Abstract
Background. Edentulism, a common condition, may be congenital or acquired later in life as a result of dental caries, periodontitis, aging, craniofacial trauma, or tumor resection. The rehabilitation of missing teeth can be achieved with dental implants. In cases of insufficient alveolar bone, several treatment options have been described in the literature, including maxillary sinus augmentation with bone grafting, the Le Fort I osteotomy, the angulated placement of conventional implants, and the use of specialized implants, such as zygomatic implants, which are anchored in the zygomatic bone.
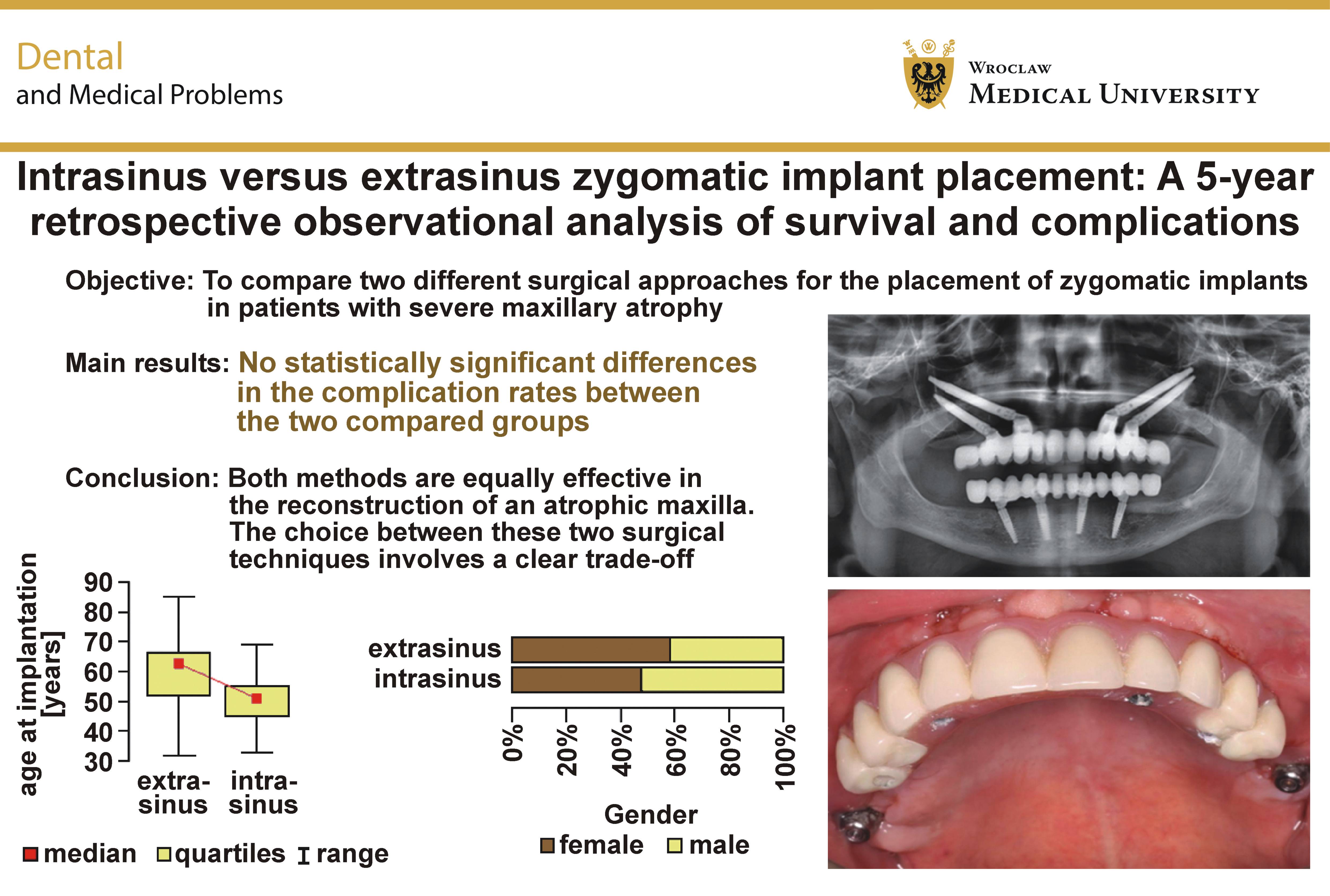
Objectives. The aim of this retrospective study was to compare 2 surgical approaches – intrasinus and extrasinus – for the placement of zygomatic implants in patients with severe maxillary atrophy.
Material and methods. The study was based on the medical records of patients who underwent zygomatic implant treatment conducted by the same surgeon at 2 dental facilities in Poland between 2004 and 2021. A total of 190 zygomatic implants placed in 69 patients of varying age and sex were included in the analysis. The follow-up period was 5 years. Two surgical approaches for zygomatic implant placement – intrasinus and extrasinus – were evaluated. Statistical analysis was performed using a significance level of 0.05. Differences between the groups were assessed using the χ2 test or Fisher’s exact test, as appropriate.
Results. The zygomatic implants placed using the intrasinus approach demonstrated a 100% survival rate. In the extrasinus group, the osseointegration rate was 94.27%, with implant loss occurring in 7 patients. Maxillary sinusitis was observed in 7 patients. Soft-tissue atrophy occurred in 4 patients (8.33%) and involved 14 zygomatic implants placed using the extrasinus technique. Cutaneous fistulas developed in 2 patients treated with the extrasinus approach. One case of zygomatic bone fracture was reported in the extrasinus group.
Conclusions. No statistically significant differences in the complication rates were observed between the intrasinus and extrasinus techniques for zygomatic implant placement. Both approaches appear to be equally effective for the rehabilitation of patients with severe maxillary atrophy.
Keywords: complications, survival, zygomatic implants, maxillary atrophy, zygoma
Introduction
The severely atrophic edentulous maxilla remains one of the greatest challenges in modern dental implantology.1, 2 Traditional reconstructive approaches, such as autogenous bone grafting3 and maxillary sinus augmentation, do not always provide predictable and long-term treatment outcomes. Moreover, these procedures require additional surgical interventions, and are associated with an increased risk of complications, higher treatment costs and prolonged rehabilitation time.4 In response to these limitations, the zygomatic implant technique was developed, allowing implants to be anchored in the dense zygomatic bone while bypassing the severely resorbed maxillary alveolar process.5, 6, 7, 8 The zygomatic bone has been shown to be more resistant to resorption than the maxilla.9 It consists of a dense peripheral cortical layer surrounding a relatively small core of trabecular bone.9 Owing to its high bone density (approx. 98%), the zygomatic bone provides a favorable site for implant anchorage.9
Zygomatic implants were first introduced by Brånemark in the late 1980s as an alternative treatment for patients with extensive maxillary bone loss.10 They were originally designed to provide stable prosthetic support in patients with severe resorption of the maxillary alveolar bone or partial or complete maxillary defects following oncologic resection, who were not suitable candidates for conventional dental implant placement.11 The original Brånemark protocol involved the placement of one zygomatic implant in each zygomatic bone, with the implants traversing the maxillary sinuses, in combination with 2–4 conventional implants placed in the anterior maxilla.11 Over the following decades, this technique underwent several modifications, resulting in the development of 2 principal surgical approaches: the intrasinus approach, in which the implant passes through the lumen of the maxillary sinus; and the extrasinus approach, in which the implant is positioned external to the sinus while preserving the integrity of the Schneiderian membrane.12, 13
Currently, patients increasingly expect rapid and effective oral rehabilitation. Minimizing the number of surgical procedures in implant therapy is therefore essential, as it improves patient comfort, reduces treatment burden, and enhances overall quality of life. Zygomatic implants eliminate the need for additional surgical interventions while providing treatment outcomes comparable to those achieved with other established implant rehabilitation protocols, such as the All-on-X concept. Furthermore, the strategies aimed at improving treatment predictability, including the application of stem cells, have been proposed. According to Sayed et al., stem cell therapy may enhance osseointegration and improve implant healing.14
The intrasinus technique involves creating a window in the lateral wall of the maxillary sinus to allow the visualization of the sinus cavity and facilitate the precise planning of the implant trajectory through the sinus to the zygomatic bone. This approach provides excellent primary stability through the quadricortical anchorage involving the palatal and zygomatic cortices. However, since it requires the perforation of the Schneiderian membrane, it may be associated with a higher risk of sinus-related complications, including maxillary sinusitis and subcutaneous abscess formation.15
To overcome the limitations of the intrasinus approach, the extrasinus technique was developed, allowing implant placement without penetrating the maxillary sinus. This method involves creating a limited access point in the lateral wall of the sinus (the zygomatic antrostomy zone) and guiding the implant in a predictable and more controlled manner along the external surface of the sinus toward the zygomatic bone while preserving the integrity of the Schneiderian membrane. By avoiding contact with the sinus mucosa, the extrasinus approach may reduce the risk of sinus-related complications and facilitates more favorable implant angulation for prosthetic rehabilitation.16, 17 In addition, the extrasinus technique prevents the displacement of the prosthetic retention elements toward the palatal aspect, thereby improving prosthetic emergence and the esthetic outcome of the final restoration. Furthermore, extrasinus implant placement has been associated with greater bone-to-implant contact (BIC),18 which may enhance secondary implant stability and contribute to the long-term maintenance of osseointegration.
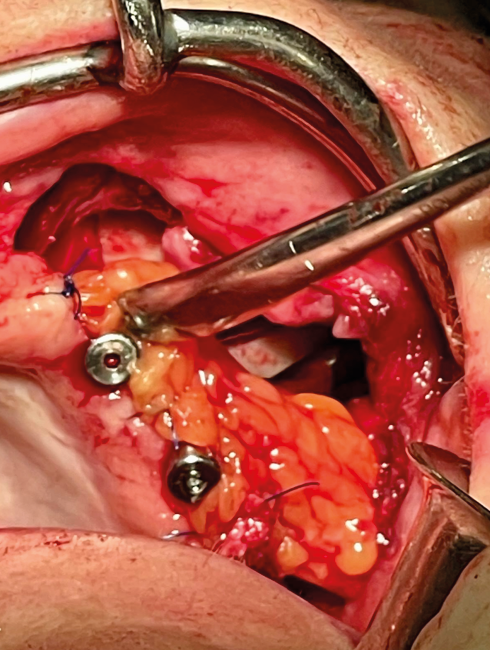
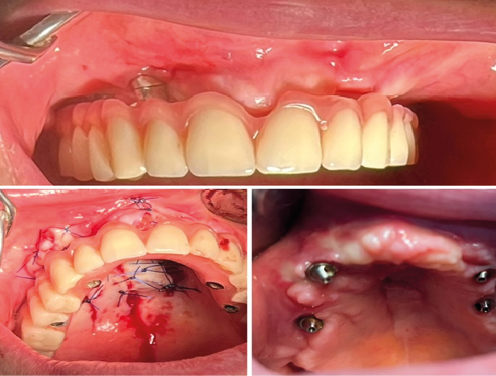
Contemporary implantology literature increasingly highlights the advantages of the extrasinus technique in terms of surgical simplicity, patient comfort and long-term clinical effectiveness. Although this approach offers several benefits, it also presents certain limitations, including soft-tissue atrophy with the potential exposure of the coronal portions of the implants. To prevent such complications, soft-tissue augmentation using the buccal fat pad (Bichat’s fat pad) is recommended in patients with a thin soft-tissue biotype to reduce the risk of gingival recession Figure 1).19
Although zygomatic implants represent a well-established solution for the severely atrophic maxilla, there remains a limited number of long-term comparative studies evaluating clinical outcomes between specific surgical protocols, namely the intrasinus and extrasinus approaches. While the extrasinus technique was developed to mitigate the risks associated with the original intrasinus method, such as sinusitis, it may introduce additional biological concerns, including soft-tissue recession.
The aim of this study was to address this gap by conducting a 5-year retrospective analysis comparing the intrasinus and extrasinus approaches. The study specifically evaluated the implant survival rates and the incidence of surgical and biological complications.
Materials and methods
The research was carried out in compliance with the Declaration of Helsinki and received approval from the institutional Bioethics Committee at the Medical University of Lublin, Poland (approval No. KE-0254/43/2019).
This retrospective observational study was based on the analysis of the medical records of patients treated with implant therapy at 2 dental facilities in Poland between 2004 and 2021. The study was conducted and reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. The included cases involved completely edentulous maxillae and posterior maxillary edentulous segments rehabilitated using zygomatic and conventional dental implants. The procedures were performed under both local and general anesthesia. The intrasinus technique was used between 2004 and 2013, whereas the extrasinus technique was introduced in 2010 and applied thereafter. Additional conventional implants were placed according to individual treatment plans.
The aim of the study was to determine which zygomatic implant approach for the reconstruction of missing teeth in cases of severe maxillary alveolar atrophy demonstrated the highest effectiveness and the lowest complication rate in the study population, based on a follow-up period of up to 5 years. The primary outcome was the number of complications observed in each group. Demographic factors, including patient age and sex, were also considered.
All patients who underwent zygomatic implant placement had been previously deemed unsuitable for sinus lift procedures for otolaryngological reasons. Prior to implant surgery, they had undergone otolaryngological treatment or functional endoscopic sinus surgery (FESS) in cases of ostiomeatal complex obstruction. The decision regarding surgical management was based on the combined findings from the SNOT-22 (Sino-Nasal Outcome Test-22) questionnaire, which assesses the subjective severity of sinonasal symptoms, and the Lund–Mackay scale, an objective radiological measure of sinusitis severity on computed tomography (CT).20
Characteristics of the clinical centers
The study was conducted at 2 dental centers in Poland – the Department of Oral Surgery, Medical University of Warsaw, and the Department and Chair of Periodontology, Medical University of Lublin.
Inclusion and exclusion criteria
The study included patients with completely edentulous maxillae or posterior maxillary edentulous segments, who provided written informed consent for implant-prosthetic rehabilitation using zygomatic implants. Each patient underwent panoramic radiography (orthopantomogram (OPG)) and cone beam computed tomography (CBCT). All patients were examine by an otolaryngologist, and all surgical procedures were performed by the same operator. The qualification criteria for the surgical intervention were more stringent for the intrasinus approach due to the limited availability of published data at the time and the surgeon’s learning curve; systemic diseases were present in only 2 patients in this group.
The inclusion criteria were eligibility for the permanent implant-supported prosthetic rehabilitation of a partially or completely edentulous maxilla in patients with severe alveolar ridge resorption and maxillary sinus pneumatization. All patients meeting the inclusion criteria during the study period were included in the analysis.
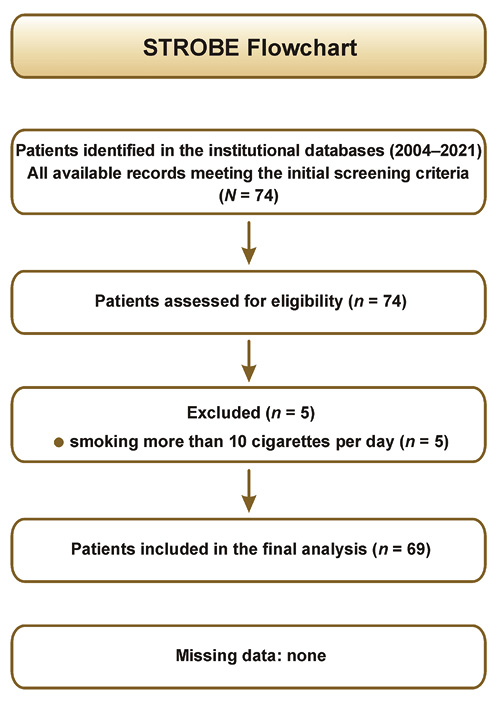
The exclusion criteria comprised severe systemic diseases, malignant conditions, poorly controlled diabetes, active autoimmune diseases, immunosuppressive drug therapy, bisphosphonate therapy, radiotherapy to the head and neck region, psychiatric disorders, parafunctional habits, and heavy smoking. The medical history of each patient was reviewed. Five patients were excluded due to smoking more than 10 cigarettes per day. All patients finally enrolled in the study were non-smokers.
The patients were allocated to groups according to the surgical technique used for implant placement. The study population did not present with systemic conditions considered to significantly affect osseointegration. No missing data was identified; therefore, no imputation or exclusion due to incomplete records was required.
The flowchart representing patient selection is depicted in Figure 2.
Distribution of patients by age and sex
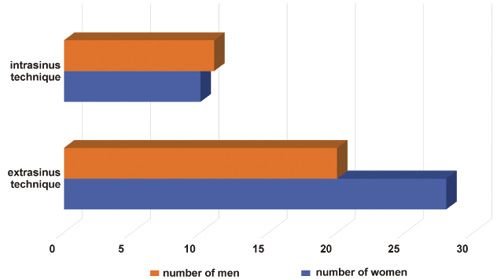
The study included 69 patients – 31 men and 38 women (Figure 3). The patients enrolled in the study ranged in age from 32 to 85 years. The median patient age was 62.5 years in the extrasinus group and 51.0 years in the intrasinus group. No patients older than 69 years were observed in the intrasinus approach. The most numerous age group in the intrasinus technique was 50–59 years, while in the extrasinus technique it was 60–69 years (Table 1).
Intrasinus approach
After removing the mucoperiosteal flap on both the palatal and buccal aspects, exposing the anterior wall of the maxillary sinus, an initial osteotomy mark was created using a drill with a diameter of 2 mm near the body of the zygoma. The tip of a large-diameter diamond bur was then positioned at the palatal entry point, and the preparation of the implant bed was initiated along the anterior and lateral walls of the maxillary sinus toward the zygomatic bone. The sinus mucosa was previously gently dissected after creating a window in the anterior sinus wall to allow access for the subsequent use of a 3.5-mm drill or the placement of a 4–4.5-mm zygomatic implant. A 2.5-mm guide drill was inserted at the crestal entry point and directed toward the previously marked zygomatic target, facilitating the trajectory through the maxillary sinus into the zygomatic bone. A depth gauge was then used to determine the appropriate drilling length for the 3.5-mm spiral drill, followed by final osteotomy preparation with the same drill. The zygomatic implant was inserted using an external screwdriver. The coronal (crestal) portion of the implant emerged slightly palatal to the residual alveolar ridge, in the region of the maxillary first molar. Finally, the wound was closed with 3-0 sutures.
Extrasinus approach
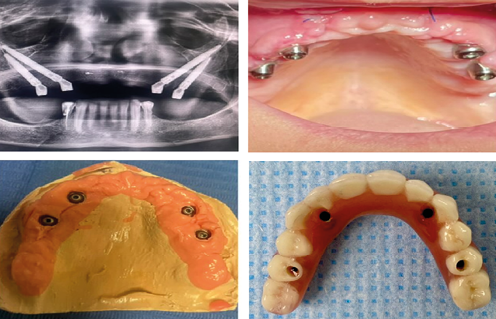
After the elevation of a full-thickness mucoperiosteal flap and the exposure of the surgical field, including the detachment of the zygomaticus major and minor muscle insertions, an initial reference point was created in the body of the zygomatic bone using a 2.0-mm drill. Subsequently, a guiding groove, approx. 15–20 mm long and 3–4 mm deep, was prepared along the lateral wall of the maxilla, using a large-diameter diamond bur, extending toward the planned implant anchorage site in the zygomatic bone. A 2.5-mm pilot drill was then advanced through the prepared groove toward the previously established reference point in the zygomatic bone. This approach enabled implant placement external to the maxillary sinus, with the implant emerging along the lateral wall of the sinus and achieving stable anchorage within the zygomatic bone. The osteotomy was sequentially enlarged using a 2.9-mm drill, followed by a 3.5-mm spiral drill. The implant length was determined with a depth gauge. The zygomatic implant was inserted so that the implant platform was positioned at the level of, or slightly coronal to, the alveolar crest (Figure 4). The surgical wound was closed with non-resorbable 3-0 sutures.
Immediate and final prosthetic protocol
Prosthetic rehabilitation was performed according to a standardized two-stage protocol. Immediately after implant placement, the patients received a screw-retained provisional full-arch acrylic resin prosthesis. Following a 6-month healing period, when successful osseointegration was confirmed clinically and radiographically, the provisional restoration was replaced with a definitive porcelain-veneered prosthesis.
Complication assessment
The following complications were assessed: the lack of implant osseointegration; zygomatic bone fracture; maxillary sinusitis; soft-tissue atrophy with the exposure of the coronal portion of the implant; and cutaneous fistula formation.
Follow-up period
All patients attended the scheduled follow-up visits at 7, 15, 30, and 60 days, as well as at 3, 6 and 12 months after surgery. Thereafter, follow-up examinations were performed at least annually.
To minimize the potential time-related bias resulting from the different observation periods of the historical intrasinus cohort and the more recently treated extrasinus cohort, administrative censoring at 5 years was applied in the survival analysis.
Statistical analysis
Statistical analyses were performed using the R software, v. 4.5.2. The significance level for all statistical tests was set at α = 0.05. To compare categorical variables between the intrasinus and extrasinus groups, the χ2 test was used. For 2 × 2 contingency tables, Yates’s continuity correction was applied when appropriate. Fisher’s exact test was used when the expected cell counts were low. All analyses were conducted at the patient level, with the exception of implant survival, which was analyzed at the implant level.
Results
A total of 190 zygomatic implants placed in 69 patients were included in the analysis. Of these, 33 implants were placed using the original Brånemark intrasinus technique, in which the implant traverses the maxillary sinus, whereas 157 implants were placed using the extrasinus technique, with the implant positioned external to the sinus cavity. The distribution of patients and implants according to the surgical technique is presented in Table 2.
Overall, 8 patients were rehabilitated exclusively with either 2 or 4 zygomatic implants, using the extrasinus approach. The remaining 61 patients underwent rehabilitation with a combination of zygomatic and conventional dental implants (the mixed technique).
A total of 336 conventional dental implants were placed, including 197 in the extrasinus group and 139 in the intrasinus group.
Among the patients treated with the extrasinus approach, 9 were completely edentulous. In the intrasinus group, 8 of 21 patients were completely edentulous. Overall, 17 of the 69 patients included in the study presented with complete edentulism.
Incidence of complications
Zygomatic implant loss occurred in 9 implants, all of which had been placed using the extrasinus technique; no implant failure was observed in the intrasinus group. All implant losses occurred 6 months after surgery, during prosthetic loading. Implant failure affected 7 patients in the extrasinus group (14.58%; 4 men and 3 women; age range: 45–68 years). No patients treated with the intrasinus approach experienced zygomatic implant failure. The difference in the implant failure rates between the 2 groups was not statistically significant (Table 3).
The zygomatic implants placed using the intrasinus approach demonstrated a 100% success rate. In the extrasinus group, successful osseointegration was achieved in 94.27% of implants, corresponding to a failure rate of 5.73% (Table 4). No smokers were present in either group. The overall implant success rate was 95.26%.
Maxillary sinusitis occurred in 3 patients (3 men; age range: 41–55 years) whose zygomatic implants traversed the maxillary sinus (14.29% of patients in this group). None of these patients were smokers. The symptoms of maxillary sinusitis in the extrasinus group were observed in 4 patients (3 men and 1 woman; age range: 56–85 years), representing 8.33% of patients treated with this approach. None of these patients smoked cigarettes. No statistically significant difference in the incidence of sinusitis was found between the groups (Table 3). Overall, maxillary sinusitis occurred in 10.14% of patients.
Soft-tissue atrophy with coronal implant exposure occurred in 4 patients (8.33%; 1 man and 3 women; age range: 45–63 years), involving 14 zygomatic implants placed using the extrasinus technique (Figure 5). No such complication was observed in the intrasinus group. None of the patients in either group were smokers. No statistically significant difference in the incidence of this complication was found between the groups (Table 3). Overall, the incidence of soft-tissue atrophy with coronal implant exposure was 5.80%.
Cutaneous fistulas (Figure 6) occurred in 2 patients (one male and one female; both aged 45 years) treated using the extrasinus approach (4.17% of patients in this group). In one case, the removal of the zygomatic implant was required. No cutaneous fistulas were observed in the intrasinus group. No statistically significant difference in incidence was found between the compared groups (Table 3). Overall, cutaneous fistulas occurred in 2.90% of patients.
One case of zygomatic bone fracture was reported in a 52-year-old female patient without comorbidities, a non-smoker, treated using the extrasinus approach (2.08% of patients in this group). During implant placement, miniplate osteosynthesis was performed. This complication was not observed in the intrasinus group. No statistically significant difference in incidence was found between the compared groups (Table 3). Overall, zygomatic bone fracture occurred in 1.45% of patients.
Discussion
The simultaneous occurrence of increased maxillary sinus pneumatization and advanced alveolar bone loss presents a therapeutic challenge for oral and maxillofacial surgeons. To avoid multistage procedures, such as guided bone regeneration (GBR) or sinus augmentation, the use of zygomatic implants has been proposed as an alternative solution. Numerous prospective studies have demonstrated the high effectiveness of this approach.21 Implant placement in the zygomatic bone as an alternative to maxillary reconstruction with the use of autogenous bone grafts has been considered a viable option for the rehabilitation of severely atrophic jaws.22, 23, 24, 25 Based on the available literature, most implant failures occur within the first 6 months after surgery,21 which is consistent with our findings. The reported complications included the lack of osseointegration within 6 months of surgery, maxillary sinusitis, soft-tissue atrophy with the exposure of the coronal portions of the implants, cutaneous fistulas, and zygomatic bone fracture.
Osseointegration is defined as a direct structural and functional connection between ordered living bone and the surface of a load-bearing implant.26 This process is a key determinant of successful implant outcomes and is achieved through functional ankylosis.18 Multiple factors influence osseointegration, including implant-related factors, host-related factors, the surgical technique, healing time, and the loading conditions.26
In the present study, osseointegration was achieved in 95.26% of all zygomatic implants, which is comparable with the results reported by Chrcanovic et al., who demonstrated a 95.2% survival rate of zygomatic implants after 12 years of follow-up,21 and by Sales et al., who reported an overall survival rate of 96.7%.27 The present study showed that the zygomatic implants placed using the extrasinus approach demonstrated a 94.27% success rate, which was 5.73% lower than that observed in the intrasinus group. A total of 9 zygomatic implants were lost, all in the extrasinus group. For comparison, conventional dental implants have been reported to have failure rates ranging from 1% to 19%.28 None of the patients who experienced zygomatic implant failure were smokers or presented with significant systemic conditions that could have affected osseointegration.
Maxillary sinusitis occurred in 3 patients who received zygomatic implants that traversed the maxillary sinus (14.29% of patients treated with this approach). The symptoms of maxillary sinusitis were observed in 4 patients treated using the extrasinus technique (8.33% of patients in this group). These findings are consistent with the data reported in the literature, where the incidence of sinusitis after zygomatic implant placement ranges from 0% to 26.6%.9 In the present study, maxillary sinusitis occurred in 10.14% of all enrolled patients. This was most likely associated with perforation or trauma to the Schneiderian membrane during implant placement, and persistent communication between the maxillary sinus cavity and the zygomatic implant. Similar conclusions were reported by Jain et al., who described several cases of sinusitis associated with the intrasinus technique.9
In this study, soft-tissue atrophy with the exposure of the coronal portion of the implant occurred in 14 implants placed using the extrasinus technique, whereas no such complication was observed in the intrasinus group. This finding suggests that the position of the implant neck relative to the alveolar crest is critical for peri-implant soft-tissue stability. Although the survival rate of zygomatic implants is reported in the literature to range from 92.3% to 100%,29 researchers also emphasize the potential for biological complications, including soft-tissue-related adverse events.21 The extrasinus technique, as described by Aparicio et al.,30 effectively reduces the risk of maxillary sinusitis; however, in less favorable anatomical conditions, it may result in mucosal recession and the exposure of implant threads.17, 31 In this technique, the coronal portion of the implant is positioned lateral to the alveolar crest, often with limited bony support. In such conditions, a thin mucosal phenotype and insufficient width of keratinized tissue may predispose to soft-tissue recession, as previously demonstrated for conventional implants by Linkevicius et al.32 and Lin et al.33 To prevent such complications, soft-tissue augmentation using the buccal fat pad (Bichat’s fat pad) is recommended in patients with a thin mucosal phenotype.
According to the present study, zygomatic bone fracture occurred in 1 of 69 patients (1.45%), which is consistent with the data reported in the literature. D’Agostino et al. described one case of right zygomatic bone fracture among 45 patients (2.22%).34 In the present study, this complication was observed only in the extrasinus group. The affected patient was managed immediately with miniplate osteosynthesis.
Cutaneous fistulas following zygomatic implant placement have a multifactorial etiology, although local factors related to the surgical technique play a key role. The most frequently cited cause is the overheating of the zygomatic bone around the implant threads due to insufficient irrigation and heat accumulation in the dense zygomatic bone, which may lead to bone necrosis, resorption and secondary infection.35, 36, 37 In the present study, cutaneous fistulas occurred in 2.90% of cases (2 of 69 patients).
The risk of fistula formation increases when the inter-implant distance is reduced, particularly in cases involving 2 implants placed in the same zygomatic bone, where heat accumulation between osteotomy sites may be greater.37 Vrielinck et al. reported an association between peri-zygomatic infections and insufficient inter-implant spacing,35 while an experimental study by Li et al. confirmed that reducing the distance between osteotomies significantly increased bone temperature above the threshold for thermal injury.37
Additional etiological factors include the presence of bone debris and the fragments of Schneiderian membrane in the difficult-to-access apical region of the surgical field, excessive insertion torque (overtorquing),38, 39 which may contribute to delayed bone necrosis,35 as well as the mechanical irritation of soft tissues by the protruding implant apex.40 Review studies further indicate that these infections are more frequently observed in patients treated with the quad zygoma protocol, in which 2 implants are placed in the same zygomatic bone.36, 41
In the present study, the first patient in whom this complication occurred had 2 zygomatic implants placed in the right zygomatic bone, whereas the second patient received a single zygomatic implant in the left zygomatic bone. Cutaneous fistulas were observed exclusively in the extrasinus group, which may be related to the use of more aggressive implant trajectories as compared to the intrasinus approach. The extrasinus technique emphasizes primary implant stability; however, excessive insertion torque in combination with the dense structure of the zygomatic bone may contribute to subsequent bone necrosis and fistula formation.
The management of cutaneous fistulas is primarily surgical. In selected cases, conservative treatment may be considered, consisting of the resection of the apical portion of the implant (apicoectomy) and the curettage of the inflamed tissue.38, 39 However, in cases of implant instability, significant bone loss or persistent infection, complete implant removal, the surgical debridement of the infected site, and fistuloplasty are required.35 Antibiotic therapy may serve as an adjunctive measure, but does not replace surgical management in cases of persistent fistula formation. In the present study, one zygomatic implant required removal as a result of this complication.
Despite the 100% success rate observed with the intrasinus approach, our retrospective analysis of medical records suggests lower patient tolerance and less favorable prosthetic esthetics as compared to the extrasinus technique, which is consistent with the previously published data. It has been demonstrated that, in the extrasinus approach, the coronal portion of the zygomatic implant is positioned closer to the alveolar crest, which reduces prosthesis bulk, and facilitates hygiene, speech and mastication.42 In contrast, in the original intrasinus zygomatic implant protocol developed by Brånemark, the coronal portion of the implant is located in a more palatal position, which may complicate the fabrication and use of the prosthesis. This positioning can negatively affect the biomechanics and alignment of the maxillary prosthetic arch, potentially leading to malocclusion.43
Currently, several methods are available for the rehabilitation of missing teeth in cases of an atrophic maxilla that eliminate the need for bone augmentation or maxillary sinus floor elevation, including prosthetic rehabilitation using short and ultra-short implants. As reported in previous studies, short and extra-short implants placed in the posterior maxilla demonstrate high survival rates and may reduce patient morbidity associated with advanced grafting procedures.44 However, in cases of severe alveolar ridge atrophy and high bone resorption, salvage implantology techniques, including zygomatic implants, are often required.
Limitations
It should be noted that this study was retrospective in nature, which limited the ability to fully standardize procedures and control for all potential confounding variables. A lack of comparability between the groups was observed with respect to the sample size, which may have influenced the robustness of the results. The study was subject to selection bias, as the inclusion criteria were more stringent for the intrasinus technique due to the limited availability of evidence at the time and the surgeon’s learning curve. In addition, the long inclusion period (2004–2021) introduced potential temporal bias, as surgical protocols, materials and clinical experience likely evolved over this 17-year period (the primary confounding variable).
A significant baseline imbalance was also observed between the cohorts, with a higher median age in the extrasinus group (62.5 years) as compared to the intrasinus group (51.0 years), representing a potential confounding factor. To address differences in the maximum follow-up duration between the cohorts, administrative censoring at 5 years was applied to reduce the bias related to unequal observation times.
The influence of systemic diseases on the complication rates was not specifically evaluated, as the study population did not include the conditions considered to significantly affect osseointegration. Moreover, it has been reported that systemic diseases are not significantly associated with an increased incidence of complications in zygomatic implant therapy.45
Another limitation was the absence of standardized patient-reported outcome measures (PROMs), as treatment tolerance and esthetic satisfaction were assessed retrospectively from medical records. Finally, as all procedures were performed by a single operator, the findings may reflect individual clinical expertise and may not be fully generalizable to the broader surgical community.
Future prospective studies with balanced cohorts and biomechanical analyses are warranted to further validate these findings.
Conclusions
Based on the present study and the postoperative evaluation using various clinical criteria, no statistically significant differences in the complication rates were observed between the 2 zygomatic implant techniques. Both approaches appear to be equally effective for the rehabilitation of the severely atrophic maxilla.
The extrasinus technique allows for a more favorable prosthetic emergence profile at the level of the alveolar ridge rather than the palate, which facilitates prosthetic rehabilitation and results in esthetics comparable to that achieved with conventional implants. However, it may be associated with a higher risk of soft-tissue complications and biomechanical challenges. Although the intrasinus technique demonstrated a 100% implant survival rate and no soft-tissue complications in this study, it was associated with greater surgical invasiveness and less favorable prosthetic esthetics. Thus, the choice between these 2 techniques involves a clear clinical trade-off.
Further long-term studies are required to optimize the biomechanical stability and clinical predictability of the extrasinus approach.
Ethics approval and consent to participate
The study was conducted in compliance with the Declaration of Helsinki and was approved by the institutional Bioethics Committee at the Medical University of Lublin, Poland (approval No. KE-0254/43/2019). The study had a retrospective design and was based on the analysis of the existing clinical records. No identifiable patient data is presented in the manuscript.
Data availability
The datasets supporting the findings of the current study are available from the corresponding author on reasonable request.
Consent for publication
Not appicable.
Use of AI and AI-assisted technologies
Not applicable.