF having only 5.6% of the teeth with score 3 as opposed to 16.7% in the case of ART. This was probably due to the remineralization of carious tissue by 38% SDF, which aided in arresting progressive caries. Studies have ascertained that SDF causes remineralization through various probable mechanisms,25, 26, 27, 28 the first being the occlusion of the dentinal tubules by silver, which demonstrated reduced dye permeability and electric resistance.2 Silver and its compounds arrest caries by blocking acid diffusion and sealing the dentinal tubules against the entry of microorganisms. Further growth of microbes is inhibited by the oligodynamic action of silver.25 The other mechanisms could be the reactions between the tooth minerals and SDF. The fluoride released from SDF amplifies the resistance of the dentin, which results in a decreased penetration of acids.26 It has been observed that SDF (Ag(NH3)2F) reacts with hydroxyapatite (HA) to release calcium fluoride (CaF2) and silver phosphate (Ag3PO4), which reinforces the affected dentin.9 This may be the reason why the teeth were sound and no soft carious tissue was present, even after the restoration was partially or completely lost. This finding is similar with the results of Zhi et al., who concluded that the application of an SDF solution or high fluoride-releasing glass ionomer resulted in arresting active dentin caries.1 Caries arrest by SDF has been reported by various studies, including those by Chu and Lo,9 Llodra et al.,10 Clemens et al.,12 Fung et al.,23 and Yamaga et al.29
Silver diamine fluoride showed better retention of the restoration (58.9%) than ART (47.8%) with respect to score 1. The lesser retention in the case of ART is probably the result of the technique-sensitive manual excavation of caries as opposed to the brush application of SDF. As mentioned by Gupta et al., SDF reacts with the tooth surface to produce silver phosphate, which then reacts with RMGIC to form hydroxyapatite and fluorapatite, which may also contribute to increased bond strength.30
The most common side effect of SDF is the staining of the teeth and oral mucosa due to improper isolation. This staining is the result of the oxidation of silver and it affects only the damaged portion of the tooth; healthy enamel is not affected.12 However, there was no instances of oral mucosal staining in our study.
In the present study, ART scored higher in comparison with SDF with respect to scores 3 and 5, which represented teeth that were carious even after restoration. This could be explained by the fact that caries arrest due to the fluoride release from GIC ceased once the restoration was lost, and hence the remineralizing effectiveness of GIC was also reduced. Other causes could be seepage at the margins of restorations, secondary caries and improper isolation.31 The loss of the restoration could be due to the lack of a proper retentive form, as the cavity preparation in ART is done solely with the use of hand instruments. Also, the fact that ART is a technique-sensitive procedure cannot be overlooked.
Our study found that caries arrest was better in group 1, which was reflected by 58.9% of the teeth recording score 1. Similar findings were also reported in studies conducted by Zhi et al.,1 Llodra et al.,10 Fung et al.,23 and Vollú et al.32 The analysis also showed that the survival of the SDF restorations was higher than in the case of ART, and this was similar to the findings of Raskin et al.33 This may be a consequence of the remineralizing effect of SDF without requiring a proper cavity form, technical skills and or the use of complex armamentarium. Due to the abovementioned advantages of SDF, it can be used with little or no training by primary healthcare workers in areas with the shortage of dental manpower.
Limitations
The current study was conducted over a period of 9 months; a longer follow-up would give a clearer idea about the retention of restorations. Certain outcomes associated with the use of SDF, such as the staining of the teeth and mucosa, was not assessed, as that was not part of the primary objective of the study. The occurrence of secondary caries could not be evaluated, as radiographs were not available in the field setting where the study was undertaken. Further studies could explore the cost effectiveness of SDF as opposed to ART.
Conclusions
Silver diamine fluoride was found to be an easy, effective and well-received minimally invasive approach for treating dental caries among schoolchildren. The treatment of the teeth with SDF does not necessitate the presence of a well-equipped dental set-up or the use of costly instruments. Hence, SDF can be used effectively in developing countries as a caries-arresting agent in community-based programs.
Trial registration
The trial was registered at Clinical Trials Registry – India (www.ctri.nic.in) (REF/2020/06/034629).
Ethics approval and consent to participate
The study was approved by the Ethical Review Board of the Institute of Medical Sciences and SUM Hospital at Siksha ‘O’ Anusandhan Deemed to be University, Bhubaneswar, India (ref. No. DMR/IMS.SH/SOA/180316). Informed written consent was obtained from the parents before clinical examinations and verbal assent from the children at the time of the procedure.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.