Abstract
Medication-related osteonecrosis of the jaw (MRONJ) is a severe complication associated with antiresorptive and antiangiogenic therapies. Laser-based approaches, including photobiomodulation therapy (PBMT) and erbium laser-assisted surgery, have been proposed as adjunctive interventions to improve healing and clinical outcomes. This consensus-based review aimed to synthesize evidence from systematic reviews and meta-analyses evaluating laser-based therapies in the prevention and treatment of MRONJ, and to translate these findings into clinical recommendations developed by the World Federation for Laser Dentistry (WFLD) and the Polish Society for Laser Dentistry (PTSL).
The review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 and Joanna Briggs Institute (JBI) guidance, and was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO). An electronic search of the PubMed/MEDLINE, Embase, Scopus, and Cochrane Library databases was conducted for systematic reviews and meta-analyses published between January 2015 and October 2025. Study selection, data extraction and methodological assessment were performed independently by 3 reviewers.
Eighty-five records were identified, and 14 reviews met the inclusion criteria. These included several hundred primary studies, mainly observational studies and case series. Laser-based interventions were primarily used as adjuncts to conventional MRONJ management. Photobiomodulation therapy was associated with pain reduction and improved soft tissue healing, while erbium-doped yttrium aluminum garnet (Er:YAG) laser-assisted surgery enabled the precise removal of necrotic bone. Combined protocols showed generally favorable trends. However, substantial heterogeneity in study design, laser parameters and outcome definitions precluded quantitative synthesis.
Laser-based therapies may provide beneficial adjunctive effects in MRONJ management, particularly within multimodal treatment strategies. However, the strength of these conclusions is limited due to substantial heterogeneity in study design, laser protocols and outcome reporting.
Keywords: laser therapy, low-level laser therapy, MRONJ, PBM, erbium laser
Introduction
Rationale – MRONJ
Medication-related osteonecrosis of the jaw (MRONJ) is a serious complication in dental and oncologic care, affecting patients treated with bone-modifying agents, such as bisphosphonates and denosumab, or antiangiogenic therapies.1, 2 It is defined as exposed bone or bone that can be probed through a fistula in the maxillofacial region, persisting for more than 8 weeks, in patients with current or prior exposure to these agents and no history of jaw irradiation, and it is associated with substantial morbidity and reduced quality of life (QoL).1, 3 The incidence of MRONJ varies according to indication and dosing.1, 3 Population-based data indicates an overall incidence approaching 9% in high-dose recipients, with denosumab associated with a five-fold higher risk than bisphosphonates, and the sequential antiresorptive therapy further increasing the risk.4, 5
The pathophysiology of MRONJ is multifactorial and not fully elucidated, involving impaired bone remodeling, osteoclast suppression, reduced angiogenesis, soft tissue toxicity, and the unique biological characteristics of jaw bones.3, 6, 7 Bisphosphonates induce osteoclast apoptosis via the inhibition of the mevalonate pathway, while denosumab suppresses osteoclast formation by neutralizing receptor activator for nuclear factor-kappa B ligand (RANKL), leading to necrotic bone accumulation and impaired healing after dental trauma or infection.7, 8, 9 The management of established MRONJ remains largely empirical. Conventional treatment comprises antimicrobial rinses, systemic antibiotics, conservative debridement, and surgical resection in advanced cases, with outcomes strongly dependent on the disease stage.1, 10, 11 Earlier guidelines favored predominantly conservative management, reserving surgical intervention for non-responsive or advanced disease. However, contemporary position papers, including that by the American Association of Oral and Maxillofacial Surgeons (AAOMS) from 2022,12 increasingly support timely intervention, even in selected stage 1 cases, when patient-related and local conditions permit. Despite this shift, no standardized gold-standard protocol exists, and clinical outcomes remain variable, particularly for higher-stage lesions.12, 13, 14 Given these limitations, adjunctive therapies targeting impaired angiogenesis, cellular dysfunction and deficient bone remodeling have gained interest.
Rationale – laser therapy
Laser-based therapies have demonstrated biological effects, including enhanced cellular proliferation, angiogenesis, inflammation modulation, and osteogenic differentiation.15, 16, 17 Experimental and translational studies have shown that photobiomodulation therapy (PBMT) improves cellular viability, modulates apoptotic pathways, and enhances osteogenic and mesenchymal marker expression in oral soft tissues and bone-related cells, providing a strong biological rationale for its use in compromised healing conditions.18, 19 Clinically, PBMT has been shown to reduce pain, support soft tissue healing and improve bone-related outcomes in various dental and maxillofacial indications, supporting its consideration as an adjunctive modality in high-risk oral surgical settings.20, 21, 22, 23, 24 Emerging evidence suggests that PBMT may reduce MRONJ incidence after dental procedures and improve healing when used adjunctively.18, 25, 26, 27, 28, 29 Systematic reviews report benefits, including pain reduction and improved soft and hard tissue healing, although significant heterogeneity in laser modalities, irradiation parameters and outcome measures limits definitive conclusions.17, 30, 31, 32 In contrast to PBMT, erbium-based lasers, such as the erbium-doped yttrium aluminum garnet (Er:YAG) laser, are primarily used for hard tissue interaction and precise debridement, and may be effectively combined with PBMT to enhance tissue healing and to modulate inflammatory responses in clinical settings,33, 34, 35 enabling the precise ablation of mineralized tissues with minimal thermal damage,36, 37, 38 providing bactericidal effects,34, 35, 39, 40, 41 and preserving the surrounding structures, which is particularly relevant in the surgical management of necrotic or infected bone.42, 43, 44 Given the complexity of MRONJ pathophysiology and the heterogeneity of the available therapeutic approaches, there is a need for a structured synthesis of the evidence regarding laser-assisted interventions. Beyond evidence synthesis, the present review aims to translate the available literature into a clinically interpretable framework and consensus-based recommendations developed jointly by the World Federation for Laser Dentistry (WFLD) and the Polish Society for Laser Dentistry (PTSL), addressing both the preventive and therapeutic applications of laser technologies in MRONJ management.
Aims
The aim of this literature-supported consensus statement was to systematically synthesize and critically appraise evidence from systematic reviews and meta-analyses evaluating the clinical effectiveness and safety of laser-based therapies in the prevention and treatment of MRONJ.
In addition, the study assessed the methodological quality of the included reviews, and used the available evidence to inform clinically oriented interpretations and consensus-based recommendations from WFLD and PTSL, while identifying key gaps and priorities for future research.
Methods
This publication was designed as a consensus statement supported by a structured overview of systematic reviews and meta-analyses. Accordingly, it should not be interpreted as a standalone review, but rather as a clinically oriented consensus document supported by a structured synthesis of systematic review evidence. The study was conducted in accordance with the Joanna Briggs Institute (JBI) methodology and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines, and was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD420251269761).45, 46, 47, 48, 49, 50 A quantitative meta-analysis was not performed due to substantial heterogeneity across the included reviews in terms of laser modalities, irradiation parameters, clinical indications, and outcome definitions. A formal primary-study overlap analysis (e.g., via the corrected covered area formula) was not performed, as its interpretive value was considered limited given the substantial clinical and methodological heterogeneity across the included reviews. However, the potential overlap of primary studies across the included systematic reviews may have influenced the apparent consistency of findings and was considered during the qualitative interpretation of the evidence. Therefore, the reported patterns should be approached with caution, particularly where similar outcomes are described across multiple reviews. Formal Grading of Recommendations Assessment, Development and Evaluation (GRADE)-based certainty-of-evidence assessment was also not undertaken, as the evidence base consisted predominantly of heterogeneous systematic reviews of non-randomized and observational studies, with substantial variability in interventions, clinical settings and the reported outcomes. Under these conditions, the application of GRADE would not enable reliable or internally consistent certainty ratings across recommendations and could result in misleading interpretations of the evidence strength. This approach is consistent with the interpretative and consensus-oriented nature of the present work.
Review PICO question
In patients diagnosed with medication-related osteonecrosis of the jaw (Population), does the use of laser-based therapies (Intervention), compared with conventional surgical or non-surgical management without laser application (Comparison), lead to improved clinical outcomes, including enhanced wound healing, reduction in pain and inflammation, decreased lesion progression, or improved quality of life (Outcome)?48 Both the preventive and therapeutic applications of laser-based interventions were considered, provided they were evaluated within the context of MRONJ. Preventive applications refer primarily to peri-extraction or management strategies in high-risk patients, as well as early-stage disease, where photobiomodulation (PBM) may support tissue healing and reduce inflammatory burden. However, the available evidence in this context remains more limited as compared to therapeutic interventions.
Search strategy
A systematic literature search was performed across major electronic databases, including PubMed/MEDLINE, Embase, Scopus, and the Cochrane Library, to identify published systematic reviews and meta-analyses evaluating the use of laser therapies in the prevention or treatment of MRONJ. Three independent reviewers performed the search, using a predefined combination of Medical Subject Headings (MeSH) terms and free-text keywords related to MRONJ, osteonecrosis of the jaw, and laser-based interventions. The search was restricted to English-language publications, with no year-of-publication limit, and was completed in October 2025, including all records available as of October 1. Study selection followed a two-stage screening process. Titles and abstracts were initially screened, followed by full-text assessment against the predefined inclusion and exclusion criteria, conducted independently by 3 reviewers. The reference lists of all included reviews were manually examined to identify additional relevant studies. The final search encompassed literature published between 2015 and 2025 across the selected databases (Table 1).
Eligibility criteria
Three reviewers independently screened titles and abstracts, and then full text-articles, using the predefined criteria aligned with this consensus statement’s objectives. Disagreement was resolved through discussion. We included peer-reviewed systematic reviews and meta-analyses on laser therapies for MRONJ prevention or treatment, reporting clinical outcomes like mucosal/bone healing, pain/inflammation reduction, lesion stabilization, or patient-reported improvement. Studies required transparent methodologies with defined controls and measurable outcomes. Excluded were non-peer-reviewed works, narrative reviews, expert opinions, editorials, abstracts, theses, non-English publications, methodologically vague studies, non-laser MRONJ interventions, duplicates, and redundant secondary analyses.
Study selection
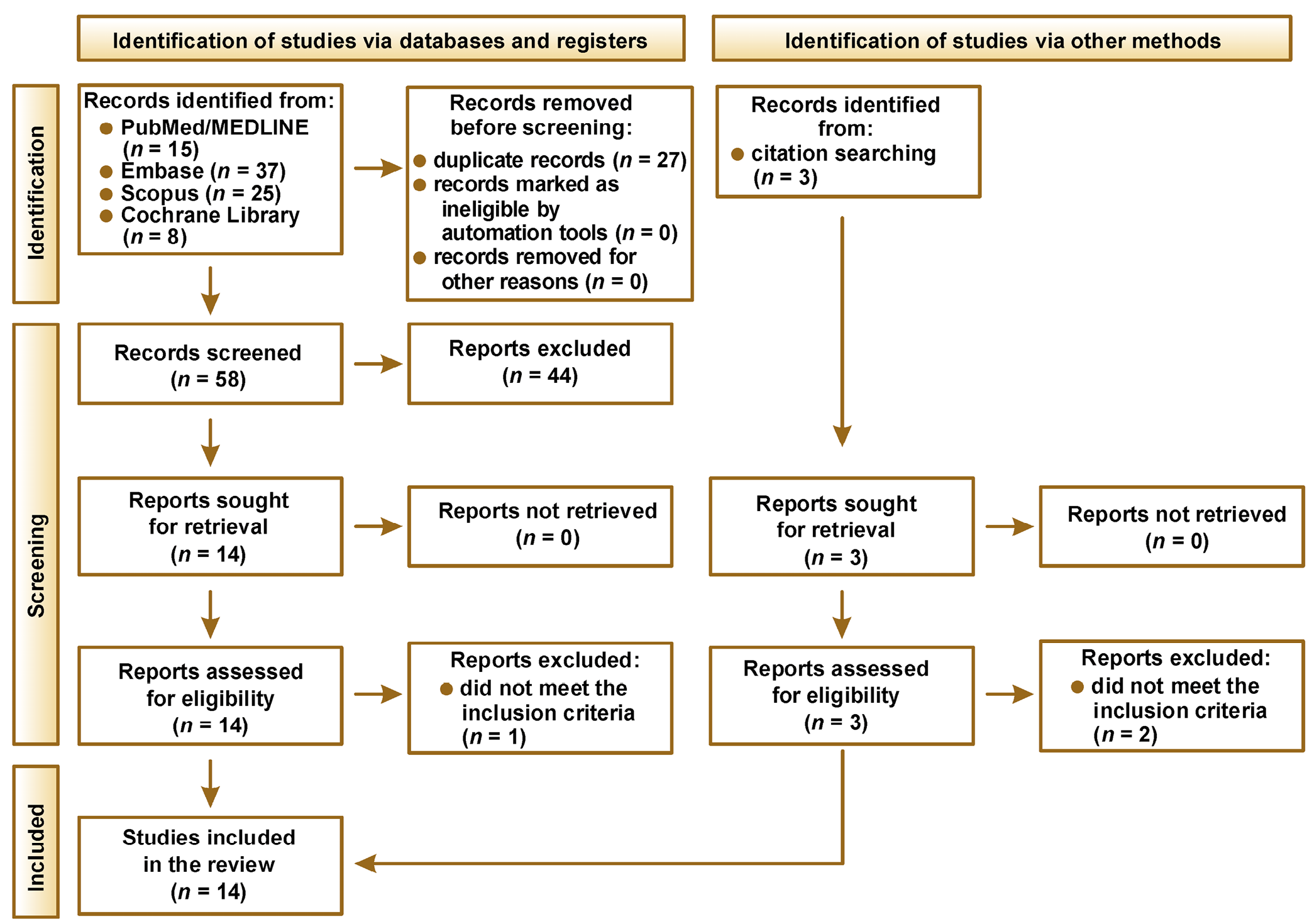
A total of 85 records were initially identified through database searching, including PubMed (n = 15), Embase (n = 37), Scopus (n = 25), and the Cochrane Library (n = 8). After the removal of duplicate records (n = 27), 58 unique records remained and were subjected to title and abstract screening. During this stage, 44 records were excluded based on the predefined eligibility criteria, resulting in 14 reports being sought for full-text retrieval. All 14 reports were successfully obtained and assessed for eligibility. Following full-text evaluation, 1 report was excluded, since it did not meet the inclusion criteria, leaving 13 studies eligible from database sources. In addition, 3 records were identified through citation searching. All 3 reports were retrieved and assessed for eligibility. Two reports were excluded at the full-text stage for not meeting the inclusion criteria, resulting in 1 additional eligible study. Consequently, a total of 14 studies were included in the final review (Figure 1).
The included studies were categorized according to their primary clinical intent into preventive (peri-extraction or high-risk patient management) or therapeutic applications, the latter further subdivided into non-surgical or laser-assisted surgical management, primarily using Er:YAG lasers for necrotic bone removal.
Data extraction
Three reviewers independently performed data extraction using a standardized and predefined protocol to ensure consistency and minimize bias. The key information collected from each included review comprised the first author, the year of publication, clinical settings, and the characteristics of the patient population affected by MRONJ.
The extracted parameters included the type of laser or photonic device, wavelength, power output, energy density or fluence, the mode of application, the duration of exposure, and the number of treatment sessions. When available, additional details, such as treatment frequency, the target tissue or surgical site, and whether laser therapy was applied as a standalone or adjunctive modality, were also documented.
The outcomes of interest encompassed both primary and secondary clinical measures, including the resolution or stabilization of necrotic lesions, improvement in soft tissue and bone healing, reduction in pain and inflammatory symptoms, a decreased risk of disease progression, and improvement in patient QoL. This data was systematically recorded to facilitate comparative analysis across the studies, and to evaluate the consistency, reliability and clinical relevance of the reported therapeutic effects in support of evidence-based recommendations.
Risk of bias and quality assessment
The methodological quality of each included review was independently assessed by 3 reviewers using a structured risk-of-bias evaluation tool specifically adapted for reviews investigating laser-based therapeutic interventions in MRONJ. This tool comprises 9 domains designed to appraise methodological transparency and internal validity. The assessment criteria included:
(1) comprehensive identification and detailed description of the laser system and treatment parameters, such as wavelength, power output, energy density, and mode of application;
(2) clear definition of treatment protocols, including frequency, duration, and whether laser therapy was applied as a primary or adjunctive modality;
(3) explicit specification of clinically relevant outcomes, including the improvement of necrotic lesions, pain reduction, and soft tissue or bone healing;
(4) inclusion of appropriate control or comparator groups;
(5) transparent inclusion criteria with detailed characterization of the MRONJ patient population;
(6) consideration of bias control measures, including randomization and blinding when applicable;
(7) appropriateness, transparency and reproducibility of statistical analyses;
(8) clarity and completeness of outcome reporting, including adverse events and follow-up data;
(9) disclosure of funding sources and the potential conflicts of interest.
Each domain was scored dichotomously, with 1 indicating that the criterion was met and 0 indicating that it was not met, resulting in a total quality score ranging from 0 to 9. Based on their cumulative scores, the reviews were classified as having low (7–9 points), moderate (4–6 points), or high (0–3 points) risk of bias. Disagreement between the reviewers was resolved through discussion, and when necessary, arbitration by a fourth reviewer was undertaken. This quality assessment was conducted in accordance with the best-practice recommendations outlined in the Cochrane Handbook for Systematic Reviews of Interventions.51
This laser-adapted assessment approach was adopted to account for substantial heterogeneity in the laser systems, irradiation parameters and treatment protocols reported across MRONJ studies, which cannot be adequately captured by generic quality assessment tools.
It should be noted that the applied risk-of-bias tool is not formally validated, and was specifically developed to capture laser-related methodological and reporting characteristics, not fully addressed by the existing instruments, such as a measurement tool to assess systematic reviews 2 (AMSTAR-2). While this tailored approach enhances clinical relevance, it represents a methodological limitation. Future evidence syntheses may benefit from combining validated tools such as AMSTAR-2 with modality-specific assessment frameworks.
Results
Risk of bias and quality assessment
Upon using the predefined laser-adapted risk-of-bias assessment tool, most of the included reviews showed a balanced distribution of low and moderate risk of bias. However, relevant methodological limitations persisted, particularly incomplete reporting of laser parameters, limited use of randomized designs, and insufficient control of confounding factors, which should be considered when interpreting the findings (Table 2).
Characteristics of the included reviews
A total of 14 systematic reviews met the inclusion criteria and were incorporated into the analysis. These reviews encompassed a wide range of laser-based interventions, including PBMT, Er:YAG laser-assisted surgery, autofluorescence (AF)-guided techniques, and combined protocols, applied across different stages of MRONJ. The included evidence was derived mainly from observational studies, case series, and a limited number of comparative or randomized studies. The most frequently assessed outcomes were pain reduction, mucosal and bone healing, and overall clinical improvement. Despite frequent reporting of favorable trends, substantial heterogeneity in study design, laser parameters and outcome definitions limited direct comparison across the reviews. The included studies were categorized according to their primary clinical intent into preventive (peri-extraction or high-risk patient management) and therapeutic applications. Preventive applications, including the use of PBM in early-stage disease or high-risk patients, were addressed less frequently and were supported by a more limited and indirect evidence base as compared to therapeutic interventions. Therapeutic applications were further subdivided into non-surgical and laser-assisted surgical management, primarily using Er:YAG lasers for necrotic bone removal (Table 3).
Summary of laser parameters across modalities
Table 4 provides an overview of the core technical parameters that characterize the main laser modalities used in MRONJ management, linking physical settings to their intended clinical roles. For each approach – PBMT with red and near-infrared diodes, high-intensity Er:YAG surgical ablation, and combined Er:YAG plus PBMT protocols – the table summarizes typical wavelengths, power outputs, energy densities, delivery modes, and session frequencies, as reported in the included systematic reviews.
Presenting these ranges side by side highlights areas of relative consistency across the studies, while also underscoring domains in which substantial heterogeneity persists and currently precludes firm parameter standardization. Importantly, many included reviews reported outcomes qualitatively without standardized effect measures, which further limited the feasibility of constructing a reliable comparative visual map.
Summary of the results
Across the 14 reviews included in the final synthesis, laser-based interventions in MRONJ were evaluated in both preventive and therapeutic contexts, most commonly as adjuncts to surgical or conservative management. The reported outcomes primarily included pain reduction, mucosal healing, the resolution of the exposed bone, and improvement in soft tissue conditions, whereas hard clinical endpoints, such as complete disease resolution or recurrence, were less consistently assessed.
Where quantitative data was available within the included reviews, the reported outcomes showed variable but generally favorable ranges. Pain reduction was commonly described as clinically meaningful, with several reviews reporting significant decreases in pain scores following laser-based interventions. The soft tissue healing rates varied across the studies, but were frequently reported as improved as compared to baseline or conventional management. In surgical contexts, laser-assisted procedures were associated with effective necrotic bone removal and the facilitation of mucosal closure, although quantitative success rates were inconsistently reported. Variability in the reporting formats and outcome definitions precluded direct comparison across the studies; however, these ranges provide a general indication of clinical effectiveness.
Within the included reviews, 3 main domains of outcomes were identified: (1) pain reduction and symptom control; (2) soft tissue and mucosal healing; and (3) surgical outcomes, including necrotic bone removal and recurrence. Photobiomodulation therapy was predominantly associated with the alleviation of pain and improvement in soft tissue healing, particularly in early-stage disease and preventive settings. Er:YAG laser-assisted surgery was mainly applied in moderate-to-advanced MRONJ, and was associated with improved precision of necrotic bone removal and the facilitation of mucosal closure. Combined protocols integrating surgical and PBM approaches generally demonstrated favorable trends across the studies.
Overall, the evidence suggests favorable trends for combined laser-based approaches, particularly Er:YAG-assisted surgery with adjunctive PBMT. Direct comparison with conservative or medical management remains limited, and these observations should be interpreted with caution. Substantial heterogeneity in study design, laser parameters, outcome definitions, and follow-up duration further precluded quantitative comparison and limited the strength of conclusions regarding optimal treatment protocols.
It should be noted that the evidence regarding the preventive applications of laser-based therapies, particularly the use of PBM in early-stage disease or high-risk patients, remains limited and less consistently reported as compared to therapeutic interventions. Current interpretations in this area are based partly on indirect evidence and biological rationale, and therefore should be approached with caution. In addition, the potential overlap of primary studies across the included systematic reviews may have influenced the apparent consistency of the reported outcomes, and these findings should therefore be interpreted with appropriate caution.
Discussion
This consensus statement synthesizes the currently available systematic evidence on laser-based interventions in MRONJ management. Beyond summarizing the existing systematic reviews, the present study integrates heterogeneous evidence into a clinically interpretable framework distinguishing preventive, supportive (PBMT) and surgical laser applications. This structured interpretation enabled the formulation of consensus-based recommendations developed jointly by WFLD and PTSL.
Rationale – laser therapy
The application of laser-based therapies in MRONJ management is grounded in their established photobiological mechanisms that directly address the pathophysiological disturbances characteristic of this condition, including impaired angiogenesis, suppressed cellular metabolic activity, deficient bone remodeling, chronic inflammation, and compromised wound healing capacity.50, 51, 52, 53 Beyond its biological rationale, PBMT has also been incorporated into preventive clinical protocols for high-risk patients. Several clinical protocols support the preventive use of PBMT in patients undergoing tooth extraction, demonstrating a reduced incidence of MRONJ when PBMT is applied preoperatively in combination with antibiotic prophylaxis.14, 54, 55, 56, 57
Photobiomodulation therapy operates primarily through photochemical rather than photothermal mechanisms, targeting cytochrome c oxidase (CcO), the terminal enzyme in the mitochondrial respiratory chain. When photons at specific wavelengths (typically 600–1,100 nm) are absorbed by CcO, this interaction increases mitochondrial adenosine triphosphate (ATP) synthesis, modulates reactive oxygen species (ROS) production to therapeutic levels, and triggers downstream activation of multiple signaling cascades critical for tissue regeneration.18, 20, 21, 28, 58, 59, 60, 61 The cellular effects of PBMT on osteogenic cells are well documented. These mechanistic effects are supported by in vitro and in vivo evidence demonstrating improved fibroblast viability, the modulation of apoptotic signaling, enhanced angiogenic potential, and the promotion of osteogenic differentiation following PBMT exposure.18, 19, 58, 62 In osteoblasts, PBMT increases proliferation, ATP synthesis, mitochondrial activity, and osteoblastic differentiation in a dose-dependent manner, primarily mediated through moderate increases in intracellular ROS levels. Red laser wavelengths (particularly 635 nm) have been shown to induce vinculin-rich adhesion clusters, upregulate the expression of key osteogenic markers, including Runt-related transcription factor-2 (RUNX-2), alkaline phosphatase (ALP) and osteopontin (OPN), promote mineralized bone-like nodule deposition, and activate Akt signaling pathways that modulate bone matrix formation. These cellular responses translate into accelerated bone formation regardless of parameters or biomaterial use, though energy density emerges as the most critical variable.50, 52, 55, 56 Photobiomodulation therapy simultaneously enhances angiogenesis through multiple mechanisms, addressing the vascular compromise that characterizes MRONJ pathophysiology. Studies demonstrate that PBMT significantly enhances the expression of vascular endothelial growth factor (VEGF), bone morphogenic proteins (BMPs) and transforming growth factor-beta (TGF-β). The angiogenic effect operates through a ROS/hypoxia-inducible factor-1 alpha (HIF-1α)-dependent mechanism: PBMT triggers ROS accumulation, which in turn increases HIF-1α expression, subsequently upregulating VEGF and TGF-β, ultimately resulting in the formation of CD31hiEMCNhi (type H) vessels that couple angiogenesis with osteogenesis. This creates a positive feedback loop between ROS and HIF-1α that amplifies the pro-angiogenic response.56, 57, 59 The anti-inflammatory and immunomodulatory properties of PBMT represent another critical mechanism relevant to MRONJ management. Photobiomodulation therapy suppresses gene expression related to inflammation in osteoblasts, fibroblasts, human periodontal ligament cells, and endothelial cells. Specifically, both 810-nm diode and 1,064-nm Nd:YAG lasers significantly decrease the production of pro-inflammatory cytokines, including interleukin 6 (IL-6), IL-8, tumor necrosis factor-alpha (TNF-α), cyclooxygenase-2 (COX-2), and inducible nitric oxide synthase (iNOS), while reducing nuclear factor-kappa B (NF-κB) p65 phosphorylation and nuclear translocation. These effects are mediated through the activation of the AMP-activated protein kinase (AMPK)/sirtuin 3 (SIRT3) signaling axis, which facilitates both anti-inflammatory and antioxidative activity. Additionally, PBMT produces an initial upregulation of inflammatory mediators (IL-1, IL-6, IL-8, IL-18) and COX-2 at early time points (36 h to 3 days), followed by their decrease at 7 days, suggesting modulation rather than complete suppression of the inflammatory cascade necessary for proper healing.28, 60, 61, 63, 64 In addition to host-modulating effects, several laser systems exhibit direct antimicrobial activity against bacterial and fungal biofilms, which may contribute to infection control in compromised oral wounds.65, 66
Among the available laser systems, Nd:YAG laser irradiation has demonstrated pronounced antimicrobial and antifungal effects, particularly against mixed bacterial-fungal oral biofilms. In vitro studies have shown that Nd:YAG laser exposure significantly inhibits the growth of Candida albicans and Streptococcus mutans, as well as complex oral biofilms, suggesting a potential adjunctive role in reducing microbial burden in infected or compromised oral tissues.66, 67, 68, 69 The disinfection effects of the Nd:YAG laser are primarily attributed to a dominant photothermal mechanism, supplemented by a minor photomechanical component, which together disrupt biofilm architecture and compromise microbial cell integrity. The photothermal effect arises from the selective absorption of the laser energy (λ = 1,064 nm) by the pigmented chromophores within microbial cells or their surrounding medium, resulting in rapid and localized heat generation that leads to the thermal destruction of microorganisms. In cases where sufficient amount of energy is absorbed by the pigmented structures, a secondary photomechanical effect may occur, characterized by micro-explosions induced by rapid vaporization or plasma formation. These micro-explosions further contribute to the mechanical disruption of cellular structures. Importantly, the photomechanical component is contingent upon the adequate primary absorption of the laser energy. On the other hand, low-energy delivery typical of many Nd:YAG protocols may induce PBM in the exposed host cells, potentially stimulating cellular responses without causing thermal damage. Importantly, the microbiological landscape of MRONJ is dominated not only by common oral bacteria and fungi, but also by Actinomyces spp. Actinomyces spp. preferentially colonize the exposed necrotic bone, where compromised vascularization, impaired immune surveillance, and antiresorptive therapy-induced suppression of bone turnover create a favorable niche for persistent infection and biofilm maturation.24, 38, 44 Several studies have demonstrated a bactericidal effect of Nd:YAG laser irradiation against Actinomyces spp. In particular, Nd:YAG laser exposure has been shown to significantly reduce the viability of Actinomyces israelii in vitro. The antimicrobial activity of Nd:YAG lasers against Actinomyces appears to result from thermal protein denaturation, the disruption of bacterial cell walls, and photothermal damage to microbial membranes. Additionally, Nd:YAG irradiation has demonstrated bactericidal activity against oral bacteria within biofilm-like settings in vitro, particularly when used in combination with adjunctive antimicrobial agents, supporting its potential adjunctive role in microbial load reduction, which may be clinically relevant in MRONJ lesions characterized by persistent polymicrobial colonization.69 Although these findings are derived primarily from laboratory and adjunctive periodontal studies, they may be clinically relevant in MRONJ, where secondary bacterial and fungal colonization, particularly by Actinomyces spp., frequently complicates wound healing and disease control. Given the polymicrobial nature of MRONJ lesions and the frequent coexistence of bacterial and fungal biofilms, adjunctive antimicrobial laser effects may complement conventional surgical debridement, antiseptic measures and systemic antimicrobial strategies.
In parallel, recent evidence suggests that the biological effects of PBMT may be further modulated when combined with autologous fibrin-based biomaterials, such as platelet-rich fibrin (PRF). A systematic review by Bertoni Reis et al. reported that the combination of fibrin scaffolds and PBMT may enhance regenerative responses by influencing angiogenesis, fibroblast activity and extracellular matrix remodeling.70 The proposed mechanisms include improved cellular migration within the fibrin matrix, enhanced growth factor bioavailability, and mitochondrial stimulation induced by PBMT. Nevertheless, the available evidence supporting PBMT-PRF combinations remains limited predominantly to in vitro, animal, and small clinical observational studies, with substantial heterogeneity in laser parameters, biomaterial preparation protocols and clinical endpoints, precluding definitive clinical recommendations. Importantly, the increasing prevalence of antibiotic resistance highlights the need for localized drug delivery systems capable of minimizing systemic exposure. In this context, autologous platelet concentrates (APCs), including concentrated platelet-rich fibrin (c-PRF) and liquid-phase concentrated growth factors (LPCGFs), have additionally emerged as promising carriers for antimicrobial agents. Autologous platelet concentrates have demonstrated potential as localized delivery systems for antibiotics and antifungal agents. The selection between c-PRF and LPCGFs should be based on the physicochemical properties of the administered drug, as well as the intended clinical application. Overall, APCs represent a promising alternative for targeted antimicrobial therapy in both dental and surgical settings. Furthermore, the biological activity of PRF is highly dependent on its cytokine and growth factor profile, which may vary substantially according to the patient’s systemic inflammatory and immune status. In this context, PRF may exert either pro-regenerative or potentially pro-inflammatory effects, underscoring the need for careful patient selection and individualized assessment when considering combined PBMT-PRF protocols.70 Systemic inflammatory burden, which may be objectively assessed using complete blood count (CBC)-derived inflammation indices, has been proposed as a sensitive determinant of immune activity and cytokine balance, and may therefore critically influence the biological behavior of APCs. This is particularly important given the limited availability of data on primary bone turnover factors and patient-related biological variables that may influence regenerative outcomes, including vitamin D status, systemic inflammatory burden, and bone marrow characteristics in the maxilla and the mandible as assessed by cone-beam computed tomography (CBCT). These factors may be particularly relevant in the context of adjunctive therapies, such as PRF, as their biological activity is influenced by the patient’s systemic inflammatory and immunological status.71, 72, 73 Consequently, while this combined PBMT-PRF approach appears biologically promising, particularly in compromised healing environments like MRONJ, robust and well-controlled clinical trials are required before definitive therapeutic recommendations can be established. Importantly, the antimicrobial effects of laser irradiation, including Nd:YAG, should be interpreted as adjunctive and hypothesis-supporting rather than as definitive clinical evidence.
The Er:YAG laser operates at 2,940 nm, a wavelength that exhibits the highest degree of affinity for both water and hydroxyapatite, the primary constituents of soft and hard oral tissues. This characteristic enables the precise ablation of necrotic bone tissue through photothermal vaporization while minimizing collateral thermal damage to the surrounding viable structures.24, 38, 44, 74 Er:YAG laser surgical debridement offers multiple advantages over conventional rotary instrumentation for MRONJ management. Scanning electron microscopy (SEM) and micro-computed tomography (micro-CT) demonstrate that Er:YAG laser creates biologically open cut surfaces with preserved trabecular architecture and minimal mechanical damage, whereas conventional drilling produces trabecular collapse, a flattened smear layer that occludes marrow spaces, reduced porosity at the margins, and histological evidence of thermal damage. Laser-mediated cutting preserves marrow exposure at the margins, facilitating cellular infiltration and likely accelerating healing, while mechanical drilling restricts cellular passage and causes localized cell death through thermal injury.75, 76, 77, 78 The Er:YAG laser demonstrates superior bactericidal efficacy as compared to conventional mechanical debridement. The laser ablates periodontopathic bacteria, including Porphyromonas gingivalis and Aggregatibacter actinomycetemcomitans, through thermal vaporization at energy densities as low as 0.3 J/cm2. In chronic wound management, Er:YAG debridement significantly reduces bacterial load both immediately (27.3% to 59.1% in low/negative category; p = 0.04) and sustains this reduction for 1 week post-treatment, whereas sharp debridement shows no sustained antibacterial effect. This is particularly important given the limited availability of data on primary bone turnover factors, such as vitamin D status, systemic inflammatory burden, or the presence of bone marrow adiposity in the maxilla and the mandible as assessed by CBCT, in the analyzed studies.35, 79, 80, 81, 82, 83, 84 From a procedural standpoint, the Er:YAG laser enables more conservative and precise osteotomy. The laser removes significantly more bone tissue in shorter time as compared to conventional drills, generates significantly less heat, produces regular cavities with sharp edges and knife-like cuts without bone fragments or debris, and creates minimal thermal alterations limited to a 30-μm sublayer. These characteristics reduce postoperative pain and decrease facial swelling.85, 86, 87, 88, 89 Beyond its cutting efficiency, Er:YAG laser application has also been associated with reduced aerosol generation, improved surgical field control, and favorable safety profiles when appropriate protocols are followed.90, 91 A critical challenge in MRONJ surgical management is the accurate intraoperative identification of necrotic vs. viable bone margins. Autofluorescence-guided surgery addresses this limitation by exploiting the natural fluorescence properties of viable bone tissue.44, 92, 93, 94 When irradiated with ultraviolet or blue light (400–405 nm), viable bone exhibits strong fluorescence, whereas necrotic bone shows marked loss of fluorescence and appears dark. This phenomenon is attributed to fluorescence-emitting amino acids within collagen molecules, which are depleted or structurally altered in necrotic tissue. Quantitative spectrophotometric analyses have demonstrated a significantly higher fluorescence signal in viable bone as compared to necrotic areas, corresponding to a mean loss of fluorescence intensity ratio of approx. 5:1. Histopathological correlation studies further validate the clinical relevance of AF guidance, showing that fluorescence-positive bone is characterized by substantially higher osteocyte density, greater collagen type I content, and increased proportions of immature regenerating bone as compared to fluorescence-negative areas.85, 86, 87, 88, 89, 90, 91, 92, 93, 94, 95, 96, 97, 98, 99, 100, 101, 102, 103, 104, 105, 106, 107, 108, 109 Importantly, the histological evaluation of hyperfluorescent bone specimens collected at the margins of necrotic lesions consistently confirms the presence of viable bone tissue, supporting the reliability of AF as a real-time intraoperative tool for defining surgical resection boundaries.110, 111, 112, 113, 114, 115
The most clinically relevant effects are observed in combined laser protocols, where synergistic mechanisms can be leveraged. Emerging clinical evidence suggests that combined protocols integrating Er:YAG laser surgery with adjunctive PBMT may provide synergistic benefits, supporting both effective necrotic tissue management and enhanced post-operative healing.95, 96 The most successful clinical outcomes in MRONJ management are reported when Er:YAG laser surgical ablation is combined with adjunctive PBMT. This combination addresses both the need for the precise surgical removal of necrotic tissue and the requirement for enhanced biological healing capacity in the remaining viable bone and soft tissues.12, 97, 98, 99 The Er:YAG laser component provides precise debridement, bactericidal effects and the preservation of bone architecture, while the PBMT component enhances cellular proliferation, promotes angiogenesis, modulates inflammation, and accelerates both soft tissue and bone healing. In a single cohort study, this multimodal approach was associated with complete mucosal healing in 87.5% of cases at a mean follow-up of 13 months; however, this finding should be interpreted with caution and cannot be generalized due to the limited evidence base.82 When combined with AF guidance, Er:YAG laser ablation allows controlled, stepwise removal of necrotic bone under real-time AF visualization, facilitating the preservation of viable hyperfluorescent bone while ensuring adequate debridement. This approach combines the precision of AF-guided margin identification with the biological advantages of laser ablation, potentially optimizing the balance between sufficient debridement and the preservation of viable bone stock.85
It should be emphasized that PBMT follows a biphasic dose-response relationship, and inappropriate energy density or treatment frequency may reduce therapeutic efficacy or result in null effects, which may partially explain inconsistent clinical outcomes reported in the literature.
Stage-adapted role of laser therapies in MRONJ
The synthesis of the available evidence indicates that the clinical role of laser-based therapies in MRONJ should be interpreted in a stage-adapted but surgically oriented framework, rather than as a uniform intervention. Contemporary international guidelines and surgical literature increasingly support the early surgical management of the exposed necrotic bone, even in the absence of overt infection, provided that the patient’s general condition allows for intervention. Photobiomodulation therapy has also been proposed as a supportive modality in early-stage disease and preventive contexts. Evidence from oncology-related clinical practice guidelines supports the use of PBMT as part of routine care for oral mucosal healing and the prevention of treatment-related complications. Although these indications are not specific to MRONJ, they provide a biological and clinical rationale for considering PBMT in the preventive or early-stage management of MRONJ. Nevertheless, direct evidence in MRONJ prevention remains limited, and extrapolation from other clinical settings should be interpreted with caution. In early-stage disease (stage 0–1), PBMT may be used as an adjunct to reduce pain, control inflammation and support mucosal healing; however, it should not be regarded as a stand-alone alternative to surgical treatment. Importantly, minimally invasive surgical approaches, including Er:YAG laser-assisted debridement, have been shown to be appropriate and biologically justified already in stage 1 MRONJ. The Er:YAG laser enables the selective and gentle evaporation of necrotic bone with minimal thermal damage to the surrounding viable tissue, which is particularly relevant in early disease, where the preservation of bone vitality and the promotion of soft-tissue closure are critical. In advanced stages (stage 2–3), laser-assisted surgical approaches play a complementary role within a more extensive surgical strategy. In these cases, Er:YAG laser surgery may enhance the precision of necrotic bone removal, improve access to irregular defects, reduce bacterial contamination, and facilitate tension-free mucosal closure, while conventional surgical principles remain the cornerstone of treatment. Laser-based modalities in MRONJ should be regarded as adjunctive tools integrated into a stage-adapted surgical treatment concept, rather than as substitutes for surgery. Their optimal use depends on accurate staging, careful patient selection, and a clear distinction between supportive biological effects (e.g., PBMT) and definitive surgical objectives (e.g., the removal of necrotic bone). Autofluorescence-guided surgery further supports intraoperative decision-making by assisting in the identification of viable bone margins; however, current evidence remains limited to non-randomized studies. This stage-dependent interpretation is essential to avoid the overgeneralization of laser efficacy across heterogeneous clinical scenarios.
Limitations of the evidence
Despite the growing body of literature supporting laser-based therapies in the prevention and management of MRONJ, the overall quality and strength of the available evidence remain limited. A principal limitation is substantial heterogeneity across the studies with respect to laser modalities, wavelengths, power outputs, energy densities, application techniques, treatment duration, and the number of sessions. This variability prevents meaningful comparison between the studies and significantly limits the feasibility of quantitative synthesis or protocol standardization. Given the pronounced heterogeneity in the reported laser protocols, full reporting of the operating parameters should be considered mandatory to ensure reproducibility and meaningful comparison between the studies.94 Outcome reporting was also inconsistent. While pain reduction, usually assessed using the visual analog scale (VAS), was frequently reported, other clinically relevant outcomes, such as the extent of bone healing, mucosal coverage, radiographic bone regeneration, lesion recurrence, and disease-free survival, were variably defined or omitted. In addition, outcome definitions and staging systems for MRONJ were not uniformly applied across the studies and reviews, and some studies failed to stratify outcomes by disease severity, further complicating interpretation, limiting cross-study comparability and precluding stage-specific quantitative synthesis. Another critical limitation is the predominance of small sample sizes and non-randomized study designs. Many included studies were observational, retrospective, or case series in nature, with limited control groups and inadequate adjustment for confounding factors, such as systemic disease, medication type and duration, or concomitant therapies. Follow-up periods were frequently short, often limited to weeks or a few months, which is insufficient to assess long-term stability, recurrence or progression of MRONJ. These limitations reinforce the view that current recommendations for laser-based interventions in MRONJ should be interpreted as conditional and context-dependent, emphasizing their role as adjunctive rather than stand-alone therapies within comprehensive, stage-adapted management strategies. Safety reporting was inconsistent and often incomplete. Although serious adverse effects related to laser therapy were rarely described, the absence of standardized reporting limits definitive conclusions regarding long-term safety. Collectively, these limitations underscore the need for well-designed, adequately powered randomized controlled trials (RCTs) with standardized laser protocols, uniform outcome measures and extended follow-up periods.
Limitations of the review process
This consensus statement study was conducted in accordance with the established methodological standards; however, several limitations related to the review process itself should be acknowledged. First, the search strategy was restricted to English-language publications, which may have resulted in language bias and the exclusion of potentially relevant evidence published in other languages. This is particularly relevant in the field of laser therapy, where clinical experience may be reported in non-English literature. However, this approach was adopted to ensure methodological consistency, reproducibility, and the reliability of data extraction and interpretation across the reviewers. Second, gray literature, including conference proceedings, theses and unpublished data, was not taken into consideration, increasing the risk of publication bias toward studies with positive findings. The number of eligible systematic reviews and meta-analyses was relatively limited, and substantial heterogeneity existed among them in terms of inclusion criteria, laser modalities assessed, outcome definitions, and methodological quality. These factors precluded the conduct of a higher-level quantitative synthesis and constrained comparisons across laser types. Although screening, data extraction and quality assessment were performed independently by multiple reviewers to minimize subjectivity, some degree of interpretive bias may persist, particularly in the evaluation of methodological rigor and outcome relevance. Additionally, the absence of individual patient-level data restricted subgroup analyses based on MRONJ stage, medication exposure or patient-specific risk factors. These limitations highlight the importance of improved transparency, standardized reporting and harmonized methodologies in future evidence syntheses. An additional methodological limitation of this review is that the overlap of primary studies across the included systematic reviews was not formally quantified using a citation matrix or the corrected covered area analysis. Since many reviews addressed partially overlapping clinical questions while differing in inclusion criteria, intervention scope and outcome definitions, some degree of duplication of the underlying evidence is likely. This may have contributed to the overrepresentation of certain findings and influenced the apparent consistency of the reported outcomes. Therefore, the observed trends across the reviews should be interpreted with caution, particularly when similar results are reported across multiple sources.
Implications for practice, policy making, and future research
From a clinical perspective, the available evidence supports the use of laser-based therapies as adjunctive tools rather than standalone treatment in MRONJ management. From a practical perspective, the implementation of laser-based therapies may be influenced by resource availability and economic considerations. The use of advanced laser systems requires dedicated equipment, maintenance and clinician training, which may limit accessibility in certain clinical settings. While PBMT is increasingly recognized and supported by procedural coding systems in some healthcare frameworks, access to laser technologies as well as reimbursement policies remain variable across regions and clinical environments. These factors should be considered when integrating laser-based interventions into routine clinical practice, particularly in resource-limited settings. This is particularly relevant given the growing clinical adoption of PBMT and its inclusion in selected clinical guidelines and reimbursement frameworks.
Photobiomodulation therapy appears beneficial for pain reduction, inflammation control and the enhancement of soft tissue healing across the full spectrum of MRONJ stages, including early disease, advanced lesions and palliative settings. In patients with advanced MRONJ, immunocompromised status, active malignancy, poor performance status, or limited life expectancy, PBMT may represent a valuable supportive option to reduce pain, decrease reliance on repeated antibiotic cycles, and improve QoL, with a favorable safety profile and no clinically relevant contraindications reported.
Er:YAG laser-assisted surgery and AF-guided techniques show promise in improving surgical precision, facilitating the selective removal of necrotic bone, and supporting mucosal healing, particularly when integrated into stage-adapted surgical strategies. However, clinicians should exercise caution and integrate laser therapies within comprehensive, multidisciplinary stage-adapted treatment plans, rather than applying them as isolated interventions. At the policy level, current evidence does not yet justify universal guideline mandates for laser therapy in MRONJ, but supports conditional recommendations for their adjunctive use in specialized centers with appropriate surgical and laser expertise. Standardized training, credentialing, and structured reporting frameworks are necessary to ensure safe, reproducible and effective implementation.
Future research priorities include the development of consensus-driven laser protocols with clearly defined parameters, standardized outcome sets and harmonized reporting guidelines. A major limitation of current laser applications in MRONJ remains the wide variability in the irradiation parameters, treatment frequency and the number of clinical sessions, which substantially limits inter-study comparability. Notably, similar challenges affect laser applications in periodontology, peri-implantitis, PBM for orofacial pain, and temporomandibular joint disorders, underscoring that this limitation reflects the broader field of medical laser therapy rather than MRONJ-specific shortcomings.wstawić jako nowy akapit:
Additionally, it is crucial to consider the patient’s general condition when planning local treatment, including factors such as the body mass index (BMI), insulin resistance, the immune system status, and other parameters related to bone metabolism, including vitamin D levels.115 These systemic conditions may significantly influence local healing processes and can markedly affect the final therapeutic outcomes.
Large, multicenter RCTs with long-term follow-ups are essential to determine the comparative effectiveness, cost-efficiency and optimal integration of laser therapies across MRONJ stages. Additionally, mechanistic studies linking clinical outcomes with biological endpoints may further clarify patient selection criteria and refine therapeutic indications, and support the rational incorporation of laser-based adjuncts into evidence-informed clinical guidelines.
Conclusions
Given the substantial heterogeneity of study designs, laser parameters and outcome measures, the recommendations derived from the available evidence should be regarded as conditional rather than definitive, and interpreted within a multimodal, stage-adapted treatment framework. Evidence from systematic reviews nevertheless suggests potential benefits in terms of pain reduction, enhancement of soft tissue healing, improved surgical precision, and higher rates of mucosal closure, particularly when lasers are used as part of combined treatment protocols. However, the current evidence base remains limited by methodological weaknesses and insufficient long-term data. Therefore, the reported clinical benefits should be interpreted with caution, particularly when extrapolating outcomes from preventive or early-stage settings to advanced MRONJ requiring surgical management. At present, the most evidence-supported role of laser therapy in MRONJ lies in its integration into multimodal, stage-adapted treatment strategies rather than as an isolated therapeutic intervention. Importantly, when applied within the established safety parameters, laser-based adjunctive therapies, particularly PBM, have demonstrated a favorable safety profile, with an absence of clinically relevant side effects and no recognized contraindications reported in the available literature. Continued high-quality research, protocol standardization and rigorous outcome reporting are required to strengthen the evidence base and inform the development of definitive, evidence-based clinical guidelines. Laser-based therapies represent a valuable adjunct in the contemporary management of MRONJ. Importantly, the present review moves beyond traditional evidence synthesis by integrating the available literature into a stage-adapted clinical framework and consensus-based recommendations developed by WFLD and PTSL.
Consensus-based clinical guidance from the World Federation for Laser Dentistry (WFLD) and the Polish Society for Laser Dentistry (PTSL)
All recommendations are classified as conditional due to the limited certainty of the available evidence. Upgrading to strong recommendations would require consistent findings from adequately powered RCTs, standardized laser protocols and robust long-term data on clinically relevant outcomes, including recurrence and malignant transformation.
These recommendations were developed based on a structured synthesis of systematic reviews and meta-analyses, and reflect expert consensus. A key objective of this section is to translate the heterogeneous evidence base into a structured, stage-adapted clinical framework for laser-assisted MRONJ management, distinguishing preventive, supportive and surgical indications. Given the heterogeneity and overall moderate-to-low quality of the available evidence, these recommendations should be interpreted as conditional and intended to support, rather than replace, established MRONJ management strategies. This is particularly important given the limited availability of data on primary bone turnover factors, such as vitamin D status, systemic inflammatory burden assessed by biochemical markers, or the presence of bone marrow adiposity in the maxilla and the mandible as assessed by CBCT, in the analyzed studies.73, 100 Importantly, laser-based interventions in MRONJ should be interpreted according to the primary clinical intent: (a) prevention (peri-extraction/preoperative risk reduction in high-risk patients); and (b) treatment of established MRONJ, further subdivided into non-surgical supportive PMB (PBMT) and laser-assisted surgical management (primarily Er:YAG), optionally guided by AF. Laser-based interventions in MRONJ should be performed by clinicians with formal training in both MRONJ management and laser safety. Appropriate eye protection, adherence to laser safety standards and careful patient selection are mandatory, particularly in oncological patients with complex comorbidities. Clinical laser application in MRONJ is schematically illustrated in Figure 2.
General therapeutic principles
1. Stage-adapted care provides an important framework, but should not be applied rigidly. While MRONJ staging (e.g., AAOMS or equivalent classifications) remains a useful reference, therapeutic decisions should not be based on the disease stage alone. Laser therapy should therefore be integrated into an individualized, stage-informed treatment strategy, and should not be used as a universal replacement for the established conservative or surgical protocols.
2. Patient selection and risk stratification are essential. Medication-related osteonecrosis of the jaw represents a heterogeneous clinical condition, and treatment decisions must be made on a case-by-case basis, taking into account the underlying indication for antiresorptive or antiangiogenic therapy, the route and duration of drug exposure, the oncological status, age, systemic comorbidities (e.g., diabetes, immunosuppression), local infection and inflammatory burden, the anatomical extent of the disease, and the feasibility of close clinical follow-up.
3. Across all disease stages, infection control and wound stability remain core therapeutic objectives. Laser-based modalities should be considered adjuncts to the established standard measures, including local antisepsis, systemic antibiotics when clinically indicated, the optimization of oral hygiene, and adherence to sound surgical principles where required.
4. Claims of “curative efficacy” should be avoided in the absence of robust, controlled comparative evidence. The current body of literature primarily supports the adjunctive benefits of laser therapies, such as pain reduction, the enhancement of soft tissue healing, the facilitation of mucosal coverage, and improved outcomes when incorporated into combined, multimodal treatment protocols, rather than definitive curative effects.
5. Photobiomodulation therapy can be safely applied across all MRONJ stages and patient profiles, including oncological, immunocompromised and frail individuals, as it is associated with a favorable safety profile and the absence of relevant contraindications. Its short treatment duration and non-invasive nature further support its use in patients with limited tolerance for prolonged or invasive procedures.
6. Photobiomodulation therapy follows a biphasic dose-response relationship, consistent with the Arndt-Schulz law (hormesis), which describes stimulation at low doses and inhibition at higher doses, as demonstrated in PBM research. Moreover, the available evidence suggests that therapeutic effects are dose-dependent, with lower doses often promoting cellular proliferation and tissue repair, while excessive energy delivery possibly attenuating these effects. In clinical practice, this underscores the importance of appropriate parameter selection, as both insufficient and excessive energy delivery may compromise therapeutic outcomes.18, 22, 58, 101
Intent-Based Recommendations (Prevention vs. Treatment)
Prevention (peri-extraction and preoperative risk reduction)
Recommendation (conditional): Consider PBMT as part of perioperative risk-reduction protocols in high-risk patients undergoing tooth extraction, particularly when combined with standard infection prophylaxis and atraumatic surgical techniques.
Good practice points:
– PBMT should not be a standalone preventive “guarantee”; it should be integrated within risk-reduction protocols (antisepsis, antibiotic prophylaxis when indicated, primary closure where feasible, and close follow-up);
– Where preventive PBMT is implemented, the protocol (wavelength, fluence, the number of points, the session schedule) must be explicitly documented to enable reproducibility and audit.
Treatment of established MRONJ – non-surgical supportive PBMT
Recommendation (conditional): PBMT may be used as a supportive modality to reduce pain and inflammation and to promote soft tissue healing, particularly in early-stage disease or as preoperative support.
Key limitation statement (as in oral lichen planus (OLP) guidance): PBMT is best interpreted as supportive rather than definitively curative in advanced MRONJ when used as monotherapy.
Treatment of established MRONJ – laser-assisted surgery (Er:YAG ± AF)
Recommendation (conditional): In patients requiring surgical debridement/resection, Er:YAG may be considered as an adjunct to conventional instrumentation for necrotic bone removal and bacterial decontamination, with the objective of minimizing thermal damage and supporting mucosal closure.
Recommendation (conditional): AF-guided surgery may be considered to assist in the intraoperative identification of viable bone margins, particularly in complex or advanced cases; however, evidence remains limited and should be interpreted cautiously.
Combined protocols (Er:YAG + peri-operative PBMT, AF optionally integrated)
Recommendation (conditional, preferred integration strategy): When feasible, multimodal protocols combining Er:YAG laser debridement with perioperative PBMT, optionally supported by AF-guided surgery, should be prioritized over isolated laser use, as combined approaches are most consistently associated with favorable mucosal healing and clinical improvement.
Minimal documentation standards
All cases should include standardized documentation of the following elements:
– MRONJ classification and treatment intent: MRONJ staging system used (e.g., AAOMS or equivalent); anatomical location; and primary clinical intent (prevention vs. treatment – non-surgical vs. surgical);
– patient-related systemic characteristics and medication exposure: age; sex; relevant comorbidities (e.g., obesity and its metabolic complications, such as diabetes mellitus, hyperlipidemia, metabolic dysfunction-associated steatotic liver disease (MASLD), hypertension, as well as immunosuppression); oncological status; performance status where applicable; and detailed drug history, including the type of antiresorptive and/or antiangiogenic agent, the route of administration, the cumulative dose, the duration of therapy, the timing of the last dose, and concomitant medications affecting bone turnover (e.g., corticosteroids, chemotherapy, and targeted therapies), as well as factors influencing bone metabolism, such as vitamin D levels;
– radiographic diagnostics, including CBCT, computed tomography (CT) or magnetic resonance impaging (MRI), performed to assess the extent of necrosis, the proximity of the adjacent anatomical structures, and bone density for the presence of bone marrow steatosis116;
– all laser treatment parameters: wavelength; power; emission mode (continuous or pulsed); spot size or fiber/tip diameter; fluence or energy per point; exposure time per point; number of points treated; session duration; number and frequency of sessions; and use of adjuncts, such as irrigation, cooling or photosensitizer when applicable;
– co-interventions and procedural details: antisepsis protocol; antibiotic therapy (agent, dose, duration); surgical technique (extent of debridement, resection margins, closure strategy); and any additional adjunctive therapies;
– core clinical outcomes (minimum dataset): pain assessment (VAS or the numerical rating scale (NRS)); mucosal coverage or closure; presence or resolution of the exposed bone or fistula; signs of infection or suppuration; need for re-intervention; and duration of follow-up (recommended ≥6–12 months to assess stability and recurrence whenever possible).
Safety considerations and clinical precautions
Operator competency: Laser based interventions should be performed by clinicians with formal laser safety training and documented competency in MRONJ conservative and surgical management.
Mandatory safety measures: Appropriate eye protection for the patient and the staff, a controlled clinical environment, and strict adherence to manufacturer-specific safety recommendations are mandatory.
It is important to recognize that MRONJ encompasses 2 clinically distinct patient populations, whose risk profiles, disease progression and therapeutic considerations differ substantially. Patients receiving high-dose antiresorptive or antiangiogenic therapy for malignant diseases, most commonly bone metastases or multiple myeloma, represent a higher-risk group characterized by more advanced and treatment-refractory lesions, greater systemic vulnerability, and more complex comorbidity profiles, including immunosuppression, concomitant chemotherapy and reduced functional reserve. In contrast, patients receiving low-dose oral bisphosphonates for osteoporosis generally present with earlier-stage disease, lower rates of progression, and a more favorable response to conservative and adjunctive laser-based therapies.
Beyond the distinction between oncological and osteoporotic populations, important differences among specific drug classes should also be considered. Bisphosphonates exert prolonged skeletal effects because of their high affinity for hydroxyapatite and extended retention within bone tissue, whereas denosumab, a RANKL inhibitor, demonstrates a more reversible pharmacological profile following treatment discontinuation. These differences may influence both the timing and the biological response to laser-assisted interventions. Antiangiogenic agents introduce an additional and distinct mechanism of tissue injury through vascular compromise, which may attenuate the proangiogenic effects of PBMT, and therefore requires particular caution when interpreting treatment outcomes in this subgroup.
In addition, the present recommendations should be interpreted in the context of the patient’s current treatment status, as the biological environment and healing potential may differ substantially between patients actively receiving antiresorptive or antiangiogenic therapy and those in whom treatment has been temporarily or permanently discontinued before or after the onset of MRONJ. These distinctions are not consistently addressed in the current literature, and represent an important area for future stage- and drug-specific investigations.
Finally, the management of MRONJ, including decisions regarding the initiation, continuation or interruption of the causative medication, should be undertaken within a multidisciplinary framework. Close collaboration with the treating oncologist, hematologist, rheumatologist, or other relevant specialist responsible for antiresorptive or antiangiogenic therapy is essential to ensure that laser-based interventions are integrated into a comprehensive and individualized treatment plan that appropriately balances oncological or metabolic treatment goals with oral health outcomes.
Research and standardization needs
The WFLD and PTSL emphasize the need for:
– well-designed comparative trials taking into account the patient’s general condition (PBMT vs. standard care; Er:YAG vs. conventional surgery; combined protocols vs. monotherapy);
– standardized dosimetry reporting and harmonized outcome measures;
– stage-specific analyses and longer follow-up (≥12 months) to assess recurrence and durability; and
– cost-effectiveness and patient-reported outcomes.
Trial registration
The study was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD420251269761).
Ethics approval and consent to participate
Not applicable.
Data availability
All data for this study is included within the article.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
AI-assisted tools were used exclusively for language editing and the improvement of readability. No AI tools were used for data analysis, interpretation, or the generation of scientific conclusions. All content was reviewed and approved by the authors.