Abstract
Background. It is of utmost importance to identify and treat groups susceptible to psychological problems during the coronavirus disease 2019 (COVID-19) pandemic.
Objectives. This study aimed to compare the psychological status between the general population and subjects with orofacial pain (OFP) during the COVID-19 pandemic.
Material and methods. A total of 509 young adults were recruited based on the inclusion and exclusion criteria, using the convenient sampling approach. They were assigned to 2 study groups: group 1 – individuals with OFP; and group 2 – the general population. Their background variables, knowledge, perception, attitude, concerns, and Kessler scale scores were recorded through an online questionnaire. Student’s t test, the χ2 test, Pearson’s correlation coefficient, and one-way analysis of variance (ANOVA) were used for the statistical analysis.
Results. Some of the background variables were significantly different between the study groups (p < 0.05). The knowledge, perception and attitude scores of the respondents were not significantly different between the study groups (p > 0.05). Females exhibited significantly higher adjusted Kessler scores as compared to males (p < 0.05). Group 1 exhibited the highest adjusted Kessler scores (p < 0.05).
Conclusions. Individuals with OFP exhibited higher psychological distress, depressive symptoms and anxiety during the rapid rise of the COVID-19 outbreak, representing a moderate psychological disorder. Females suffered more from psychological distress as compared to males. Therefore, psychological interventions should be focused on this group.
Key words: psychological status, orofacial pain, COVID-19, Kessler scale (K10)
Introduction
The deadly coronavirus disease 2019 (COVID-19) has promptly become a pandemic with its high transmissibility.1, 2 The COVID-19 pandemic has adversely affected the mental health of health professionals, patients and the public, increasing the incidence of psychological crises.3, 4, 5, 6 Symptoms of adverse psychiatric outcomes have become more prevalent in different populations as compared to the era before the pandemic. Currently, varying degrees of the outbreak severity, national economy, government preparedness, the availability of medical supplies/facilities, and a proper dissemination of COVID-related information have led to regional differences in the general public’s psychological health. At the beginning of the outbreak, when individuals were challenged by mandatory quarantine, unexpected unemployment and uncertainty associated with the outbreak, symptoms of adverse psychological outcomes were more commonly observed.7
Conditions in which an examination by the physician puts individuals at risk of contracting coronavirus disease might predispose them to psychological problems.8 One of these conditions is orofacial pain (OFP), with a prevalence of 10–15% in the adult population.9 After back, neck and knee pain, OFP is one of the most common causes of chronic pain.9 Recently, it is comprehensively classified as OFP attributed to dentoalveolar disorders and anatomically related structures, myofascial OFP, temporomandibular joint (TMJ) pain, OFP attributed to the lesions or diseases of the cranial nerves, OFP resembling the presentations of primary headaches, and idiopathic OFP.10 Acute pain in the orofacial area is often tooth-related.9 Chronicity in OFP is defined as pain occurring on more than 15 days per month and lasting for more than 4 hours daily for at least 3 months.10 Chronic OFP is most commonly related to musculoskeletal disorders and temporomandibular disorders (TMDs).9 Temporomandibular disorders is an umbrella term embracing pain and dysfunction that involves the masticatory muscles, TMJ and associated structures.9 Apart from imposing a substantial economic burden on societies,11 persistent OFP exerts a great impact on patients’ quality of life.12 It has been suggested that, both as a confounder and a mediator, psychological distress coexists with chronic pain, and being exposed to pain might exacerbate a depressive state.13 Comorbid psychological distress and psychosocial dysfunction have been observed in people with OFP, especially when the pain is chronic, such as in TMDs.14, 15, 16, 17 A study from 2005 on the presence and impact of post-traumatic stress disorder (PTSD) in a sample of patients seeking OFP treatment suggested that PTSD was prevalent in the OFP setting.18 In the era of the COVID-19 pandemic, patients with OFP might even suffer more from psychological distress, as the disease, the lockdown of cities and the associated sequelae have increased the incidence of psychological crises in the whole world population.3, 4, 5, 6
Psychological factors associated with the pandemic might even lead to a greater risk of developing and perpetuating bruxism and TMDs.19 Also, depressive symptoms can influence the treatment outcome of OFP.13, 20 Therefore, the early identification of the populations in the first stages of a psychological crisis would allow for the efficient implementation of interventional strategies.3 Clinicians would devise appropriate measures, including suggestions for professional psychological consultation and prioritizing the vulnerable patients for treatment. To the best of our knowledge, no study has compared the psychological status of individuals with OFP and the general population under the added psychosocial burden imposed by the COVID-19 pandemic. Therefore, this study aimed to compare the psychological distress, symptoms of depression and anxiety in the general population and individuals suffering from OFP during the COVID-19 pandemic. Moreover, the knowledge, perception, attitude, and concerns were compared between the groups.
Methods
Subjects
The study was conducted in Shiraz, Iran. Individuals aged 19–39 years were recruited in this study. The convenient consecutive sampling approach was used. Individuals with past or current neurologic or psychiatric illnesses or systemic diseases, or any oral and maxillofacial surgeries or orthodontic treatment in their treatment plan were excluded by asking the inviters not to invite them to participate in the study and ensure it with similar questions in the questionnaire. The respondents were divided into 2 groups as follows:
– group 1 – patients suffering from chronic pain in the orofacial region for more than the last 3 months, diagnosed by the clinicians through history, physical examinations and validated pain questionnaires (Brief Pain Inventory, Beck Depression Inventory, Hospital Anxiety and Depression Scale, McGill Pain Questionnaire, and Oral Impact on Daily Performance). The records and documents of the patients, from the date of the announcement of the beginning of the pandemic (March 11, 2020) to April 11, 2020, in 3 pain clinics and 3 dental emergency centers, were searched, and eligible subjects were invited to fill in the questionnaire. The same administrator was introduced to all the patients via a phone call by the clinic. The nature and purpose of the research were explained to the patients by the administrator through the WhatsApp messenger. The patients were allowed to ask the administrator questions via the messenger;
– group 2 – the general population with no diagnosis of OFP. The general population was invited to participate in the study through social media, including Instagram accounts, WhatsApp groups or Telegram channels, with more than 1,000 followers.
Ethical considerations
The protocol of this cross-sectional study was approved by the Ethics Committee of the Vice-Chancellor for Research at Shiraz University of Medical Sciences in Iran (No. IR.SUMS.DENTAL.REC.1399.122). The participants were told about the nature and purpose of the research by 1 administrator. The participants were allowed to ask the administrator questions through the WhatsApp messenger. They were reassured that all their personal data would be kept confidential. Informed consent was obtained from all the participants.
Questionnaire
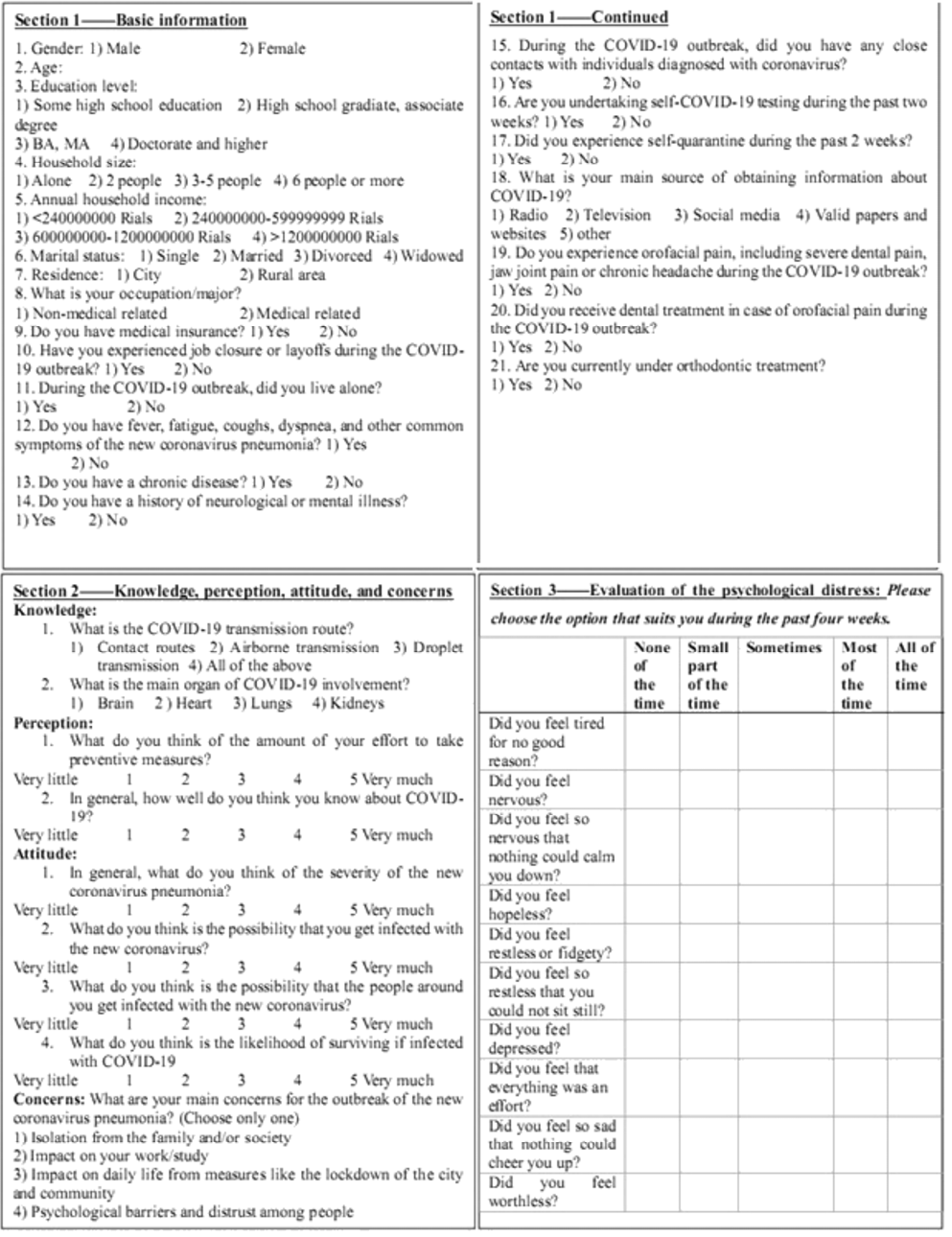
The questionnaire consisted of 3 sections (Figure 1).
The 1st section focused on individual background information and the person’s primary source of information about COVID-19. Questions regarded the current orthodontic treatment, the current OFP and its treatment, and 6 questions related to the probability of catching coronavirus, job closure and quarantine. Questions about the exclusion criteria were also asked in this section.
The 2nd part consisted of 9 questions on knowledge (2 multiple-choice questions), perception (2 questions on a 5-point Likert scale; the higher the total score, the higher perception of the participant), attitude (4 questions on a 5-point Likert scale; the higher the total score, the more negative attitude of the individual), and the main concerns about the influence of the pandemic (a single-choice question and the participants could choose only 1 option) developed by the investigators.
The validity of the 2nd part of the questionnaire was assessed by submitting the questionnaire to 1 professor in each field – orthodontics, public health and internal medicine. The reliability was assessed by asking 20 subjects to complete it twice with a 2-week interval. Cronbach’s α was used as a measure of reliability. All the values were ≥0.8.
The last part of the questionnaire was the Kessler Psychological Distress Scale (K10).21 The reliable and valid Persian version of this scale was available at the beginning of the study.22, 23, 24 There are 10 items (on a 5-point Likert scale) on this scale. The total score was regarded as a continuous variable in this study, with higher scores indicating increased psychological distress. The K10 score is a sensitive screen for diagnosing anxiety and depressive symptoms, with 4 items indicating anxiety (K-anxiety) and 6 items indicating symptoms of depression (K-depression).25, 26 A total score of 10–19 is considered normal, while 20–50 indicates mental distress (20–24: mild disorder; 25–29: moderate disorder; 30–50: severe disorder).27
Data collection
The questionnaires were developed at www.docs.google.com and filled in through an online survey. The questionnaires were available from April 25, 2020 to May 20, 2020; during that period, all routine elective medical and dental procedures were suspended except for emergencies.
The questionnaires with missing data or identical answers in all the K10 questions, or with extreme variations in answers regarding similar questions were excluded.
Statistical analysis
The data was imported to IBM SPSS Statistics for Windows, v. 21.0 (IBM Corp., Armonk, USA). The scores referring to the K10 questions were summed separately to form individual K10 scale, K10-anxiety and K10-depression scores for each respondent. The scores of knowledge, perception and attitude were summed separately to achieve the knowledge scores, the perception scores and the attitude scores, respectively. All the statistical analyses were performed with a two-tailed α significance level of 0.05, and 95% confidence interval (CI) for β and p-value was calculated.
All the background variables except for age were compared between the groups with the use of the χ2 test. Age as well as the knowledge, perception and attitude scores were compared between the 2 groups with Student’s t test. The primary concerns were compared between the groups by means of the χ2 test.
Regardless of the group, the correlation of age and the knowledge, perception and attitude scores with the Kessler scores was determined using Pearson’s correlation test. A comparison of the Kessler scores between various concern choices was evaluated using the one-way analysis of variance (ANOVA) and the post-hoc Šidák test. The Kessler scores were also compared between genders with Student’s t test.
The one-way analysis of covariance (ANCOVA) was conducted to determine differences between the groups in the K10 scale, K-anxiety and K-depression scores, controlling for the possible confounding variables. The percentages of individuals with mental distress were also compared between the groups by means of the χ2 test. Also, in group 2, one-way ANCOVA was used to compare the Kessler scores in the respondents who “sought pain management” and those who did not.
Results
The number of eligible patients in group 1 was 197. Temporomandibular disorders were present in 92 subjects (87 subjects with TMD of muscle origin, 5 subjects with TMD of joint origin). Headache was present in 84 subjects (53 subjects with headache of chronic tension type, 21 with chronic migraine and 10 with chronic daily headache). The remaining eligible 21 subjects had trigeminal neuralgia (15 subjects) and traumatic neuroma (6 subjects). Twenty-seven subjects with OFP did not fill the questionnaire (response rate: 86.3%). Totally, 635 respondents were recruited (group 1 or patients with OFP: n = 170; group 2 or the general population: n = 465). Respondents who met the exclusion criteria, or provided incomplete or mixed data were excluded (126 individuals). Finally, 509 eligible respondents (group 1: n = 112; and group 2: n = 397) underwent the statistical analysis.
Comparison of independent variables between the groups
Table 1 presents the demographic data and the background variables which were compared between the groups. The household income variable was statistically different between the study groups (p = 0.016).
The knowledge, perception and attitude scores of the respondents were not significantly different between the study groups (p > 0.05) (Table 2). The concerns of the respondents were not different between the study groups (p > 0.05). The most often reported main concern for both groups was “impact on work/studies” (Table 2).
Relationship between psychological indices and the respondents’ age, knowledge, perception, attitude, and main concerns, regardless of the group
Age had a weak inverse correlation with the K10 scale (r = −0.118; p = 0.003), K-anxiety (r = −0.114; p = 0.004) and K-depression scores (r = −0.116; p = 0.003).
Attitude had a moderate positive correlation with the K10 scale (r = +0.226; p = 0.0001), K-anxiety (r = +0.215; p = 0.0001) and K-depression scores (r = +0.224; p = 0.0001). Perception had a weak negative correlation with the K10 scale (r = −0.108; p = 0.005), K-anxiety (r = −0.103; p = 0.008) and K-depression scores (r = −0.106; p = 0.006). Knowledge had a weak positive correlation with the K-anxiety score (r = +0.077; p = 0.046), while it was not statistically correlated with the K10 scale and K-depression scores (p > 0.05).
The K10 scale, K-anxiety and K-depression scores were not statistically different between the respondents with different concerns except for the respondents who chose “psychological barriers and distrust”; they exhibited significantly higher K10 scale (p = 0.018), K-anxiety (p = 0.045) and K-depression (p = 0.014) scores as compared to the respondents with the primary concern of “isolation from family/society”.
Comparison of psychological indices between genders and the groups,
and within the groups
Regardless of the respondents’ group, females exhibited significantly higher K10 scale, K-anxiety and K-depression scores than males (p = 0.002, p = 0.002 and p = 0.003, respectively).
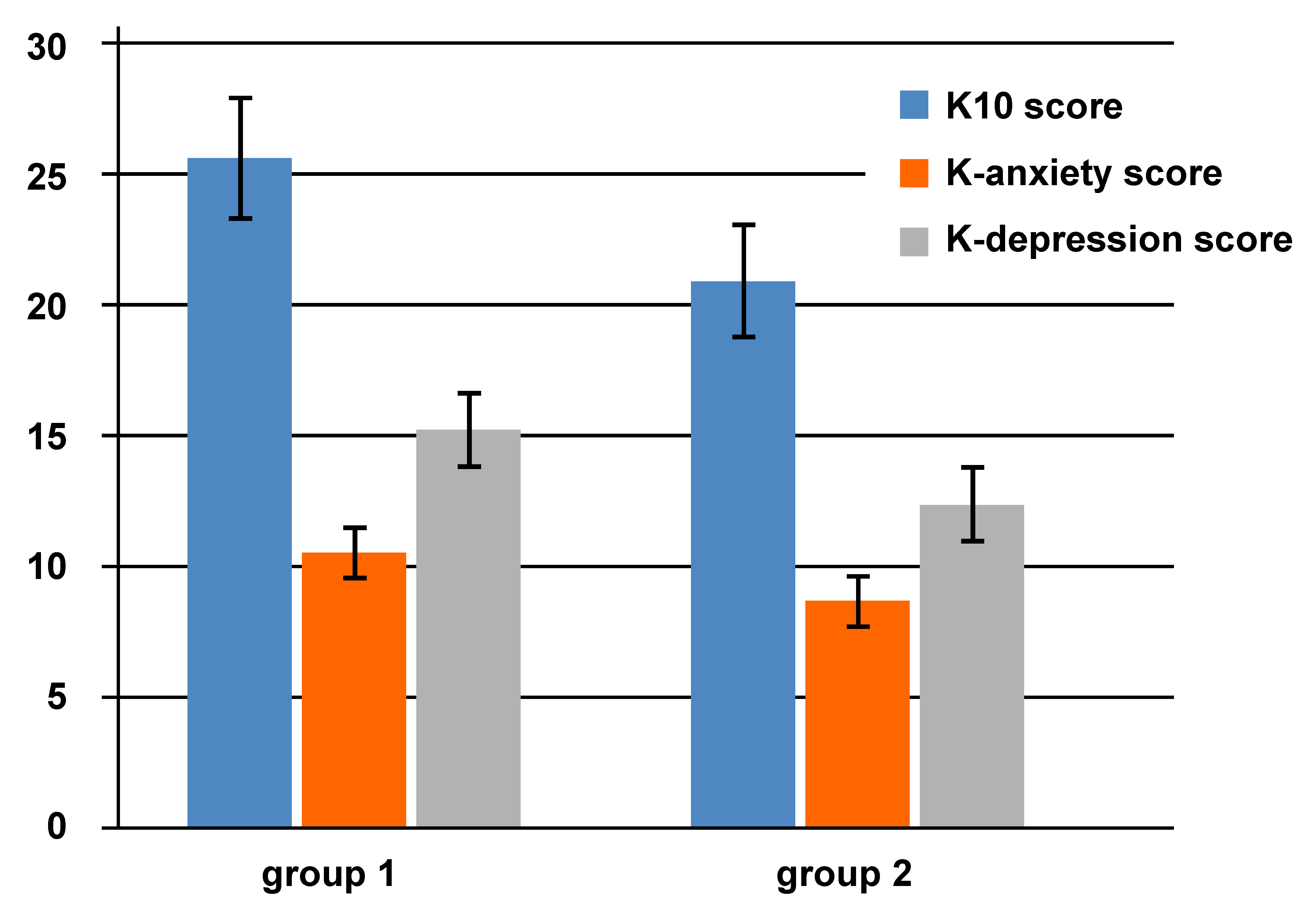
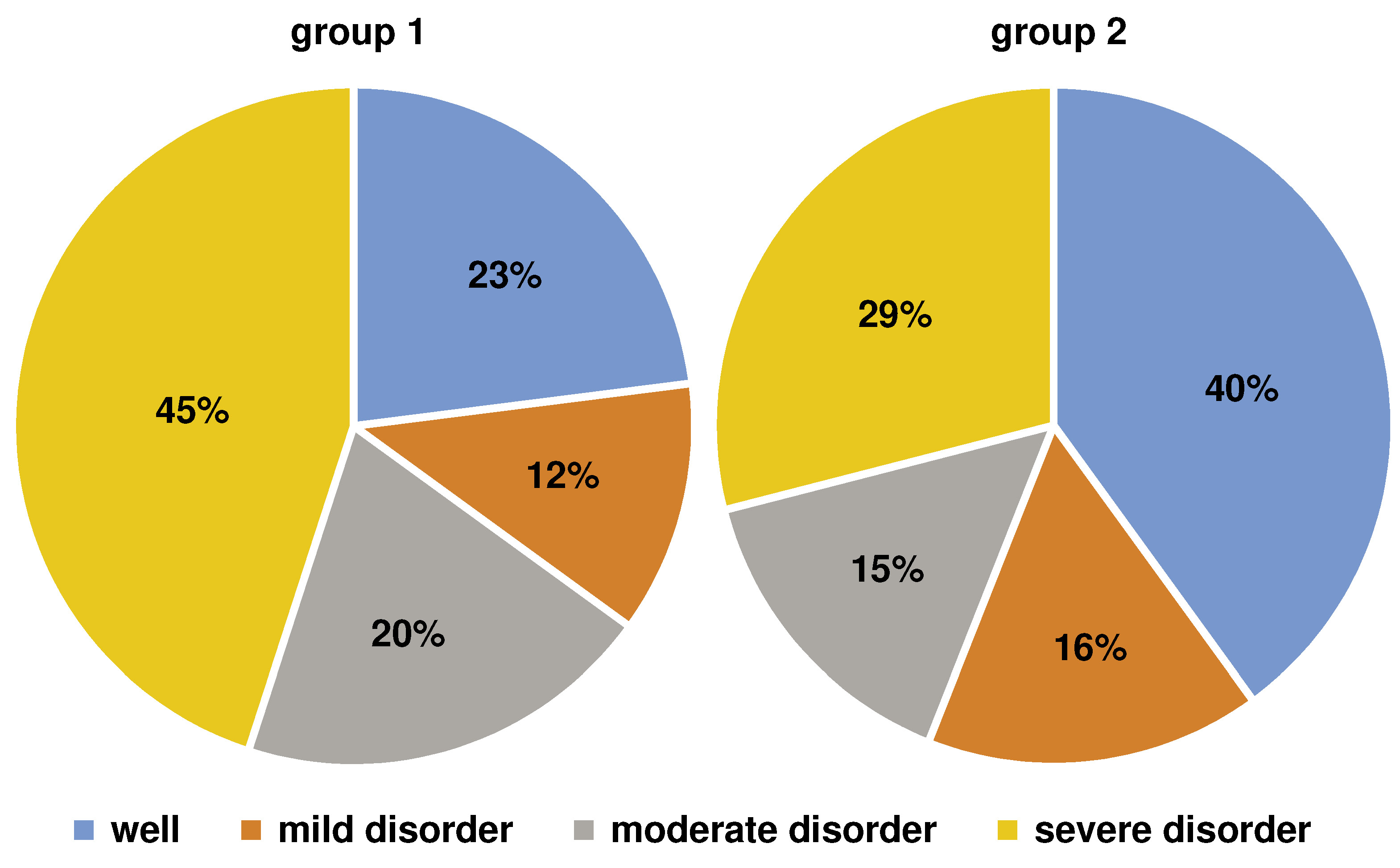
A one-way ANCOVA was conducted to determine statistically significant differences between the groups in terms of the K10 scale, K-anxiety and K-depression scores, controlling for the household income. The K10 scale, K-anxiety and K-depression scores were significantly higher in group 1 than in group 2 (p = 0.0001; FK10 = 18.31; FK-anxiety = 16.06; FK-depression = 18.29) (Figure 2). Group 1 exhibited a significantly higher percentage of individuals with mental distress than group 2 (p = 0.047) (Figure 3).
In group 1, 10.71% (n = 12) of the respondents sought pain management; they did not differ from the respondents in their group who did not seek treatment in terms of the K10 scale and K-anxiety and K-depression scores (p > 0.05).
Discussion
The COVID-19 pandemic has imposed a substantial psychological burden on the world population, especially at the beginning of the outbreak, when individuals encountered unexpected quarantine, unemployment and uncertainty associated with the outbreak.7 Pandemic-associated psychological factors might even exacerbate OFP.19 The treatment outcome of OFP can also be influenced by depressive symptoms.13 Therefore, the early identification of the populations in the first stages of a psychological crisis would allow for the efficient implementation of interventional strategies.3 This study analyzed anxiety and depression in 509 respondents, with 397 normal population individuals and 112 patients with OFP, during the COVID-19 pandemic. The factors associated with COVID-19-related psychological distress which were determined in previous studies28, 29, 30 were evaluated in our study. If they were different between the groups, they were adjusted not to affect the final comparison of the psychological status of the groups. Respondents with chronic illnesses and orthodontic treatment, or oral and maxillofacial surgeries were excluded, as these factors have been reported to affect the psychological condition.31, 32 In the present study, as the index of the psychological status, the Kessler Psychological Distress Scale was adopted21; it was previously used to assess the association between psychological distress and different types of pain, including musculoskeletal pain33 and all types of chronic pain.34
Our socio-demographic data suggests that females experienced a more significant psychological impact of the outbreak, and had higher levels of anxiety and symptoms of depression. This finding corresponds to a previous extensive epidemiological study, which found that women were at higher risk of depression.28 A study on Iranian medical students similarly revealed that anxiety was more prevalent in females than males; however, the study showed no significant difference between genders in depression.35 This contrast can be attributed to the fact that medical students respond differently to the pandemic-related psychological burden as compared to the general population. As previously reported in another research,30 older individuals exhibited less psychological distress in the present study, although the correlation was weak.
High levels of knowledge (score: 1.88–1.89 out of 2) and perception (score: 7.59–7.80 out of 10) in both groups represents success with regard to awareness measures and information programs. Higher knowledge of COVID-19 was associated with higher anxiety in the present study. It has been suggested that a higher level of information about COVID-19 received from various sources or the excessive use of media reporting on COVID-19 predict more anxiety among individuals,36, 37 which confirms our results. However, higher perception and a more positive attitude were found to be related to lower psychological distress. Previously, similarly to our findings, higher cognitive perception of the COVID-19 risk was reported to be related to a lower risk of depression for people in public health crises.38 Another study revealed that regardless of the actual amount of knowledge individuals had, those perceiving themselves as more knowledgeable exhibited a stronger sense of control and experienced more happiness during the outbreak.39
Moreover, our findings are consistent with the positive correlation between attitude and psychological quality of life assessed in previous studies, in which the higher the coping attitude about the disease was, the higher the score in the psychological domain was obtained.40, 41 Keeping in mind the knowledge–attitude–behavior theory, there is a complex interaction between knowledge, perception and attitude.42 Therefore, during the COVID-19 pandemic, all these variables should be addressed and improved concomitantly to enhance the related psychological status.
As for the main concerns about COVID-19, objective choices, like the impact on work/studies and daily life, were more important, while more subjective ones were relatively less important, such as the isolation from the family/society, psychological barriers and distrust among people. The main concern for individuals with OFP as well as for the general population was “impact on work/studies”.
The respondents who chose “psychological barriers and distrust” as the primary concern exhibited significantly higher psychological distress than the respondents with the primary concern of “isolation from family/society”. This is somehow justified by the results of a study on adults indicating that some cognitive strategies, such as rumination, catastrophizing and self-blame, are linked to poorer psychological well-being.43 In contrast, other strategies, like positive refocusing, putting into perspective and acceptance, show few significant associations with poorer psychological health.43
The main results of the present study indicated that the K10 scale, K-anxiety and K-depression scores were noticeably higher in participants with OFP than in the other group. The frequency of mental distress was higher in the OFP group.
This higher level of anxiety and depressive symptoms in individuals with OFP suggests that people with a history of pain experience would be possibly the main targets of psychiatric assessment and care. In a recent systematic review there was consistent evidence that chronic pain was associated with PTSD,44 which confirms our results. Previously, OFP, especially chronic pain, was associated with lower oral health-related quality of life, higher suicidal ideation, depression, anxiety, PTSD, and psychological distress signs.13, 18, 44 The comparison of the limited number of population-based studies is difficult due to different psychological indices and methods used.45, 46, 47, 48 None of the previous studies assessed the psychological status of patients with OFP in comparison with the general population after the psychological effect of an accident. However, our results are similar to those reported by Kindler et al., concerning psychological distress, and specifically the role of anxiety and depression related to pain; the authors found a moderate-to-strong relationship between the symptoms of depression or anxiety and the signs of TMD.46 Also, Natu et al. stated that the severity of TMD had some bearing on the quality of life, emotional states and sleep quality.47 Dindo et al. suggested that psychological inflexibility was related to the expression of the symptoms of anxiety and depression in adults with migraine.48 The results of a recent study by Simoen et al. before the pandemic indicated that patients with pain attributed to TMD had higher depression and anxiety scores in comparison with the general population.49 Although different psychological indices were applied (Patient Health Questionnaire-9 and Generalized Anxiety Disorder-7), their findings were similar to ours during the pandemic.49 A recent study showed that the aggravation of the psychoemotional status caused by the COVID-19 pandemic could result in the exacerbation of bruxism and TMD symptoms, and even lead to increased OFP.20
When people with chronic pain are denied assessment and treatment, their condition can worsen significantly, decreasing health-related quality of life, increasing pain and exacerbating depression.50, 51 Efforts are suggested to prevent and control pain – particularly chronic pain – during the COVID-19 pandemic. Moreover, addressing emergencies associated with pain, avoiding medication shortages due to panic-buying and avoiding the inaccessibility of the remaining healthcare options during movement restrictions are recommended, and pain management providers face the challenge of delivering face-to-face services through different modes.52
Most patients with OFP did not seek dental/medical pain management during the pandemic. A study suggested that precautionary measures, such as avoiding sharing utensils, hand hygiene and wearing masks to prevent the spread of COVID-19, could have had protective psychological effects during the early stages of the pandemic.28 Therefore, it might be concluded that the process of diagnosis and treatment of patients can be resumed with appropriate preventive measures so that they are not afraid of referring for pain management.
Overall, social media were the primary health information channels in both groups during the COVID-19 pandemic. Similarly to our findings, other studies reported that participants usually obtained information about the novel coronavirus through social media.53, 54 It should be noted that this large platform should be used for raising awareness and training in high-risk groups in the coronavirus pandemic, and the content of health information provided during the pandemic should be based on evidence to avoid adverse psychological reactions.28 On the other hand, this familiarity of the population with social media can be taken as an advantage. Telehealth, the sourcing of treatment modalities by means of digital and telecommunication technologies, can be provided by health professionals to exchange information necessary for self-care as well as the diagnosis, treatment and prevention of pathologies and injuries, including OFP or psychological distress.55
Varying degrees of the outbreak severity, national economy, government preparedness, the availability of medical supplies/facilities, a proper dissemination of COVID-related information, and cultural differences have led to regional differences in the general public’s psychological health during the pandemic.7 The COVID-19 outbreak began in Iran on February 19, 2020, and promptly spread all over the country. On April 21, 2020, of 330,137 tested patients, 80,868 were infected with COVID-19 (55,987 recovered, 3,513 became critically ill and 5,031 died). Like everywhere in the world, the formal announcement of the outbreak resulted in public panic and anxiety. Fake news and misinformation further increased public anxiety. The Headquarter for Coronavirus Combat and Prevention implemented strategies, such as stopping mass gatherings, the closure of educational institutes, national coordination with volunteer, civilian and military forces, the national screening program, and social distancing. These measures potently alleviated some of the public fear. However, at the same time, they could affect the economy. People were urged to strongly avoid familial gatherings and trips during the New Year holidays. Stricter measures, especially travel bans, were introduced on March 26, 2020. The measures desirably lead to the flattening of the epidemic curve.56 In the subsequent months, the government gained control of the virus and began relaxing lockdown measures. At the beginning of June 2020, the media reported a worrying sharp increase in the number of COVID-19 cases that mirrored March peak levels: 3,574 new infections in 24 h as of June 3.57
This is the first report on the psychological distress of individuals with OFP as compared to the general population during the COVID-19 pandemic, to the best of our knowledge. The main strengths of the present investigation are the comparison of the severity of this psychological distress and a considerable number of participants.
Like other questionnaire-based research, the accuracy of our study results depended on the participants’ accuracy in answering the questionnaire. Our respondents were mostly females and were of the young adult group. Due to ethical requirements concerning anonymity and confidentiality, we were not allowed to collect contact details and personal information from the respondents. As a result, we could not conduct a prospective study that would provide concrete evidence to support the need for a focused public health initiative. Given the limited resources available and the time-sensitivity of the COVID-19 outbreak, we adopted the non-randomized, convenient sampling strategy. Due to the cross-sectional design, the associations in the study cannot be perceived as causal. Lastly, this study had some limitations in interpreting the results, since COVID-19 is a novel coronavirus disease and limited research is available for comparison.
Future studies on a comparable number of males and females within various age groups are suggested. Furthermore, it would be ideal to conduct a prospective study on the same group of participants after some time, especially when all routine dental and medical procedures, including elective ones, are allowed. Future studies with a similar examination approach in a population-based group and a patient group are recommended to draw more logical conclusions.
Conclusions
In summary, our findings suggested that during the rapid rise of the COVID-19 outbreak, the psychological status was associated with knowledge, perception, attitude, and concerns about COVID-19. Females suffered more from psychological distress than males. As compared to the general population, psychological distress, and symptoms of depression and anxiety were noticeably higher in individuals with OFP, who suffered from moderate psychological distress.