Abstract
This systematic review was designed to evaluate and compare successful cases of regenerative endodontic treatment (RET) in terms of etiology, diagnosis, treatment protocols, and signs of success. An electronic search was performed in the PubMed and Google Scholar databases. The search was completed by 2 independent reviewers following the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines. All in vivo studies in humans that reported at least 1 successful case of RET were included in this review. Successful RET cases were defined as any case that involved the absence of clinical signs/symptoms of periapical inflammation and the presence of continued root maturation, especially apical closure, after the completion of the initial RET. A total of 250 successful cases of RET from 18 studies were selected in this review. A total of 98 (39%) successful cases were detected at least 2.5 years after the initiation of RET. A total of 239 (96%) successful RET cases were presented with the healing/absence of periapical lesions, and no further treatment was required. Furthermore, 45% of the successful RET cases showed root development maturation (stage V). Finally, the clinical outcomes of these RET cases are presented in this systematic review. Prudent case selection and excellent operative protocols are considered to be essential to achieve successful RET outcomes. Future studies are needed to identify a variety of relevant data, including preoperative, intraoperative and postoperative factors, in order to provide a better understanding of successful cases after RET.
Keywords: endodontic regeneration, immature necrotic teeth, outcome assessment, systematic review
Introduction
Regenerative endodontics has been suggested as the appropriate treatment approach for immature, necrotic-pulp permanent teeth cases. Most clinical regenerative endodontic treatment (RET) cases reported in the literature have presented promising clinical results.1, 2 Radiographic evidence of periapical healing and the lack of clinical signs and symptoms have been recognized as the primary indicators of successful RET.3 Also, increased root wall thickness and/or length of the immature root, similarly as recovering the vitality of the tooth, have been recognized as additional goals of RET and are associated with a high rate of success.3 Current endodontic regeneration is frequently referred to as “revascularization”. This means cleaning the root canal with the use of an antibiotic mixture and irritating the root apex tissue to create a blood clot inside the root canal that works as a natural scaffold, and to assist pulp–dentin stem cell proliferation and differentiation.4, 5, 6
Conventional endodontic therapy includes the disinfection, debridement, and subsequent obturation of the root canal system with biologically based materials to replace the function of the organ and the live tissue within the diseased system as an important objective of regeneration in the body.4, 7, 8 Regenerative endodontics or “regeneration” (the previous terminology also included “revascularization”) consists in performing biologically based procedures to replace the necrotic tissue and create a new tooth structure.4 Additional benefits of achieving this goal are continued root development and/or apical closure (root end development), and ultimately, avoiding “traditional” root canal therapy. For regeneration, the available cells of the body are invigorated to regrow the missing tissue. Stem cells, tissue scaffolds, growth factors, and other ingredients that can be introduced into the root canal system are beneficial adjuncts for the regeneration of the pulp and further development of the roots.4, 8, 9, 10, 11
After the redefinition of RET in its new concept, evidence-based clinical outcomes have been extracted from case reports/series with favorable outcomes. However, the main apprehension related to this level of evidence is that it may not factually represent the true results of RET, considering that unfavorable outcomes are underreported in most cases. In the last 5 years, numerous prospective and retrospective clinical studies linked to RET have been published in the literature.1, 2, 12, 13 These types of studies contribute to a higher level of evidence related to successful RET outcomes and present a relatively more accurate depiction of successful RET cases. One review study from 2018 concluded that a successful regenerative procedure was achieved by the regeneration of the pulp with root end closure as well as the healing/absence of periapical pathology, and no further treatment being required.14 However, if signs or symptoms of disease or necrosis of the new pulp/pulp-like tissue occur, any additional apical closure from the regenerative endodontic procedure can promote a more predictable outcome, should root canal therapy later be required. Thus, even “unsuccessful” regeneration can still be beneficial, as any progress from the initial immature-apex state must be acknowledged as a victory.2, 14
Previous clinical studies and case reports have revealed positive clinical results of the regenerative therapy of immature necrotic permanent teeth.5, 15, 16, 17, 18, 19, 20, 21, 22 Managing RET cases requires good treatment planning, and awareness to determine multiple challenges and to prevent any complications that may occur. The presence of an already compromised tooth with necrotic pulp and an open apex represents a major challenge. Other challenges regard the signs and symptoms of healing periapical lesions which occurred after a successful attempt at RET, such as root maturation and/or the resolution of apical infection. To date, a few available review studies from among the peer-reviewed literature have focused on the success rates of different RET cases without covering most of the different factors influencing RET outcomes associated with successful cases.23, 24, 25 Therefore, the present systematic review aimed to systematically collect, compare and evaluate all successful cases of RET mentioned in the literature. It involved highlighting the etiology for the initiation of RET in these cases, the initial diagnosis of successful cases, the treatment protocols used in these cases, the signs of success, and the time needed to successfully treat immature necrotic teeth.
Material and methods
This study was conducted by 2 independent reviewers following the Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA) guidelines.26
Research question
According to the PRISMA guidelines, the following research question was framed:
“Can successful clinical regenerative endodontic treatment cases be used as strong evidence and a promising future approach in the field of endodontic treatment to treat patients with immature necrotic pulp teeth?”
Information sources
An electronic search for articles published in the English language in the years 2015–2020 was performed using the PubMed and Google Scholar databases.
Literature search strategy
The literature search strategy was carried out in July 2020. The search was performed following the PRISMA guidelines, using 2 electronic databases – PubMed and Google Scholar. The electronic search used the Medical Subject Headings (MeSH) terms, which were combined with the Boolean operators (“AND” and “OR”). The following keywords were used: ‘immature teeth’ OR ‘immature tooth’ OR ‘immature dentition’ AND ‘pulp revascularization’ OR ‘pulpal regeneration’ OR ‘pulp revitalization’ OR ‘root canal revascularization’ OR ‘root maturation’ OR ‘regenerative endodontic’ OR ‘regenerative endodontic therapy’ OR ‘regenerative endodontic treatment’ OR ‘regenerative endodontic procedure’ AND ‘blood clot’ OR ‘platelet-rich fibrin’ OR ‘platelet-rich plasma’ AND ‘calcified barrier’ OR ‘apical closure’ OR ‘root end formation’ OR ‘root apex closure’. The detailed description of the search strategy is outlined in Table 1.
This systematic review used the available full-text articles that illustrated the relevant searching of PubMed and Google Scholar. Other databases, such as Scopus, CINAHL (EBSCOhost), Web of Science, and ProQuest Dissertations & Theses (PQDT), were not included in the search strategy, since both the PubMed and Google Scholar databases expand beyond International Scientific Indexing (ISI)-listed journals to include additional scholarly sources, such as non-ISI journals and non-indexed articles that may not be shown in specific databases like Scopus, CINAHL (EBSCOhost) or Web of Science.
The following inclusion criteria were applied to determine which articles would be accepted for the study:
– all in vivo studies in humans in which RET was performed;
– studies published in the English language;
– studies published between 2015 and 2020;
– studies that reported at least 1 successful case of RET.
Due to the lack of consensus in the literature as to defining successful outcomes of RET, the success of RET was defined in the present systematic review as any case of RET that included significant root development maturation as well as the healing/absence of periapical pathology, and no further treatment being required.
Articles that met any of the following criteria were excluded:
– review articles;
– in vitro studies;
– editorial, thesis and personal opinion articles;
– articles that did not report any successful RET cases;
– articles that illustrated clinical relevance about RET by means of percentages and samples taken from non-human sources.
Critical appraisal
Both reviewers independently screened the titles and abstracts of the retrieved articles according to the eligibility criteria as well as the PRISMA guidelines. Any disagreement was resolved through discussion among the 2 reviewers until consensus was reached.
Data extraction
The studies were initially selected by reading their respective titles and abstracts. Subsequently, the full texts of the selected articles were analyzed and organized into standardized Microsoft Office Excel worksheets by both reviewers on an independent basis. The following variables were considered: title; abstract; material and methods; type of publication; and main results.
Data items
Data items from the studies was collected and organized into a table with the following information: author and year, study design, number of successful cases, age and gender of the patients with regard to successful cases, tooth type, etiology, diagnosis, treatment protocol used (i.e., irrigation, intracanal medicaments and the inclusion of any specific scaffold), number of visits needed to finish the treatment, time elapsed between finishing RET and the reported success, signs of success, and root development stage (Cvek’s classification).
Assessment of the risk of bias
of the included studies
The assessment of the risk of bias was performed using the criteria suggested in the Cochrane Handbook for Systematic Reviews of Interventions (Version 5.1.0).27 The Cochrane Collaboration recommends a specific tool for assessing the risk of bias in each included study. The 2 review authors determined the risk of bias of the included studies during the process of data extraction. The risk of bias assessment tool includes 7 specific domains: random sequence generation; allocation concealment; blinding of participants and personnel; blinding of outcome assessment; incomplete outcome data; selective reporting; and other bias.
Each domain was assessed as ‘low risk’, ‘unclear risk’ or ‘high risk’. The overall risk of bias associated with each study was evaluated as follows:
– low risk of bias: all domains were assessed as ‘low risk’;
– unclear risk of bias: at least 1 domain was assessed as ‘unclear risk’;
– high risk of bias: at least 1 domain was assessed as ‘high risk’.
Synthesis of the results
As mentioned above, tables were prepared with the relevant data included as data items.
The following types of outcomes were measured:
– primary outcomes: elimination of clinical symptoms (pain, swelling and the sinus tract); reduction in radiographic evidence of the presence of apical pathology;
– secondary outcomes: root development, defined as an increase in root length and root wall thickness.
Statistical analysis
Due to the heterogeneity between the included studies, no meta-analysis could be conducted. Therefore, only parametric data involving the age of the patients for all the included studies is provided as mean and standard deviation (M ±SD). The descriptive evaluation of the findings is also shown.
Results
Study selection
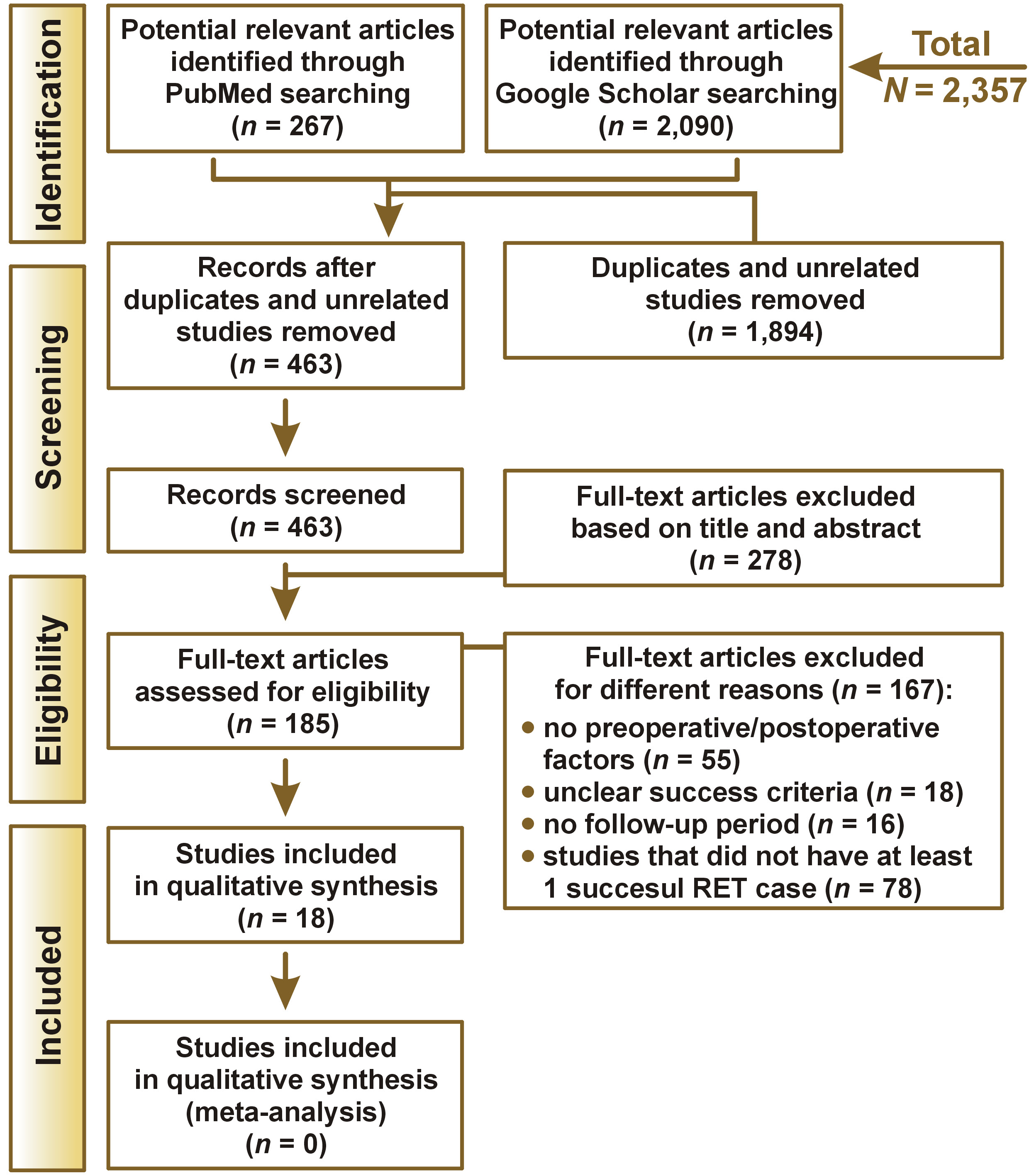
A total of 2,357 studies were initially obtained through the keywords, using the databases. Of those, 1,894 were deleted after reading the title and the abstract, as they displayed either duplicity or an unrelated topic. After applying the inclusion and exclusion criteria, 185 articles were assessed for eligibility. Finally, 18 papers were selected to be included in this review. The flow chart of this systematic review is illustrated in Figure 1.
Study characteristics
The search ultimately included 18 human studies that satisfied both the inclusion and exclusion criteria and had been conducted within the last 6 years. These studies compared the different factors influencing RET outcomes for successful cases. The 18 included studies had a total sample of 250 successful cases of RET.13, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44 The types of studies included in this systematic review were as follows: 7 case reports/case series28, 30, 35, 36, 37, 41, 44; 3 prospective studies33, 39, 43; 5 retrospective studies31, 32, 34, 38, 40; and 3 randomized clinical trials (RCTs).13, 29, 42 The number of successful RET cases ranged from 1 to 45, with the total number of 250. The distribution of these 250 cases was as follows: 10 were extracted from case reports/case series; 74 were identified from prospective studies; 112 were identified from retrospective studies; and 54 cases were identified from RCTs (Table 2). The informative description of all included studies and the different factors influencing RET outcomes for successful cases are summarized in Table Table Table 2 and Table 3.
Primary outcomes
Preoperatively, all of the 250 successful cases of RET included across the 18 studies illustrated pretreatment radiographic evidence of periapical pathology.13, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44 Postoperatively, clinical signs indicative of infection (pain, swelling and the sinus tract) were absent from 239 (96%) of the RET cases. There was a trend toward a reduction in the size of periapical pathology early after the initiation of RET (reported at less than 1 year) and the complete absence of periapical pathology after at least 2.5 years (Table 3).
Secondary outcomes
The reported secondary outcomes were variable and included an increase in root length and root wall thickness in 154 (62%) cases. In addition, there was apical closure and complete root development in 112 (45%) cases (Table 3).
Etiology and diagnosis
of successful RET cases
In 97 successful cases, the gender of patients was reported (53 cases in males and 44 cases in females). Gender was not stated in the other 153 cases (Table 2). A total of 110 successful RET cases occurred in anterior teeth and 54 in posterior teeth. The tooth location was not indicated in the other 86 cases (Table 2). The etiology for the initiation of RET was not reported in 124 successful cases. On the other hand, a total of 126 successful RET cases reported the etiology resulting in the initiation of RET. Sixty-two (49%) of these cases were caused by dental trauma, 30 (24%) by dental caries, 29 (23%) by dens evaginatus, 4 (3%) by dens invaginatus, and 1 (0.8%) by dental fracture (Table 2). All successful cases reported a pulpal diagnosis with necrotic pulp, except for 1 case,36 which reported previously initiated therapy. Most of the successful cases that reported a periapical diagnosis had some type of apical pathosis. Only 2 cases reported normal apical tissue, 3 cases were diagnosed with an acute apical abscess, 11 cases reported a diagnosis of a chronic apical abscess, 13 cases were diagnosed with asymptomatic apical periodontitis, and 4 cases were diagnosed with symptomatic apical periodontitis. Also, 64 cases were reported “with apical pathosis” and 144 cases were reported “with or without apical pathosis” in the studies, without specifically identifying the type of apical pathology. Only 9 cases did not report an apical diagnosis (Table 2).
Irrigation protocol used
in successful RET cases
The use of sodium hypochlorite (NaOCl) as the main irrigation solution with a concentration ranging from 1% to 5.25% was reported in 249 (99.6%) successful RET cases, while 1 (0.4%) case30 used 10 mL sterile saline and 20% ethylenediaminetetraacetic acid (EDTA). Nineteen (8%) cases used chlorhexidine (CHX) irrigation with a concentration of 0.12%. A total of 128 (51%) successful cases reported that NaOCl was the only irrigation solution used in the procedure, 102 (41%) of the successful cases used various combinations of NaOCl and EDTA, and 19 (8%) of the successful cases used various combinations of NaOCl, EDTA and CHX. A total of 128 (51%) successful RET cases did not use EDTA in their irrigation protocols (Table 3). The type of intracanal medicament was reported in 249 (99.6%) successful cases, and only 1 (0.4%) case43 did not report the type of intracanal medicament used in the procedure. Calcium hydroxide (Ca(OH)2) was the only intracanal medicament used in 30 (12%) cases, and 2 cases (0.8%) used a combination of an antibiotic and Ca(OH)2. Twenty-six (10%) cases used an antibiotic combination or Ca(OH)2 in their studies, and 191 (76%) successful cases reported that an antibiotic was the only intracanal medicament used in the regenerative endodontic procedure (Table 3). In 15 (6%) cases, RET was finished in a single visit, whereas in 220 (88%) cases, the completion of RET required multiple visits. Only for 15 (6%) successful cases, the number of visits was not reported (Table 3).
Scaffold and capping materials used
in successful RET cases
A total of 214 (86%) successful cases used a blood clot as a scaffold. Thirty-one (12%) successful cases reported the use of platelet-rich plasma (PRP) in the RET protocol and 5 (2%) successful cases reported the use of platelet-rich fibrin (PRF) (Table 3). A total of 186 (74%) successful cases reported that mineral trioxide aggregate (MTA) was the only capping material used in the procedure. Twenty-four (10%) cases used glass-ionomer cement (GIC), 25 (10%) cases used various combinations of capping materials with bioceramic putty or MTA and 15 (6%) cases used resin-modified GIC in their RET (Table 3).
Signs of success and root development stage of successful RET cases
The reported time elapsed between the initiation of RET and the identification of successful cases ranged from 2 months to 8 years (Table 3). Three (1%) successful cases were detected less than 1 year after the initiation of RET, 84 (34%) successful cases were detected immediately after 1 year since the initiation of RET, 38 (15%) successful cases were detected 1.5 years after the initiation of RET, 14 (6%) successful cases were detected 2 years after the initiation of RET, and 98 (39%) successful cases were detected at least 2.5 years after the initiation of RET. Only 13 (5%) successful cases ranged the time of success from 1 year to 8 years, without specifically identifying the time for each case (Table 3). A total of 239 (96%) successful cases reported the healing/absence of different periapical lesions as the main sign of success (Table 3). Due to the instructive radiographic features of Cvek’s classification and the fact that it illustrates clinical outcomes better than other classification schemes,45 Cvek’s classification was used in this review to determine the root maturation stage for all of the successful RET cases. The distribution of root development stages according to Cvek’s classification was as follows: stage V (completed apical closure) was reported as a sign of success in 112 (45%) cases; stage IV was reported in 34 (14%) cases; stage III was reported in 8 (3%) cases; and for 96 (38%) cases, the root development stage was not reported (Table 3).
Assessment of the risk of bias
of the included studies
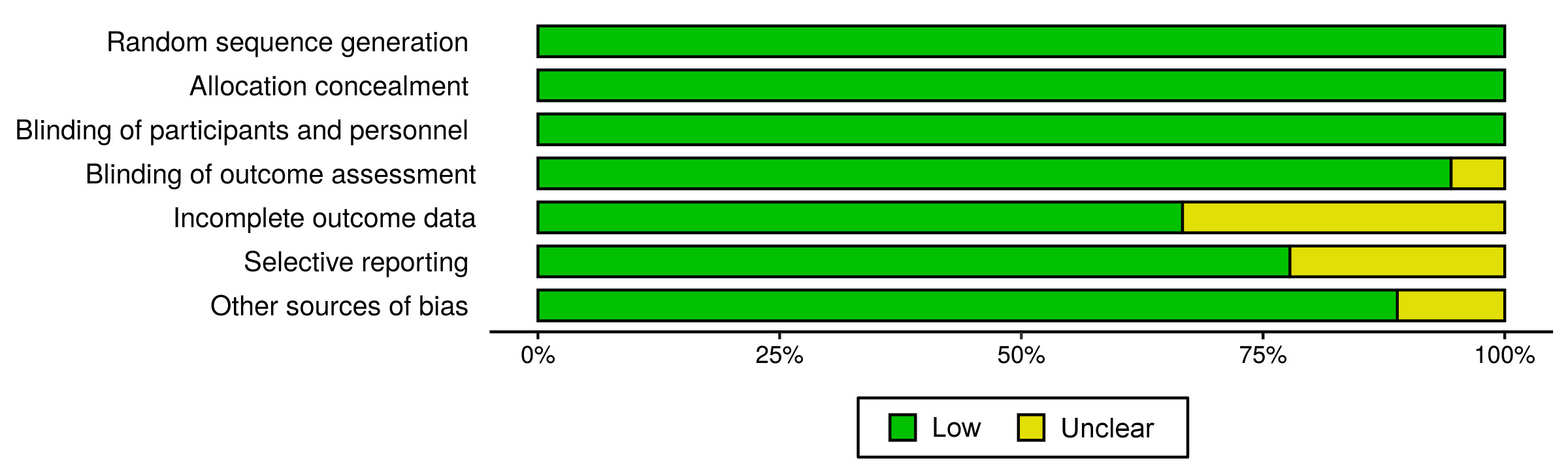
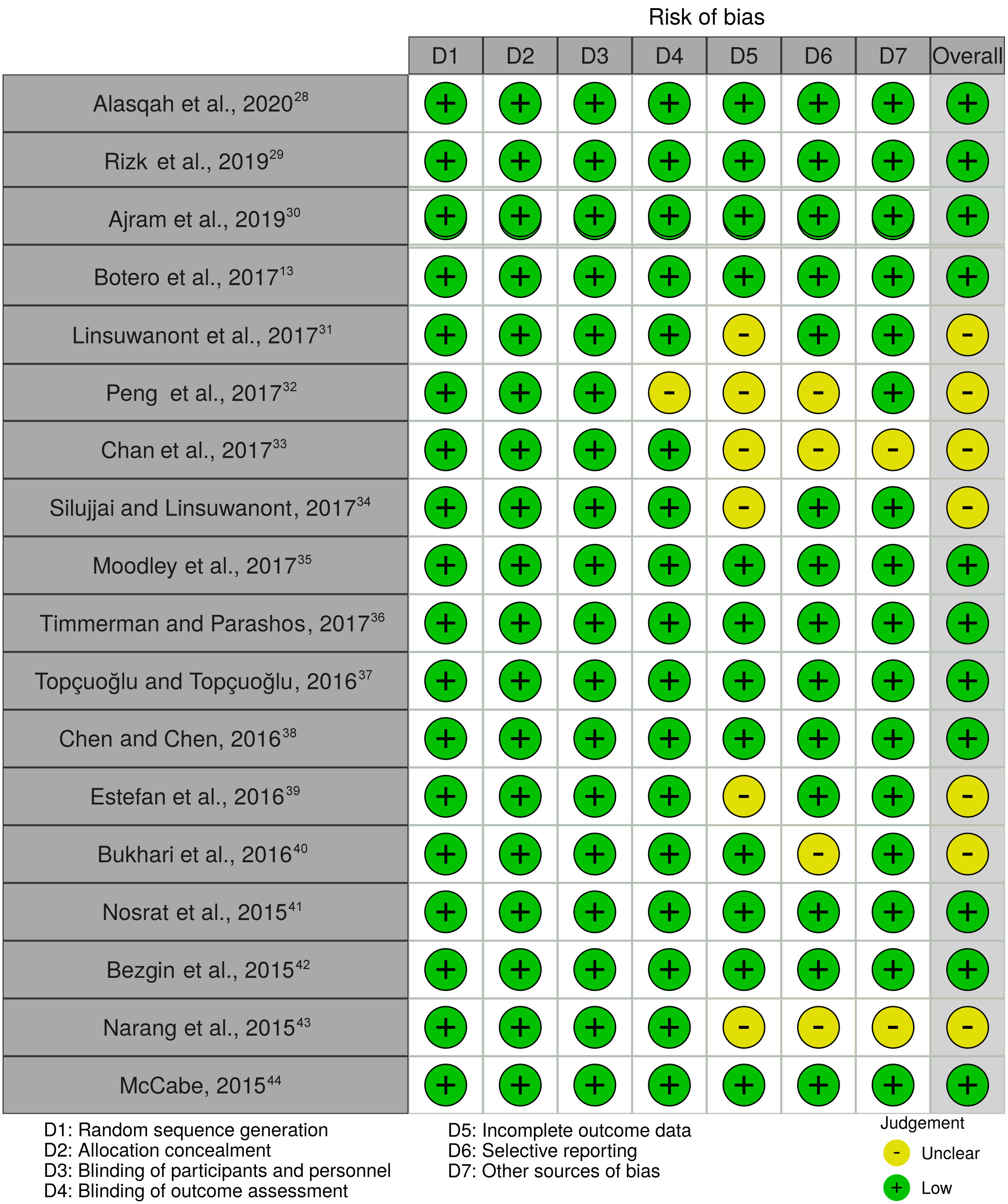
The Cochrane Collaboration’s tool for determining the risk of bias was used for all the studies included in this review.27 The 2 authors integrated the information and summarized the risk of bias associated with the included studies. The majority of studies had a low risk of bias concerning the following domains: blinding of outcome assessment (94%); incomplete outcome data (66%); selective reporting (77%); and other bias (88%). All of the studies presented a low risk of bias (100%) with regard to the random sequence generation, allocation concealment, and blinding of participants and personnel domains (Figure 2). In summary, among the 18 studies assessed for the overall risk of bias, not one study was classified as having a high risk of bias; 11 (61%) studies were considered to have a low risk of bias and 7 (39%) studies had an unclear risk of bias (Figure 3). The scoring of unclear risk of bias was given to 7 studies, as there was not enough information to make a clear judgment concerning the following domains: blinding of outcome assessment; incomplete outcome data; selective reporting; and other bias (Figure 3). A review of the authors’ judgments about each risk of bias domain is presented in Figure 2. Finally, the risk of bias for each study is presented in Figure 3.
Discussion
This systematic review was carried out to summarize and appraise all studies published within the last 6 years that were relevant to our study aim. It gathered all recent clinical studies that investigated the factors influencing RET outcomes for successful cases. This study demonstrates a comprehensive set of evidence extracted from 18 articles that fulfilled our inclusion and exclusion criteria. To date, 2 systematic reviews have discussed the signs of success in different human and animal studies concerning the preoperative factors and postoperative factors in RET (Table 4).24, 25 Alghamdi and Alqurashi concluded in their systematic review that most of the retrieved studies about RET suggested its effectiveness in periapical healing and the formation of apical closure in immature necrotic teeth.25 In addition, Torabinejad et al. demonstrated in their systematic review that the primary goal of RET could be reliably achieved with high probability (91–94% of periapical healing).24 This clearly shows consistency in the conclusions drawn by the previously published systematic reviews. In agreement with those findings, 239 (96%) cases in this review showed the healing/absence of different periapical lesions after RET in human subjects. Also, the 2 abovementioned articles covered the period between 1966 and 2019 (Table 4), while our systematic review covered all eligible articles published within the last 6 years (Table 2 and Table 3).
In our systematic review, most of the successful cases mentioned the etiology for the initiation of RET (Table 2). Dental trauma accounted for 49% of these cases as the main etiology for the initiation of RET, followed by the existence of dental caries (24%) and dens evaginatus (23%). These outcomes are in agreement with a previously published review, which found that the etiology of 30% of all cases treated with RET was dental trauma, followed by the presence of dens evaginatus (22%).46 However, for the majority of successful RET cases, the type of traumatic injury was not reported.46 One clinical study concluded that there were significantly better outcomes for RET cases with an etiology of dens evaginatus as compared to dental trauma.2 The current systematic review found that the healing/absence of periapical lesions was the main presentation of RET success in 96% of cases, as one of the signs of RET success (Table 3). In addition to other signs of success for these RET cases (Table 3), apical closure formation is the secondary goal of RET and the second sign of success in 45% of successful RET cases (Table 3) in comparison with other traditional treatment options for the management of immature necrotic teeth, including periapical surgery and apexification.
Other publications point out that maintaining a high level of disinfection intra/postoperatively in RET is important to enhance RET outcomes.2, 47, 48, 49, 50 Antibiotic medicaments and high-concentration irrigation solutions are recommended to improve the irrigation protocols during RET, since NaOCl,51 CHX,52 and antibiotic intracanal medicaments53 have concentration-dependent antibacterial effects that contribute to reducing different biofilms produced by endodontic pathogens. However, the main irrigation predicament in RET is that lower concentrations of various intracanal medicaments and irrigation solutions are advised to preserve the survival of stem cells from apical papillae.54, 55, 56, 57 Thus, different irrigation approaches should be examined in an endeavor to reach lower concentrations of antibacterial irrigations and medicaments that can still maintain a high level of irrigation.
In our systematic review, most of the successful RET cases had a follow-up period ranging from 2 months to 8 years. In contrast, there is a previous review that retrieved 18 successful cases with RET and reported the history of pulp necrosis no longer than half a year.58 Also, in the present study, the time elapsed between the initiation of RET and the recognition of successful RET was exactly 1 year in 34% of successful RET cases. Furthermore, 39% of all the included successful RET cases were identified at least 2.5 years after the initiation of RET. Some of the successful RET cases reported evidence of initial favorable outcomes, such as the resolution of radiographic lesions,34, 35, 41 apical closure,35, 41 and an increase in root length and root thickness.34, 35, 41 Several case reports and retrospective clinical studies in the literature have reported a high success rate for RET after a maximum follow-up period of 12–19 months.1, 2, 12, 42, 59 In one of the systematic reviews, they calculated the average follow-up time of RET studies to be 16.7 months.24
In our systematic review, 15 successful RET cases were completed in a single visit with different intracanal medicaments used.13, 37, 41, 44 These results are in agreement with a previously published case report, in which RET was performed in a single visit and was reported to be successful.60 A total of 74% of successful RET cases reported the use of MTA as the main capping material in their studies. Other studies used different capping materials, including GIC (10% of cases) and resin-modified GIC (6% of cases). A comparative systematic review found that the pooled success rates for MTA apical plugs and RET were 94.6% and 91.3%, respectively.24
In summary, this systematic review was developed based on the comparison of the impact of the preoperative and postoperative factors on eventual treatment success in RET (Table 2 and Table 3). Some studies used radiographic evidence of completed apical closure and the healing of periapical lesions to define the successful outcomes of RET cases. There is heterogeneity in the RET protocols used to manage the cases reported in this review. Thus, following the updated evidence-based clinical considerations from the American Association of Endodontists (AAE), it is compulsory to reduce variability in RET protocols.57 Finally, it can be concluded that RET can be a useful tool in the field of endodontics along with other approaches in treating children and young adult patients with immature necrotic teeth. The successful clinical RET cases discussed in this review can be considered as high-level evidence in the field of endodontics with regard to patients with immature necrotic-pulp teeth. Based on the present evidence, it seems that the treatment of immature teeth with pulp necrosis by means of RET provides high survival and success rates.
Study strengths and limitations
This study summarized and appraised all peer-reviewed studies published within the last 6 years that fulfilled both our inclusion and exclusion criteria. To our knowledge, this is the only systematic review that covered the topic of the different factors influencing RET outcomes for successful cases in depth. The systematic reviews conducted by Alghamdi and Alqurashi25 and Torabinejad et al.24 covered the periods of 2009–2019 and 1966–2016, respectively (Table 4). Our review used PubMed and Google Scholar as search engines. One advantage of using Google Scholar is that it ensures that reviewers do not miss any relevant research published in journals that are still not cited in PubMed. Unfortunately, due to the heterogeneity of the influencing factors in the existing human studies, we were restricted to performing a systematic review without a meta-analysis. Finally, although studies conducted on human subjects were part of the inclusion criteria, we unfortunately could find but a few published successful case studies that used RET to treat children and young adult patients with immature necrotic teeth.
Conclusions
Several RET cases of immature necrotic teeth were reported in this review. These cases provide clinical outcomes, such as apical closure formation, the healing of different forms of apical pathology as well as a significant follow-up duration. Thus, prudent case selection and excellent operative protocols are considered to be essential to achieve the successful outcomes of the RET procedure. Collectively, this systematic review showed that the healing/absence of periapical pathology was the main measure of success in 96% of successful RET cases. Furthermore, 45% of successful RET cases presented with root development maturation Stage V, and 39% of successful RET cases were identified at least 2.5 years after the initiation of RET. Future studies should describe a variety of relevant data, including preoperative, intraoperative and postoperative factors, to provide a better understanding of successful cases after RET.