Abstract
Background. Coronavirus disease 2019 (COVID-19) continues to affect dental emergency services worldwide. Dental anxiety (DA) is described as a common and distressing problem in terms of oral health maintenance.
Objectives. The present study aimed to evaluate DA levels as well as the COVID-19 fear and perception of control (COVID-19 FPC) in patients attending dental emergency clinics during the COVID-19 pandemic.
Material and methods. Sociodemographic, dental and medical data was obtained from the participants. A face-to-face questionnaire with questions referring to the reasons for the emergency dental visit, the visual pain scale, the Modified Dental Anxiety Scale (MDAS), and the COVID-19 Fear and Perception of Control Scale (COVID-19 FPCS) as well as additional questions concerning bruxism and a previous diagnosis of anxiety/panic attacks or depression was administered. The χ2 test was used to analyze the data.
Results. A total of 1,439 patients were included in the study. The most common reason for the dental visit was pain (47.5%). The prevalence of DA was 5.1% (74/1,439). A significant association was found between DA and gender (p = 0.020). The incidence of severe pain was higher in patients with DA than in those without DA (p = 0.002). No significant differences in the MDAS scores were found between patients with and without a chronic disease (p = 0.804), with regard to the educational status (p = 0.364), or between the age groups (p = 0.600). The prevalence of a ‘strongly agree’ response to all questions in COVID-19 FPCS was higher in patients with DA as compared to those without DA.
Conclusions. Females and patients with severe pain were more likely to exhibit DA. In general, patients with DA strongly agreed with the statements of COVID-19 FPCS, which may indicate a correlation between the 2 scales.
Keywords: SARS-CoV-2, dental care, visual pain scale, coronavirus, Turkey, fear
Introduction
Fear is one of the emotions people often experience. It is a sudden involuntary behavior, an emotional reaction to a real or perceived threat.1 Anxiety can be defined as a mood of uncertainty, a discomfort that can turn into panic or fear. Anxiety may lead to various physiological and behavioral disorders in individuals.2
One specific type of fear is that of the dentist, namely dentophobia, which occurs with the concern that dental treatment involves terrible experiences. If the fear of the dentist turns into anxiety, then patients may overreact during treatment. Moreover, this situation may cause patients to postpone their treatment, cancel appointments or attend follow-ups irregularly.3 Dental fear and anxiety may develop during the appointment process, during the waiting period before treatment, and in relation to the dental instruments used and/or the procedures performed during treatment. The stimuli that typically cause the greatest fear and anxiety include seeing a dental injector, the injection procedure itself and the use of an aerator.4 Fear and anxiety behaviors are considered as subjective reactions to pain.5 On the other hand, anxiety can turn the pain into an unbearable feeling. Thus, it is necessary to understand the association between pain and anxiety. To meet this need, a scale was developed to measure dental anxiety (DA) in individuals. The Dental Anxiety Scale (DAS), which was created in 1978, serves this purpose.6 In 2000, it was modified by adding the ‘injection’ criteria and called the Modified Dental Anxiety Scale (MDAS).7 Today, MDAS is commonly used in research.8, 9, 10, 11 The prevalence of dental fear and anxiety across populations varies due to different measurement methods and patient groups. In the Turkish population, the prevalence has been found to be 21.3–23.5%.12
A novel type of coronavirus infection – coronavirus disease 2019 (COVID-19), which was first identified in Wuhan, China, in December 2019 and spread over the world – was declared a pandemic by the World Health Organization (WHO) in March 2020, with the first case detected in Turkey on March 11, 2020.13 Societal fear, concern and anxiety levels increased at this time due to the uncertainty associated with the occurrence of the first case. The disease is transmitted through saliva, nasal drops, physical contact between individuals, and contact with contaminated surfaces.14, 15
The bacterial and viral infection of patients and physicians has been a long-standing problem in dental clinics. However, with the COVID-19 pandemic, this problem has become a considerable danger.16 In dental clinics, which belong to areas of the highest risk of the transmission and spread of the disease, the management of this problem has been attempted with the highest precaution and care, without suspending urgent healthcare services.
The characteristic difference between infectious diseases and other disorders is the presence of fear in the population. Fear is directly related to the infectiousness, severity and mortality risk of the disease.17, 18 Excessive fear can prevent people from thinking clearly and reasonably in their reactions to COVID-19. The current mitigation techniques for COVID-19 across the world are mainly focused on the control of the spread of the infection, the development of effective vaccines and the improvement of treatment. The psychosocial effects of the disease have not yet been adequately investigated.
If infection prevention protocols are not followed during dental treatment, then dental clinics can become a major source of the spread of COVID-19. Due to the high risk of contamination, non-urgent dental procedures have been temporarily postponed. Hence, it is of great importance to determine the incidence of dental visits, the reasons for visits and the amount of pain perceived by patients during the pandemic. Furthermore, changes in DA and fear levels in patients should be analyzed.
In this regard, the obtained data would enable us to understand the measures to be taken and the strategies to be followed during the pandemic, and to determine the profiles of dental clinic patients. The present study aimed to evaluate DA levels, and the COVID-19 fear and perception of control (FPC) in patients attending dental emergency clinics, and to assess the reasons for dental visits during the pandemic.
Material and methods
Following permission from the Turkish Ministry of Health (decision No. GO 20/547), the ethical approval of the study was obtained from the Clinical Research Ethics Committee at the Faculty of Medicine of Hacettepe University, Ankara, Turkey. This study was performed in compliance with the ethical principles of the Declaration of Helsinki, using the face-to-face interview method. Patients aged 18 years or older who reported to the Department of Dentomaxillofacial Radiology between June 2020 and September 2020 for emergency dental treatment, and who could speak, read and write in Turkish were included in this study. Written informed consent was obtained from all participants. Patients who did not give consent to participate were not included in the study. Incomplete questionnaire forms (i.e., unfilled or partially filled forms) was the sole exclusion criterion.
Sociodemographic, dental and medical data was obtained from the patients, and the assessment of pain levels was made using the visual pain scale. The patients were asked to rate their pain with a value between 1 and 10, while the participants without pain marked the option ‘I have no pain’. The assessment criteria were as follows: ‘no pain’ – 0 points; ‘worst pain imaginable’ – 10 points. The classification for pain severity considered scores <3 as mild pain, scores 3–6 as moderate pain, and scores >6 as severe pain.19 In addition, the patients were asked about bruxism and a previous diagnosis of anxiety/panic attacks or depression. The reasons for the emergency dental visit were also recorded.
In the 2nd part of the questionnaire, a form including queries about COVID-19 FCP, generated by the authors, and the MDAS7 form were administered. The validity and reliability of the Turkish version of MDAS had been previously examined by Ilgüy et al.11 The scale consists of 5 questions. The minimum possible score for each question is 1 and the maximum score is 5. The adopted cut-off score on the scale was 19, and the participants who scored 19 or higher were considered to have high DA levels. In addition to these queries, the participants were asked to respond to the question “How do you feel about reporting to the dental clinic during the COVID-19 pandemic?” The COVID-19 Fear and Perception of Control Scale (COVID-19 FCPS) was generated after a detailed literature review.20, 21 It was mandatory to answer all of the questions in the questionnaire.
Statistical analysis
Frequency values expressed as number (n) and percentage (%) were used as descriptive statistics for the categorical variables. Pearson’s χ2 test was used to search for differences in terms of categorical variables, including demographic characteristics, and the medical and dental data. When the test result was statistically significant, pairwise comparisons were made using the appropriate χ2 test with the Bonferroni correction.
The internal consistency of MDAS and COVID-19 FCPS was assessed via Cronbach’s alpha. The internal consistency coefficient for MDAS was 88.3% and for COVID-19 FCPS it was 92.1%. Since there is no Turkish study on the validity and reliability of COVID-19 FCPS, each item was considered separately within the scope of this study, and the total score could not be obtained. The analyses were performed using Microsoft Word, v. 16.0 (Microsoft Corporation, Redmond, USA) and the IBM SPSS Statistics for Windows software, v. 23.0 (IBM Corp., Armonk, USA). The significance level was set at 0.05.
Results
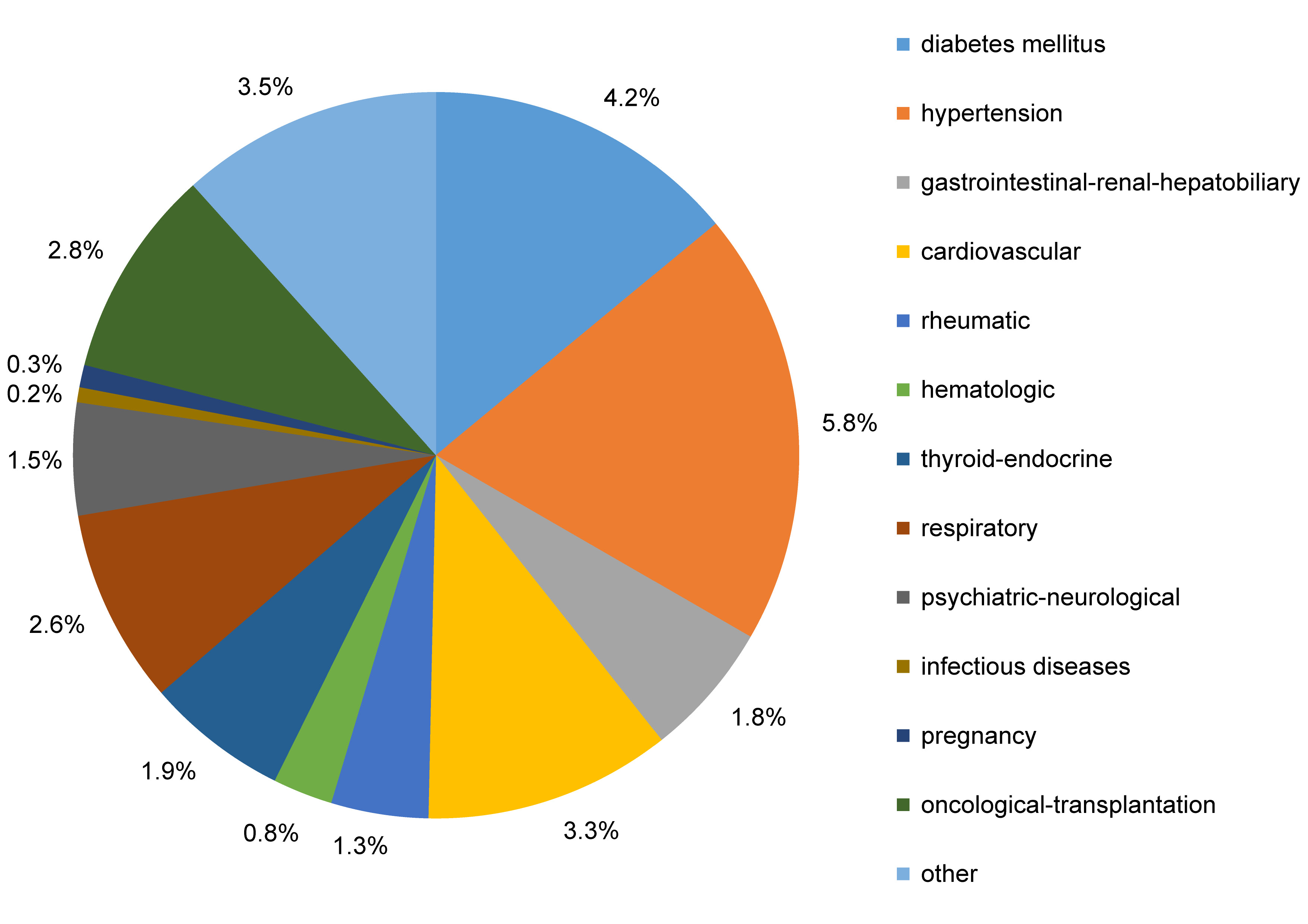
Overall, 1,644 patients attended the emergency clinic at the Department of Dentomaxillofacial Radiology within the chosen time period. Out of these, 205 patients decided not to participate in the study, and a total of 1,439 patients (595 males and 844 females) were included. The age of the patients ranged between 18 and 68 years, with a mean age of 34.8 ±14.2 years. The demographic characteristics of the sample are presented in Table 1. A total of 333 patients (23.1%) had 1 or more chronic diseases or other systemic conditions (Table 1). Hypertension (n = 83; 5.8%) was the most common disease followed by diabetes mellitus (n = 61; 4.2%) (Figure 1).
Previous diagnoses of anxiety/panic attacks or depression were more prevalent among females (n = 92; 10.9%) than males (n = 42; 7.1%) (p = 0.014). However, the prevalence rates were similar among the age groups (p = 0.365). Almost half of the patients with a previous diagnosis of anxiety/panic attacks or depression (65/134) reported an increase of varying degree in their symptoms during the pandemic.
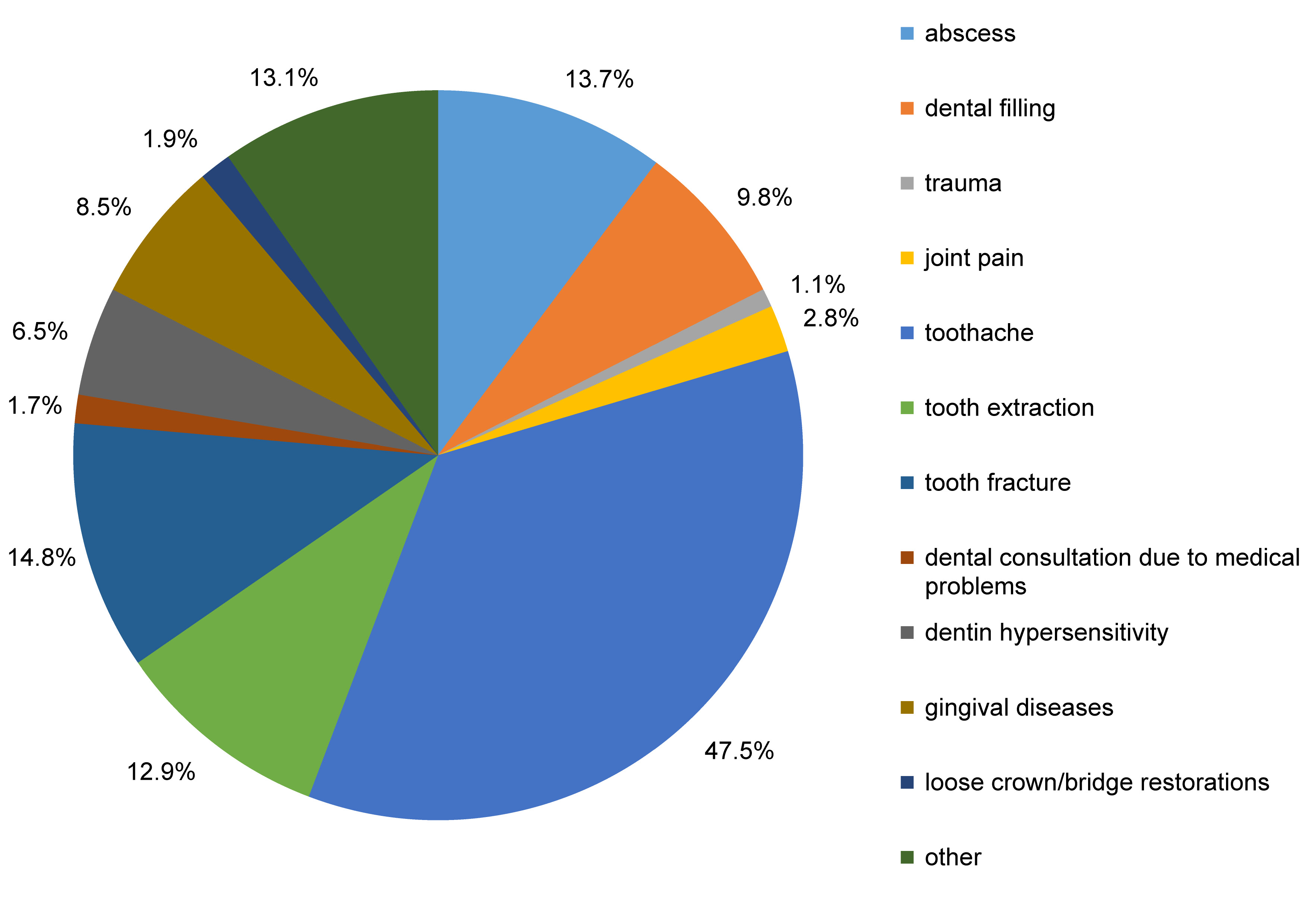
One thousand and ninety-one patients (75.8%) stated that they reported to the dentist due to a complaint, with 214 (14.9%) visiting occasionally and 134 (9.3%) visiting regularly. The most common reasons for the emergency dental visit were toothache (47.5%) followed by tooth fracture (14.8%), abscess (13.7%) and tooth extraction (12.9%) (Figure 2). Based on the scores obtained from the visual pain scale, more than half of the patients (n = 738; 51.3%) presented with severe pain, 364 (25.3%) with moderate pain, 77 (5.4%) with mild pain, and 260 (18.1%) with no pain.
The MDAS scores showed that 74 patients (5.1%) exhibited DA (MDAS ≥ 19). Dental anxiety was more common among females, the patients with severe pain, and those who felt very anxious or extremely anxious about visiting a dental clinic during the COVID-19 pandemic (p = 0.020, p = 0.002 and p < 0.001, respectively) (Table 2). No significant differences in DA were observed between the age groups, with regard to the educational status, and between patients with or without a chronic disease (p = 0.600, p = 0.364 and p = 0.804, respectively) (Table 2).
In total, 417 patients complained of bruxism. The reported bruxism was more common in females, the patients with a previous diagnosis of anxiety/panic attacks or depression, and the patients with higher MDAS scores (p < 0.001, p < 0.001 and p = 0.047, respectively) (Table 3). An association between the educational status and bruxism was also found (p = 0.010).
The analysis of COVID-19 FCPS showed that the prevalence of a ‘strongly agree’ response to all questions was higher in patients with DA as compared to those without DA (p < 0.001) (Table 4).
Discussion
The present study was mainly designed to determine the reasons for attending dental emergency clinics during the COVID-19 pandemic, and to assess DA levels, as measured with MDAS, with regard to the sociodemographic characteristics and COVID-19 FCP of the patients, with the latter measured with COVID-19 FCPS.
The majority of the patients in this study had irregular dental care habits, as they reported to the dental clinic only due to a complaint. Most of them presented with severe pain and the primary reason for seeking emergency care was toothache. These results confirm that pain relief is by far the main reason for attending dental emergency clinics.22, 23, 24 The prevalence of DA in the present study (5.1%) was slightly lower than in previous studies (8–11.6%), as measured by means of MDAS (cut-off score ≥19).8, 9, 10, 11 Based on the present findings, DA was more common in females, which is in accordance with the results of previous research.25, 26, 27, 28, 29, 30 In a previous study, it was stated that females exhibited higher levels of anxiety, because, in comparison with males, they perceived outbreaks as more dangerous.31 Therefore, performing the present study during the COVID-19 pandemic may also have resulted in higher DA levels in females. However, there have also been studies that did not found any association between gender and DA.32, 33, 34, 35, 36
Our results showing no significant association between age and DA are also consistent with previous reports.25, 32, 36 This finding might be attributed to the fact that older patients may report to the emergency clinics less often, as they may have fewer or no teeth.32 Another possible reason may be the restrictions imposed on patients aged 55 years or older, such as a national lockdown, as in this study. However, conflicting results have also been reported.7, 37, 38, 39 Consistent with several previous reports,32, 33, 36, 38, 39, 40, 41 no association was found between the educational status and the MDAS scores in the present study. This might be due to the small number of patients with higher educational levels in the study group.32 However, there are also other reports in the literature that present different results.28, 42, 43 A possible explanation for these latter observations is that a high educational level may be associated with better oral health and regular dental check-ups, which may support a decrease in DA as the educational level increases.43
The present study found an association between the reported bruxism and the MDAS scores, consistent with the results of previous studies.44, 45, 46 This might be due to the fact that bruxism is a reflection of the individual’s response to stress in the oral cavity.44 It has also been suggested that the pain experiences of individuals may impact their DA levels.27 In the present study, an association was established between severe pain and DA, a finding consistent with the literature.47, 48 We found responses of ‘very anxious’ and ‘extremely anxious’, related to the respondents’ feelings about visiting dental clinics during the COVID-19 pandemic, correlated with DA. This result is not surprising, considering the fact that people who encounter such an extraordinary situation for the first time may express emotions such as fear, anxiety or stress. Another reason is that COVID-19 causes not only physical health problems, but also a series of psychosocial disorders.49
The COVID-19 FCPS used in the present study was prepared specifically for the period of the pandemic following a review of the literature. The authors believe that there may be correlations between the scale and MDAS in many aspects. It has been shown that most individuals are afraid of being infected with the virus in crowded environments and transmitting it to their families/relatives.50 Therefore, it may be suggested that being together with other patients in the waiting rooms of dental clinics and the fact that the patient has to remove their mask during treatment/examination may increase the level of anxiety. This may also explain why patients with DA strongly agreed with the statements of COVID-19 FPCS in the present study.
Limitations
This study has some limitations. First, the study was conducted in a dental emergency clinic in Ankara, which may potentially limit the generalizability elsewhere in Turkey, especially in terms of the demographic characteristics of the patient population. Another limitation is that the data presented in this study is self-reported, and partly dependent on the participants’ honesty and recall ability. Thus, the data may be subject to recall bias. The COVID-19 FPCS generated for the present study has not been checked for validity and reliability. Therefore, the items of the scale were analyzed separately. Finally, as a result of the cross-sectional nature of this study, the assessment of DA levels in the patients was made at a single time point.
Conclusions
With the COVID-19 pandemic, the whole world came up against an unexpected danger. Uncertainty regarding the infectiousness and virulence of the virus may have led to changes in the anxiety levels of individuals. The prevalence of DA in the present study was slightly lower as compared to previous reports in the literature. Nevertheless, females and patients with severe pain were found to exhibit increased DA. In general, patients with DA strongly agreed with the statements of COVID-19 FPCS, which may indicate a correlation between the 2 scales.