Abstract
Background. Wearing masks has become an essential safety measure during the coronavirus 2019 (COVID-19) pandemic. Especially clinicians in dental clinics should focus on infection control. However, there is currently no data regarding the frequency of replacement of the masks used in hospitals. Hence, it is necessary for dental clinic staff, who deal with many patients in an aerosol-producing environment, to have precise mask-wearing guidelines.
Objectives. The aim of this study was to evaluate the contamination on the inner surface of the masks used by clinicians in dental clinics and provide basic data to describe hospital infection control guidelines in greater detail.
Material and methods. For Study I,12 participants were recruited. The experiment was conducted indoors. After wearing the mask, the temperature and the humidity inside the mask were measured at the set time points (immediately after wearing the mask, and 10 min, 30 min, 1 h, 2 h, and 4 h after wearing the mask). During the experiment, talking was not allowed. For Study II, 23 clinicians from dental clinics were recruited. After wearing the mask, the temperature, the humidity and the number of colony-forming units (CFU) inside the mask were measured at the set time points. Finally, 15 samples were selected for the study based on a survey. Bacterial identification was conducted using the 16S rDNA sequencing.
Results. The temperature and the humidity inside the mask increased significantly relative to room temperature and room humidity, respectively. Bacteria were found in all the masks worn for more than 10 min and the CFU values increased with the mask-wearing time. Bacteria belonging to the genera Staphylococcus, Bacillus and Roseomonas were detected in the used mask.
Conclusions. A mask should not be worn for more than 2 h; however, the frequency of mask replacement can vary, depending on the number of patients encountered and the working environment.
Keywords: bacterial contamination, mask contamination, inner surface of masks
Introduction
During the coronavirus disease 2019 (COVID-19) pandemic, wearing masks has become an essential safety measure to protect oneself and others.1 However, patients who visit dental clinics have to take off their masks and keep their mouths open during treatment. In addition, the handpieces and the ultrasonic equipment used in dental clinics produce aerosols that are contaminated with the patient’s saliva and blood.2 Therefore, dental clinic staff should focus on infection control. With regard to personal protective equipment (PPE) for infection control, it is reported that masks can filter 60–95% of aerosols.2 However, the filtering effect depends on the material and shape of the mask; if the fit is incorrect, the unfiltered microorganisms can penetrate through the mask.3 Various microorganisms, such as bacteria,4, 5, 6, 7, 8 viruses9, 10 and fungi,8 have been detected in masks. The contamination of masks by these microorganisms comes from the surrounding environment8 or from individuals.4, 10
It is predicted that mask contamination is greater on the inside than on the outside,4, 5 since in the former case, the mask is in direct contact with the human skin and oral microorganisms may be captured by the mask during conversation. In addition, considering the temperature and humidity factors, essential for bacterial growth, breathing allows the maintenance of relatively warmer temperatures and higher humidity inside the mask than outside it.
If the mask is contaminated, it is replaced with a new one to reduce the risk of infection. However, most people use masks daily. In addition, most clinicians replace gloves on a patient-by-patient basis, but the mask is often used for the entire day.
One study confirmed that pathogenic bacteria accumulated when both surgical and cotton masks were worn for more than 4 h,11 and according to the Australian Dental Association (ADA) infection control guidelines, the filtration capacity of the mask starts to decrease after about 20 min, as moisture fills the inner and outer surfaces of the mask.12 According to the World Health Organization (WHO) recommendations, medical masks are for a single use only, and once used, they should be discarded immediately.13
Hence, it is necessary for dental clinic staff, who deal with many patients in an aerosol-producing environment, to have precise mask-wearing guidelines.
Therefore, the aim of this study was to evaluate the contamination on the inner surface of the masks used by clinicians in dental clinics. This study provides basic data to describe hospital infection control guidelines in greater detail.
Participants and methods
This study was approved by the Ethics Committee of Ulsan College, South Korea (No. 1044363-A-2021-001).
Measurement of changes in temperature and humidity (Study I)
After thoroughly explaining the purpose of the study and its procedures, 12 participants (mean age: 27.2 ±2.9 years, no medical or dental history of a general disease, free of medication) were recruited having provided written informed consent (Table 1). The experiment was conducted in June 2021, indoors on clear days, except cloudy or rainy days. The windows and the doors were closed, and the experiment started at 9 a.m. The participants were given the same type of mask (Korea Filter Anti-Droplet (KF-AD) mask; Hwajin Industry, Yeongcheon, South Korea). The participants were helped to fit the masks to their facial shapes. After wearing the mask, the temperature and the humidity inside the mask were measured with a thermometer (Thermo-Hygrometer Pocket/Digital; Daihan Scientific, Seoul, South Korea) and recorded at the set time points (immediately after wearing the mask, and 10 min, 30 min, 1 h, 2 h, and 4 h after wearing the mask). During the experiment, the participants sat on chairs without talking and stayed comfortable, spending time freely, using books or laptops. The researcher continued to monitor the participants, and if they sneezed, coughed or talked, the experiment was stopped and repeated.
Measurement of the number of bacteria (Study II)
After thoroughly explaining the purpose of the study and its procedures, 23 clinicians working at a dental hospital in Ulsan, South Korea (no medical or dental history of a general disease, free of medication) were recruited having provided written informed consent (Table 2). The experiment was conducted in June 2021, indoors on clear days, except cloudy or rainy days. The windows and the doors were closed, and the experiment started at 9 a.m. The clinicians were given the same type of mask (KF-AD mask). Before distributing the masks, a square shape (1 cm × 1 cm) was drawn in the center of each mask and the mask was ultraviolet (UV)-sterilized for more than 40 min. After sterilization, the masks were sealed in sterile zipper bags and distributed at the dental clinic. To prevent cross-contamination by hands, the clinicians washed their hands and wore exam gloves. The researcher first observed the participants to check for the presence of cross-contamination and immediately replaced the contaminated masks with new ones. The sterilized masks were worn using only the ear loops to avoid touching the inner surface of the mask. The clinicians were helped to fit the masks to their facial shapes. After wearing the mask, the temperature and the humidity inside the mask were measured and recorded at the set time points (immediately after wearing the mask, and 10 min, 30 min, 1 h, 2 h, and 4 h after wearing the mask). During the experiment, the clinicians worked while talking. When the experiment was completed, the masks were collected and replaced with new ones. Each collected mask was placed in a sterile zipper bag and sent to the laboratory.
Final sample selection
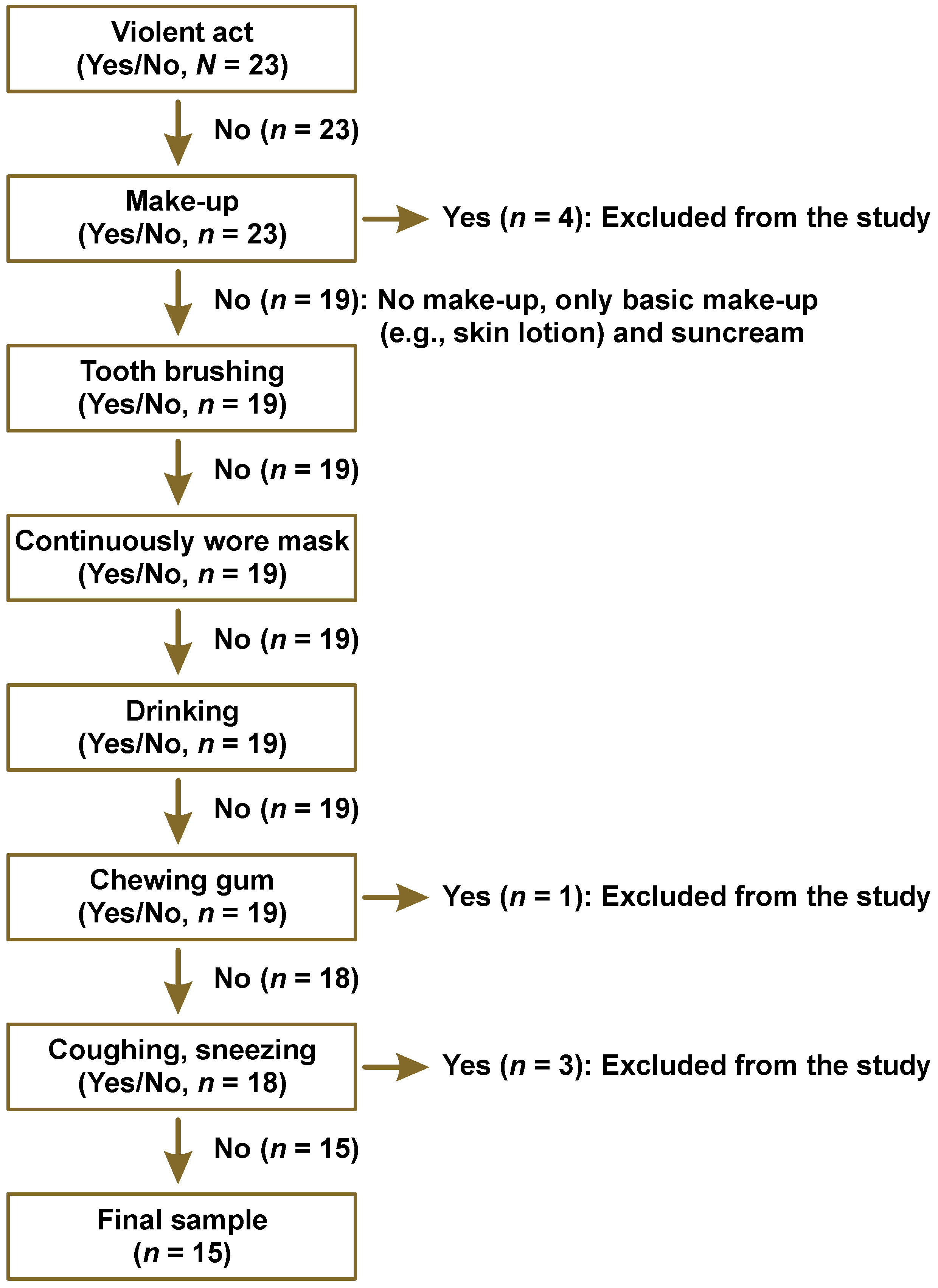
The final sample size (n = 15; mean age: 23.3 ±0.7 years) to be considered for the study was determined based on the survey of the clinicians participating in the experiment (Figure 1). The following cases were excluded: having make-up before wearing the mask (n = 4); chewing gum during the experiment (n = 1); and coughing or sneezing during the experiment (n = 3).
Measurement of general characteristics
The food, beverage and cigarette consumption habits as well as the oral hygiene habits of the participants were surveyed in Study I and Study II (Table 3, Table 4).
Dental history taking
Both in Study I and Study II, all participants underwent the intraoral examination. Sterile dental mirrors, explorers and tweezers were used at a chair unit. In order to prevent infection, fresh gloves and masks were worn for each examined participant. For the sake of data consistency, the examination was conducted by a single investigator.
For saliva sample collection, the participants were asked to brush their teeth; they were then asked to sit straight in a comfortable chair and their saliva was collected into 50-milliliter conical tubes for a duration of 5 min. After that, the initial saliva pH was measured using a pH meter (PH-200; HM Digital, Redondo Beach, USA). The stimulated saliva secretion rate and the saliva buffering capacity were measured using the saliva-check buffer kit (GC, Tokyo, Japan). Thereafter, the participants were given a chewing gum; after chewing for 30 s, the saliva secreted for a duration of 5 min was collected into a measuring cup to measure the amount of saliva. The collected saliva was dropped onto the tester with the use of a pipette and a change in color was identified; based on this, the buffering capacity test was performed. Color change determination was conducted by 3 independent investigators and an average was calculated (Table 3, Table 4).
Colony-forming unit (CFU) measurement
The square shape drawn on the mask was cut out and the inner layer was separated using a tweezer. The separated pieces were placed in an Eppendorf tube containing 700 µL of the Luria–Bertani (LB) broth, vortexed for 1 min and incubated for 24 h at 37°C. After dilution (10−1–10−7), 100 µL was placed onto brain heart infusion (BHI) agar plates. After overnight incubation at 37°C, the number of colony-forming units (CFU) was calculated.
Bacterial identification
Bacterial identification was conducted using a mask worn for 2 h. The masks were directly imprinted for 5 s on BHI agar plates. After incubation for 24 h at 37°C, the colonies were picked randomly and the 16S rDNA sequencing was performed. To amplify 16S rDNA, 2 μL of DNA template and 2 μL of the paired primer set (forward primer – 27F: AGA GTT TGA TCM TGG CTC AG; reverse primer – 1492R: GGT TAC CTT GTT ACG ACT TC) were mixed with a polymerase chain reaction (PCR) kit (IP-Taq™ PCR Premix, LaboPass™; Cosmo Genetech, Seoul, South Korea). The reaction mixtures were subjected to 30 cycles of denaturation and annealing at 50°C in an automated thermal cycler (SimpliAmp™, Applied Biosystems/Thermo Fisher Scientific, Beverly, USA). After PCR, the PCR products were resolved by electrophoresis on 1% agarose gel containing the ethidium bromide (EtBr) solution. The final PCR products were purified using the LaboPass DNA Purification Kit (Cosmo Genetech). Finally, the PCR products were analyzed with the automated sequencing, using the BigDye™ Terminator v. 3.1 Cycle Sequencing Kit (Applied Biosystems), the ABI 3730XL sequencing machine (Applied Biosystems) and a sequencing analysis program (Sequencher™, v. 5.2.4; Gene Codes Corporation, Ann Arbor, USA). The newly aligned 16S rDNA sequences were compared with the bacterial genes deposited in the GenBank® database (National Center for Biotechnology Information (NCBI), Bethesda, USA)14 and the bacterial strains with 99% matches were searched using the Basic Local Alignment Search Tool (BLAST) for nucleotides (NCBI).
Statistical analysis
The SPSS Statistics for Windows, v. 12.0 (SPSS Inc., Chicago, USA), was used for all statistical analyses. The data was evaluated by means of the one-way analysis of variance (ANOVA), followed by the paired t test. The results of all experiments are presented as mean ± standard deviation (M ±SD). The statistical significance was set at p < 0.01 and p < 0.05.
Results
According to the surveys for general characteristics, most of the subjects preferred food of a soft type (Study I: 75.0%; Study II: 80.0%). The amount of water and beverages consumed per day varied with the subjects. None of the subjects in Study II smoked. On average, the subjects brushed their teeth approx. 3 times a day. The preferred toothbrush hair type also varied. The used toothbrushes were replaced every 2–3 weeks (Study I: 16.7%; Study II: 20.0%), every 2–3 months (Study I: 83.3%; Study II: 73.3%), or every 6 months or less often (Study II: 6.7%). Of the total number of subjects, 16.7% in Study I and 53.3% in Study II used dental floss on a daily basis (Table 1, Table 2).
The intraoral examination was conducted to check the oral health status. Specific intraoral clinical findings, such as gingival bleeding, swelling and recession, were not observed in any of the subjects. In Study I, 66.7% had resin fillings, 33.3% had amalgam fillings, 25.0% had gold inlays, and 8.3% had gold crowns. In Study II, 46.7% had sealants, 73.3% had resin fillings, 13.3% had amalgam fillings, and 40.0% had gold inlays. However, no participants had progressive dental caries. The initial saliva pH (Study I: 7.0 ±0.3; Study II: 6.9 ±0.3), the stimulated saliva secretion rate (Study I: 6.9 ±1.6 mL/5 min; Study II: 6.7 ±3.6 mL/5 min) and the saliva buffering capacity (Study I: 10.3 ±0.5; Study II: 9.9 ±1.3) were normal. The saliva secretion and buffering capacity indicated a healthy status (Table 3, Table 4).
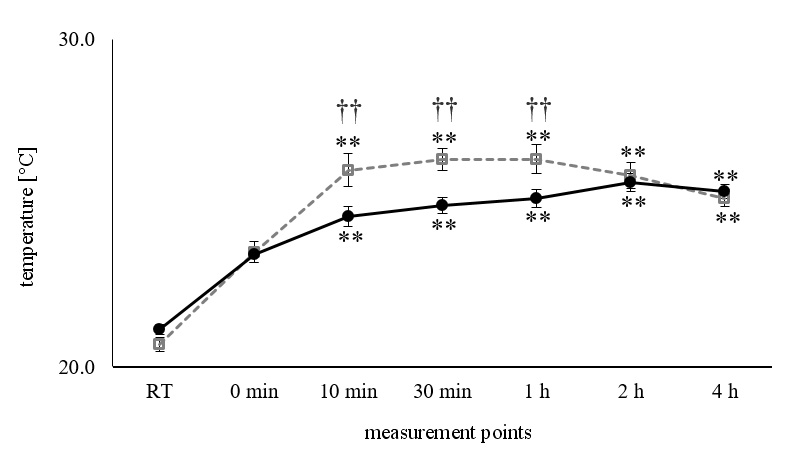
Upon wearing the mask, the temperature inside the mask increased significantly relative to room temperature (p < 0.01). Moreover, the temperature increased even more after 10 min of wearing the mask (p < 0.01), and then it remained constant. After 10 min, 30 min and 1 h of wearing the mask, there were significant differences between Study I and Study II; the average temperature in the mask was higher in Study I than in Study II (p < 0.01). There were no differences in the temperature in the mask between Study I and Study II after 2 h (Figure 2).
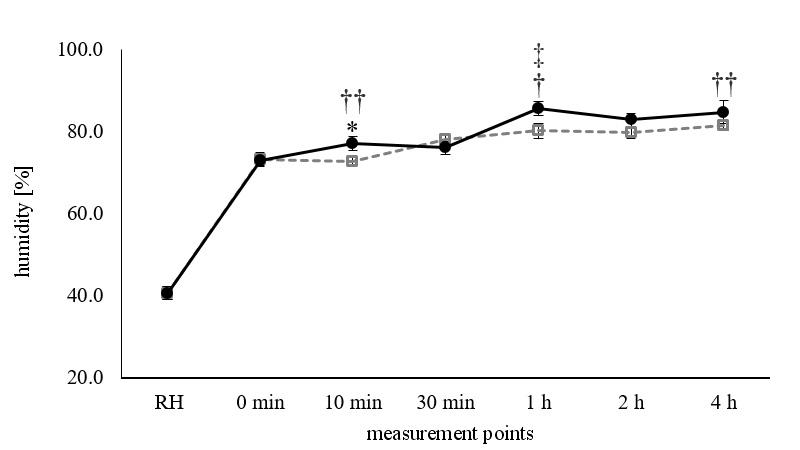
Upon wearing the mask, the humidity inside the mask increased significantly relative to room humidity (p < 0.01). In Study I, the increased humidity remained constant up to 4 h. In Study II, the humidity increased even more after 10 min of wearing the mask (p < 0.05) and was maintained for 30 min. However, there was a significant difference between the humidity values at 10 min and 1 h in Study II (p < 0.01). Thereafter, the humidity remained constant up to 4 h. There were significant differences in the humidity values between Study I and Study II at 10 min (p < 0.01), 1 h (p < 0.05) and 4 h (p < 0.01) (Figure 3).
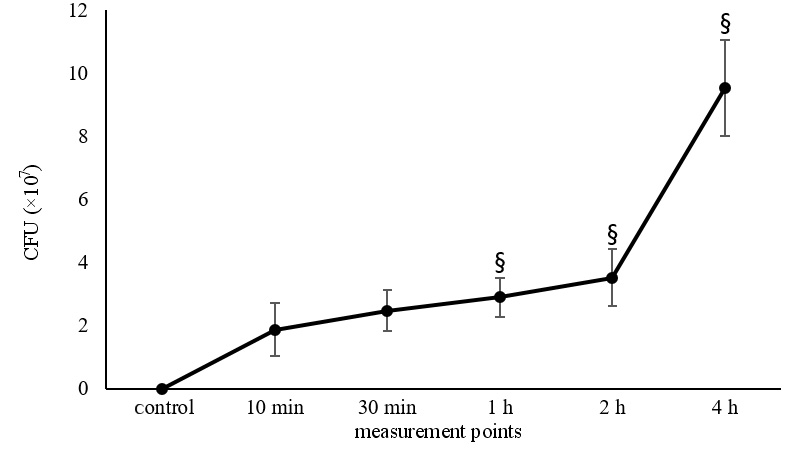
No bacteria were found in the unused mask sample (control), which was sterilized, enclosed in a zipper bag and returned to the laboratory for examination. Bacteria were found in all the masks worn for more than 10 min and the CFU values increased with the mask-wearing time. The CFU values increased up to 30 min, but there was no major difference at 30 min as compared to 10 min (p = 0.055). However, there were significant differences at 1 h, 2 h and 4 h as compared to 10 min (p < 0.01). Significant differences were found after 4 h in comparison with control and other measurement points (10 min, 30 min, 1 h, and 2 h) (Figure 4).
The bacteria identified in the mask used for 2 h are presented in Table 5. The species were classified in the genera Staphylococcus, Bacillus and Roseomonas.
Discussion
In this study, we selected masks based on the data from previous studies. Dental masks are used most frequently in dental clinics, but according to previous studies, aerosol penetration is significantly higher in dental masks as compared to others.3 Therefore, dental masks were excluded from our study. Furthermore, the filtering capacity of surgical masks was weaker than expected, and thus inappropriate for selection3, 5, 10; therefore, surgical masks were also excluded. In another study, it was reported that an N95 mask was more uncomfortable than a surgical mask; consequently, participants more frequently touched their mask to move it for comfort (N95: 25 times; a surgical mask: 8 times).15 Such inconvenience makes it difficult to wear the mask properly, thus increasing its cross-contamination by hands.16 Therefore, KF-AD masks were finally selected and used in the experiments, since they were better than surgical masks in terms of filtration and more comfortable than the conventional N95 masks.
None of the participants consumed liquids during the experiment and continuously wore masks, which might be due to the COVID-19 pandemic. In addition, participants who chewed gum, coughed or sneezed while wearing the mask were excluded from the study to avoid ambiguous results (Figure 1). One study found that particles in saliva from healthy subjects ranged from 0.09 to 3 µm in size; their concentrations ranged from 100 to 350 particles/L during normal breathing, and from 150 to 2,000 particles/L during talking or coughing.17 Another study showed the concentrations of particles ranging from 14 to more than 3,000 particles/L and an average particle size of 0.32 µm.18
It has been reported that upon wearing a mask, the facial and lip temperatures can increase by 5°C and 7.5°C, respectively.19 In addition, the oral temperature increases after 30 min of wearing a mask.20 Based on these results, we hypothesized that the increased temperature when wearing masks affects bacterial growth and mask contamination. Therefore, we evaluated changes in temperature and bacterial growth with the mask-wearing time.
When comparing the temperature before and after wearing the KF-AD mask, it increased by 2.8°C and 2.3°C in Study I and Study II, respectively. Then, the increased temperature was maintained (Figure 2). It was confirmed that if the mask was worn correctly, the temperature could significantly increase immediately after wearing the mask. Interestingly, the temperature was considerably higher in Study I than in Study II at 10 min, 30 min and 1 h (Figure 2), which could be due to the air circulation inside the mask caused by conversation,15 and warm air may have leaked from the inside of the mask to the outside. There was no further temperature increase when the mask was worn for more than 2 h. If increasing and maintaining the temperature significantly affects bacterial growth, the maximum time of using a mask should be considered as 2 h.
Humidity significantly increased immediately after wearing the mask and was maintained up to 4 h (Figure 3). This might be due to the moisture trapped from the mouth during breathing and talking. Bacteria can actively grow when a certain amount of humidity is maintained as opposed to dry environments.21 Therefore, a shorter mask-wearing time will be better for an individual’s health.
The number of CFU on the inside of the mask increased with the mask-wearing time (Figure 4). Although only a small part was cut off and tested, approx. 1.9 × 107 CFU of bacteria were found at 10 min. It is expected that the bacterial count will be high in the entire mask. After wearing the mask, 2.5 × 107, 2.9 × 107, 3.5 × 107, and 9.5 × 107 CFU of bacteria were found at 30 min, 1 h, 2 h, and 4 h, respectively. These results also indicate that a shorter mask-wearing time should be recommended.
In 230 surgical masks, more bacteria and fungi were detected outside than inside the mask and they were strongly correlated with the air pollution level in the working environment.8 A total of 240 masks worn by 130 clinicians during dental treatment for up to 30 min also showed more bacteria on the outside than on the inside.6 However, in the masks from 4 surgeons, the number of bacteria was considerably higher on the inside than on the outside.4 This could be due to the environment in the operating room, where internal pollution is efficiently managed and the entry of many people, including medical staff and patients, is strictly prohibited.4 After an average of 44 min of aerosol-generating dental treatment, bacteria were detected in the face shield of the dentist carrying out the procedure, with the highest levels of contamination in the inner corner of the eyes and the lateral ala.22 This might be due to the dentist being positioned close to the patient and to the characteristics of dental treatment. The abovementioned studies suggest that the contamination of PPE can be greatly affected not only by human sources, but also by the surrounding environment. In this study, bacterial contamination outside the mask was not monitored; thus, it was impossible to compare the CFU of bacteria inside and outside the mask. Data on bacterial changes and the working environment of the clinician providing the sample should be obtained in future studies to establish a correlation.
The 16S rDNA sequencing was performed to identify the bacterial species. The detected bacteria were classified in the genera Staphylococcus, Bacillus and Roseomonas.
Staphylococcus epidermidis (S. epidermidis) is a gram-positive, facultative anaerobic bacterium; it is part of the normal human flora, typically the skin flora, and less commonly the mucosal flora. Staphylococcus epidermidis is not usually pathogenic and infections are generally hospital-acquired.23
Roseomonas mucosa (R. mucosa) is a gram-negative coccobacillus and an opportunistic pathogen that has rarely been reported in human infections. Research on R. mucosa has not progressed much; thus, further studies on bacterial infection pathways with the use of masks are necessary.24
Bacillus cereus (B. cereus) is a gram-positive, motile, rod-shaped, spore-forming, beta-hemolytic facultative anaerobic bacterium commonly found in soil and food. Some strains are harmful to humans and cause foodborne illnesses, while other strains can be beneficial as probiotics for animals.25
Autoclaving can reduce the effectiveness of mask filters; thus, UV sterilization was selected for the sterilization of masks prior to the experiment. However, no bacteria were found at the initial time point of 0 min, before using the masks, and the masks may have been contaminated with bacteria through an unexpected route after use. This result suggests that there is a possibility of mask contamination by pathogenic bacteria through unexpected sources.
In previous studies, various microorganisms, such as bacteria (including staphylococci5, 6, 7 and bacilli7), viruses9 and fungi,6 have been detected in masks. The present results confirm that a variety of microorganisms can be found in the contaminated masks. In another study, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was detected outside the surgical masks worn by the patients infected with the virus.10 Thus, it important to note that there is a possibility of the pathogenic microorganisms derived from human sources leaking outside the mask, even if you wear a mask.
Due to different individual health conditions and immune characteristics, the same type of microorganisms can cause diverse problems, such as opportunistic or secondary infections. Thus, it is important to prevent the infections caused by the contaminated masks through increasing the frequency of mask replacement.
Limitations
This study has the following limitations: it was conducted using only one type of mask; anaerobic bacteria were not considered in this experiment; and the respiratory rate and the frequency of conversation at work varied among the participants. Furthermore, the individual skin conditions, such as acne, that could affect bacterial contamination, were not examined.
Conclusions
Based on the results of this study, the following conclusions can be drawn:
– when the mask was worn correctly, the temperature inside the mask significantly increased immediately after wearing the mask; there was no further temperature increase when the mask was worn for more than 2 h. If increasing and maintaining the temperature significantly affects bacterial growth, 2 h should be considered the maximum time of using a mask;
– humidity significantly increased immediately after wearing the mask and was maintained thereafter. Considering a constant humidity as one of the essential factors for bacterial growth, a shorter mask-wearing time is preferable for an individual’s health;
– the number of CFU on the inside of the mask increased with the mask-wearing time. These results further confirm that a shorter mask-wearing time is beneficial for health;
– bacteria belonging to the genera Staphylococcus, Bacillus and Roseomonas were detected in the used mask.
The frequency of mask replacement can vary, depending on the number of patients encountered and the working environment; regular mask replacement will help in infection control.
Ethics approval and consent to participate
This study was approved by the Ethics Committee of Ulsan College, South Korea (No. 1044363-A-2021-001). Informed written consent was obtained from the participants prior to the experiments.
Data availability
All data generated and/or analyzed during this study is included in this published article.
Consent for publication
Not applicable.