Abstract
Background. Dental professionals are at great risk of contracting coronavirus disease 2019 (COVID-19).
Objectives. The objectives of this study were to determine the levels of stress and anxiety among dental professionals, and to determine which dental procedures cause the greatest amount of stress and anxiety during the COVID-19 pandemic.
Material and methods. This cross-sectional survey was conducted by requesting voluntary participation of dental healthcare workers through the authors’ own e-form, which consisted of our self-developed questionnaire, the Perceived Stress Scale (PSS) and the Generalized Anxiety Disorder-7 scale (GAD-7). The simple and multiple linear regression analyses were used to assess the effect of dental procedures and other factors associated with stress and anxiety among the participants. A p-value ≤0.05 was considered statistically significant.
Results. This survey included 85 participants (32 males, 53 females) with a mean age of 31.6 ±6.0 years. Significant associations were found between severe stress for scaling (p < 0.001; p < 0.001), complex fillings (p < 0.001; p < 0.001), root canal treatment (RCT) (p = 0.001; p = 0.007), crown and bridge work (p < 0.001; p < 0.001), denture work (p = 0.034; p = 0.001), third molar extractions (p < 0.001; p < 0.001), surgical procedures (p < 0.001; p = 0.001), and implant placement (p = 0.001; p = 0.022) and the PSS and GAD-7 scores, respectively.
Conclusions. Dental healthcare workers exhibit severe stress and anxiety associated with elective dental procedures. Dental emergencies should take precedence and elective dental treatment should be carried out with utmost caution, ensuring all protective measures. Psychological support for dental healthcare professionals should be made accessible.
Keywords: anxiety, stress, psychological, dentistry, COVID-19
Introduction
Coronavirus disease 2019 (COVID-19) is thought to have originated in Wuhan, China, and has spread across the globe. It has infected over 53 million people and killed more than 1.3 million.1 The contagion spreads through both aerosol droplets and contact transmission.2 Patients exhibiting symptoms are the main source of transmission; however, asymptomatic patients and patients in the incubation period of the infection may also transmit the virus.2 Reports on the widespread transmission of COVID-19 to healthcare professionals have made it essential to develop strict safety protocols to protect frontline workers.3, 4
The risk of cross-infection between dental practitioners and patients is extremely high, as dental interventions cause the generation of aerosols. Additionally, dentists and dental auxiliaries work in close proximity to patients.5 As recommended, dentists have implemented exceptional hand hygiene, the use of personal protective equipment (PPE), such as masks, gloves, gowns, goggles, and face shields, and a thorough disinfection of all surfaces in negative pressure rooms.6 Initially, the scheduling of elective procedures was not recommended and only dental emergencies were performed during the pandemic; however, as the duration of the pandemic could not be predicted, elective dental services have also been resumed.7
The pandemic has caused severe distress to all people and patients worldwide. At times like these, there can be a substantial impact of stress and anxiety on our daily lives. Cohen et al. developed the Perceived Stress Scale (PSS) to objectively determine stress in individuals due to life events and how they perceive these events in terms of stress.8 Additionally, Spitzer et al. introduced the Generalized Anxiety Disorder-7 scale (GAD-7), providing clinicians with a brief index to determine anxiety in patients.9 The GAD-7 scale is credited with a sensitivity of 89% and a specificity of 82% when using the threshold score of 10. Therefore, this is a highly accurate measure to determine the severity of anxiety symptoms.9
The risk of infection with COVID-19 for healthcare providers has raised stress and anxiety among dental professionals.10, 11 The literature lacks data on the COVID-19 infection rates among dentists; only a few surveys have been conducted, finding less than 1% of dentists affected by the disease.12, 13 These surveys highlight the dentists’ perception of COVID-19 and the precautionary measures taken by them to prevent disease transmission.
Objectives
The objectives of this study were to assess stress and anxiety among general dental practitioners, specialist dental practitioners and dental surgery assistants while treating dental patients during the COVID-19 pandemic, and to determine which dental procedures cause the greatest amount of stress and anxiety.
Methods
This cross-sectional survey was conducted at the Aga Khan University Hospital in Karachi, Pakistan, between July 20th and August 5th, 2020, after obtaining an ethical approval (2020-4997-11263) from the institutional ethics review committee. The sample size was calculated using the one sample mean sample size calculator,14 assuming a sample variance as 25, a margin of error of 5 points, an equivalence limit of 2, with a confidence level (CI) of 95%, and a power of 80%. It was calculated that a minimum of 24 subjects (n) were required in each group with a total sample size of 72 (N).
General dentists, dental specialists and dental assistants were contacted via social media and requested to participate voluntarily in the present study through our e-form drafted in the English language. General dental practitioners were defined as those who have obtained a bachelor’s degree in dental surgery (BDS, 16 years of education). Specialist dental practitioners were those with at least 2 years of postgraduate specialization in any of the dental specialties (orthodontics, oral and maxillofacial surgery, operative dentistry, prosthodontics, periodontics, or pedodontics). Dental surgery assistants were regularly practicing auxiliaries, working in any private or public dental clinic or hospital. Those general dental practitioners, specialist dental practitioners and dental surgery assistants who were not in clinical practice, participants who did not respond despite 5 reminders, and those who provided incomplete responses were excluded.
The general dental practitioners, specialist dental practitioners and dental surgery assistants who met the eligibility criteria were sent the survey form via a Google Docs link. If they failed to return the filled forms, they were sent gentle reminders 5 times over a period of 15 days. Demographic information and the level of stress associated with dental procedures were recorded using a self-developed questionnaire. The level of stress was assessed using PSS.8 Anxiety was assessed by means of GAD-7.9
Statistical analyses
Data was analyzed using the Stata® software, v. 12 (StataCorp, College Station, USA). Frequency and percentages were reported for categorical variables, such as reasons for stress and anxiety among dental professionals, and the amount of stress they experienced with different dental procedures. For continuous variables, the median (Me) and interquartile range (IQR) values were reported. The Shapiro–Wilk test was applied for determining the normality of the data, which showed a non-normal distribution; therefore, we used non-parametric tests. The Mann–Whitney U test was used for comparisons between genders. The comparison of the stress and anxiety Me scores among the 3 groups was performed using the Kruskal–Wallis test. Unadjusted and adjusted β coefficients with their 95% CIs were reported by using the linear regression analysis to determine the dental procedures associated with stress among the participants as well as to adjust the results for confounding factors. A p-value <0.05 was considered statistically significant.
Results
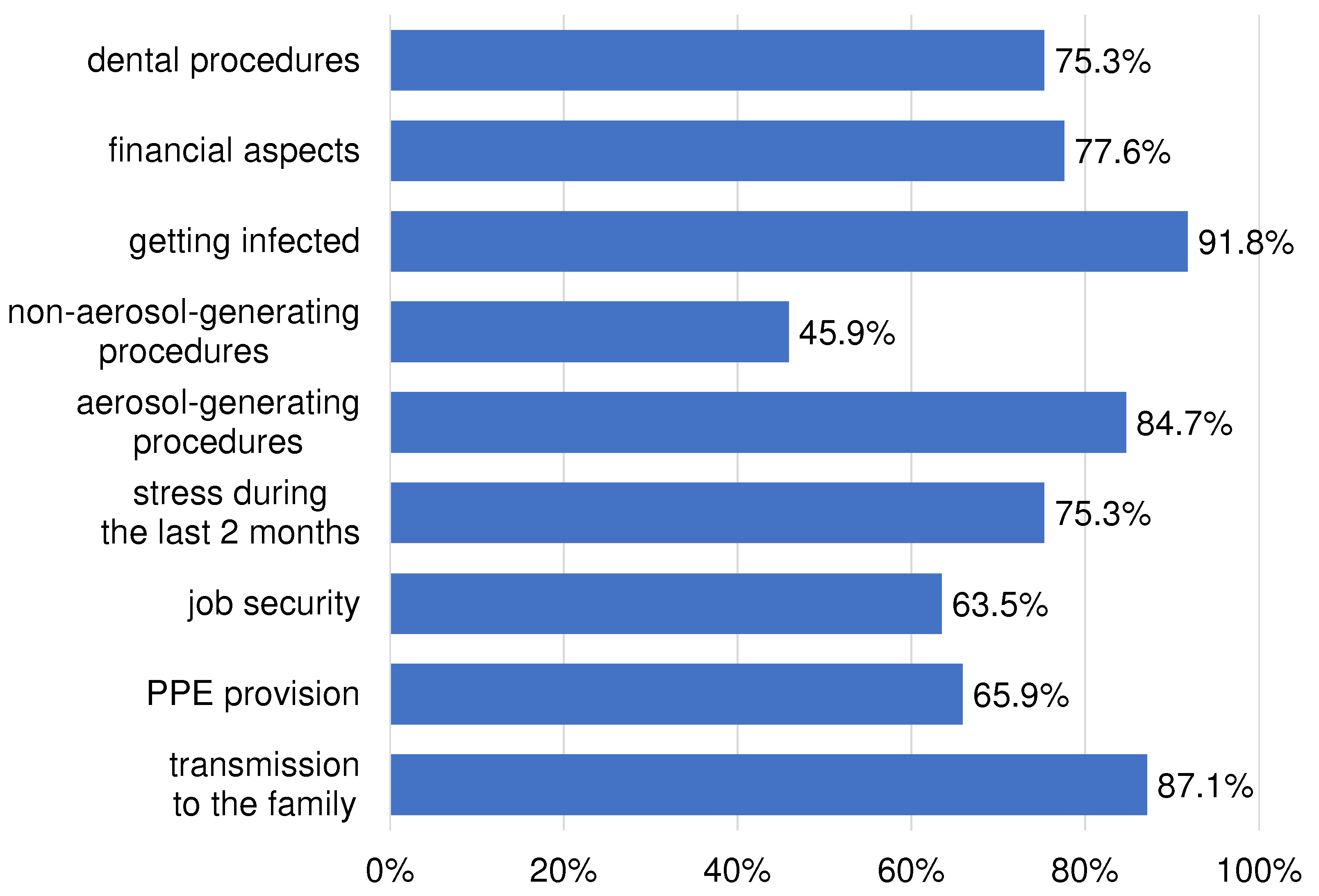
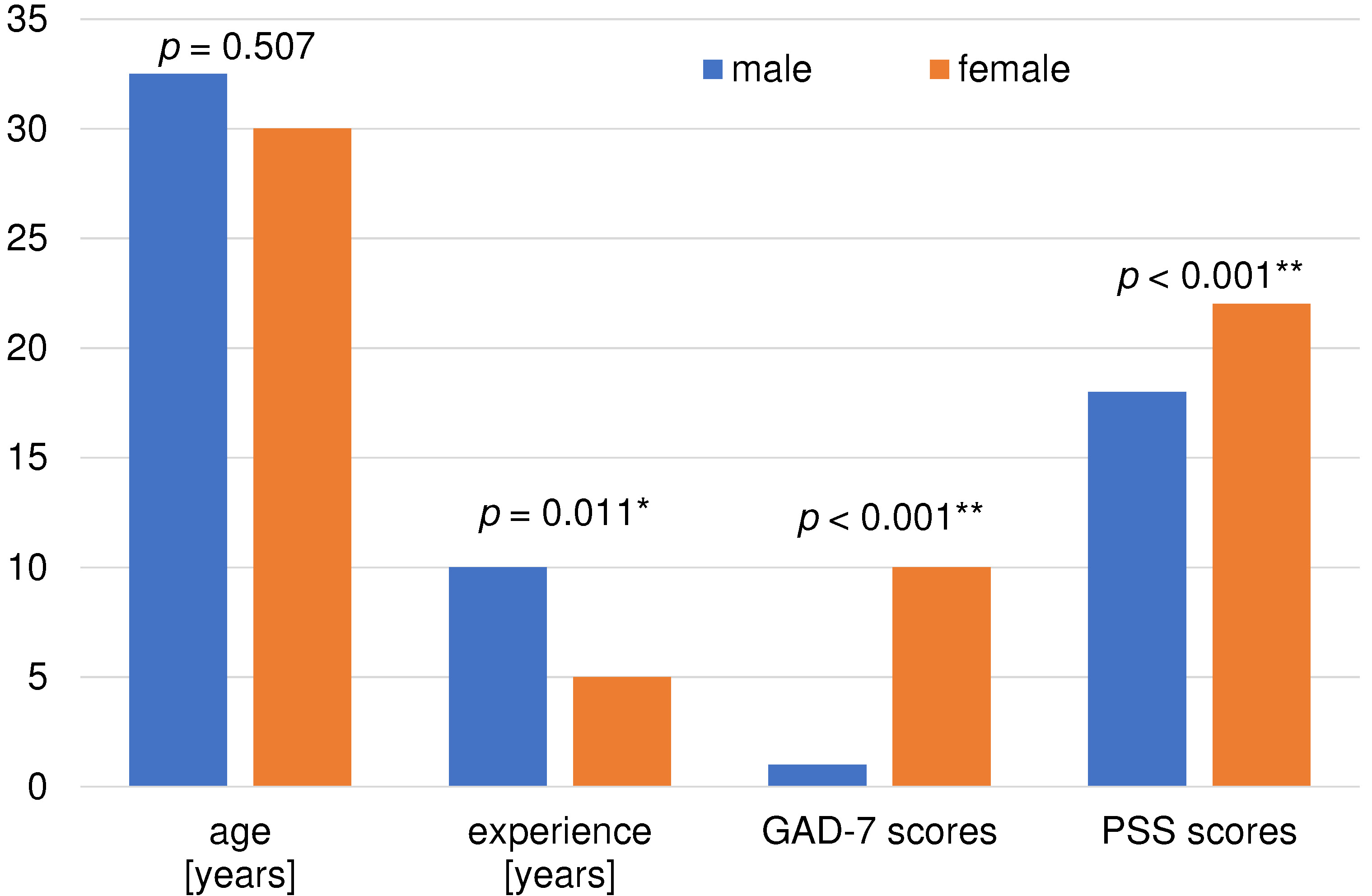
Eighty-five participants (32 males, 53 females) completed our survey and were included in this study. They were of a mean age of 31.6 ±6.0 years. The distribution of dental professionals who participated in the survey was as follows: dental assistants – 28% (18 males, 6 females); general dentists – 29% (4 males, 21 females); maxillofacial surgeons – 8% (2 males, 5 females); operative dentists – 9% (2 males, 6 females); orthodontists – 20% (5 males, 12 females); and prosthodontists – 5% (1 male, 3 females). Figure 1 presents reasons for stress and anxiety among dental healthcare workers. Significant differences were found between genders in the experience (p = 0.011), GAD-7 (p < 0.001) and PSS (p < 0.001) scores (Figure 2). Further comparisons were made after the stratification of data with respect to gender. The comparison of the PSS scores among the 3 male healthcare worker groups showed significant differences (p = 0.021). Also, the comparison of the PSS and GAD-7 scores among the 3 female healthcare worker groups showed significant differences (p = 0.012 and p = 0.037, respectively) (Table 1).
The simple linear regression analysis showed significant associations between the independent variables of age (p = 0.033), female gender (p = 0.001), stress during the last 2 months (p < 0.001), job security (p < 0.001), dental procedures (p < 0.001), aerosol-generating procedures (p < 0.001), and non-aerosol-generating procedures (p < 0.001) and the PSS scores, which reflects significant amounts of stress among dental practitioners during the COVID-19 pandemic. Significant associations were also found between severe stress connected with various dental procedures and the PSS scores, as shown in Table 2.
The simple linear regression analysis found significant associations between age (p = 0.012), female gender (p < 0.001), stress during the last 2 months (p < 0.001), job security (p = 0.001), dental procedures (p < 0.001), aerosol-generating procedures (p < 0.001), and non-aerosol-generating procedures (p < 0.001) and the GAD-7 scores, indicating severe anxiety among dental practitioners. Significant associations were also found between severe stress connected with dental procedures such as scaling (p < 0.001), complex fillings (p < 0.001), root canal treatment (RCT) (p = 0.007), crown and bridge work (p < 0.001), denture work (p = 0.001), third molar extractions (p < 0.001), surgical procedures (p = 0.001), and implant placement (p = 0.022) and the GAD-7 scores (Table 3).
The multiple linear regression analysis showed significant associations between the fear of transmitting the virus to family members (p = 0.002), PPE provision (p = 0.003), job security (p = 0.007), stress during the last 2 months (p = 0.011), and age (p = 0.034) and the PSS scores, with 48% of variance in the PSS scores being explained by these factors (Table 4).
The multiple linear regression analysis showed significant associations between the fear of transmitting the virus to family members (p = 0.048), aerosol-generating procedures (p = 0.016), age (p = 0.002), and stress during the last 2 months (p = 0.006) and the GAD-7 scores, with about 40.5% of variance in the GAD scores being explained by these factors (Table 4).
Discussion
This survey indicates a significant amount of stress and anxiety among dental practitioners associated with treating patients during the COVID-19 pandemic. Dental professionals are at high risk of contracting COVID-19 due to their exposure to saliva, blood and aerosol droplets that are produced during dental procedures.15
The outbreak of COVID-19 caused disruption in dental services and many practices were shut down temporarily. Guidelines such as those by the American Dental Association (ADA) and the Centers for Disease Control and Prevention (CDC) were rapidly developed to help standardize patient care and minimize the spread of the infection.16, 17 These changes prompted investigation into the knowledge and attitude of dentists with regard to providing dental treatment during the pandemic. Khader et al. investigated the awareness and perception of as well as attitude toward COVID-19 among dentists.18 Although the authors found that dentists possessed adequate knowledge about the pathogen, they lacked the understanding of the protective measures which needed to be implemented to prevent disease transmission. A study by Ahmed et al. indicated that 87% of dentists were afraid of acquiring the infection while providing treatment despite being aware of the necessary precautions.19 Similarly, this study shows that although dentists, specialists and dental assistants are well-informed, they fear that they may contract the virus and infect their family members. Greater PSS and GAD-7 scores were reported for the female gender as compared to males. As many female dentists often have domestic duties and are mothers, their concerns related to the risk of transmission of the virus to immediate family members is understandably greater than in the case of male dentists. Significant associations between the stress and anxiety outcomes related to the outbreak of the pandemic and conducting dental procedures with the PSS and GAD-7 scores indicate psychological effects on dental healthcare workers. For example, 43.5% of the participants either did not perform or assist in the scaling of a patient’s dentition during this pandemic. Furthermore, the fear of contracting the disease through the aerosolized droplets produced during dental treatment was reported by 84.7% of the participants. This is in concordance with a study by Gambarini et al.20
Reverse transcription polymerase chain reaction (RT-PCR) tests have been widely conducted for the detection of the COVID-19 infection.21 However, these tests have shown rates of false negative results that range between 2% and 29%, which is equal to 71–98% sensitvity.22 The neglect of COVID-19 protocols in several dental centers around the country has raised fears in dental professionals. These observations may have contributed to the high PSS and GAD-7 scores noted particularly for general dentists in our study. Many dental centers nationally and internationally have adopted preventive measures, such as a pre-procedural mouth rinse with either 0.2% povidone-iodine or 0.5–1% hydrogen peroxide, and yet dentists are hesitant when undertaking routine dental procedures.23, 24 Lower PSS and GAD-7 scores were observed in dental assistants of both genders. This may be due to the lack of education, awareness and knowledge among these individuals.
A great possibility of cross-contamination exists with elective dental procedures.16 Our results show significant associations between scaling, fillings, extractions – both simple and complex, denture work, crown and bridge work, implant placement, and other surgical procedures and the PSS and GAD-7 scores. These procedures pose a greater risk of infection transmission, as dental healthcare workers are exposed to the oral environment for prolonged periods of time and there is a constant production of fine aerosol-containing dental debris and saliva.25 This justifies any apprehension a dental healthcare professional may have toward treatment that can be deferred.
Emergency dental care continues to be provided to patients despite the ongoing pandemic. Protocols have been put into place for the alleviation of pain due to dental disease. The National Health Service (NHS) recommended that all non-urgent dental care be suspended, which included orthodontic treatment.26 As seen in the results of this study, severe stress or anxiety were not significantly associated with orthodontic treatment, most probably due to the nature of orthodontic appointments. Associations between the GAD-7 scores and simple fillings, simple extractions and pediatric procedures were statistically non-significant, unlike in the case of the PSS scores. In contrast, both the PSS and GAD-7 scores showed significant associations with severe stress when performing all other dental procedures. It is possible that this difference in the PSS and GAD-7 scores is due to the perception that simple procedures require a shorter time of exposure to a patient. Nonetheless, the possibility of contracting the virus remains. Furthermore, the pediatric population has shown to be vulnerable and poses a transmission risk. This should remind the dental community to take all the necessary precautions during the treatment of these patients.27
To the best of our knowledge and based on the literature review, there have been no studies assessing stress and anxiety among dental professionals with regard to different dental procedures during the COVID-19 pandemic. The results of this survey provide novel information regarding the inclination of dental healthcare workers to provide routine care during the pandemic. As many dental procedures are not emergencies, the reservations of healthcare workers about providing elective dental care were highlighted. A possible limitation of this online survey could be a sampling error leading to bias in the results. In addition, the number of subjects in the subgroups was small and a greater number of females participated in this study. Nonetheless, based on the present results, we recommend that psychological support and treatment should be made accessible to dental healthcare workers during the COVID-19 pandemic to maintain their mental health. We also suggest studies be conducted that would compare stress and anxiety between other medical professionals and dental healthcare workers as well as methods to reduce the risk of transmission of the virus to dental healthcare workers and patients so that both groups could be safe in these unprecedented times.
Conclusions
Dental practitioners suffer from significant stress and anxiety related to acquiring the infection during the COVID-19 pandemic. There is an escalated fear of getting infected while providing treatment and of transmitting the infection to family members. Dentists should carefully evaluate the dental needs of all patients before undertaking elective dental procedures, whereby all dental emergencies should be handled immediately while adhering to safety guidelines. Psychological support should be provided to dental healthcare professionals to maintain adequate mental health.