Abstract
Background. Pain is one of the most fundamental yet complex human biological experiences. A distinct category within this domain is orofacial pain. The orofacial region is anatomically complex, comprising a dense network of muscles, nerves and blood vessels. This complexity often makes the diagnosis and management of conditions affecting this area particularly challenging for clinicians.
Objectives. The primary aim of this study was to determine the global prevalence of oral and facial pain in the general population and to assess its distribution across different continents.
Material and methods. Literature searches were conducted in the MEDLINE and Scopus databases. This analysis synthesized data from 155 observational studies published between 2004 and 2024, encompassing 1,712,161 participants and 163,154 reported cases. Statistical analyses were performed using the R statistical language.
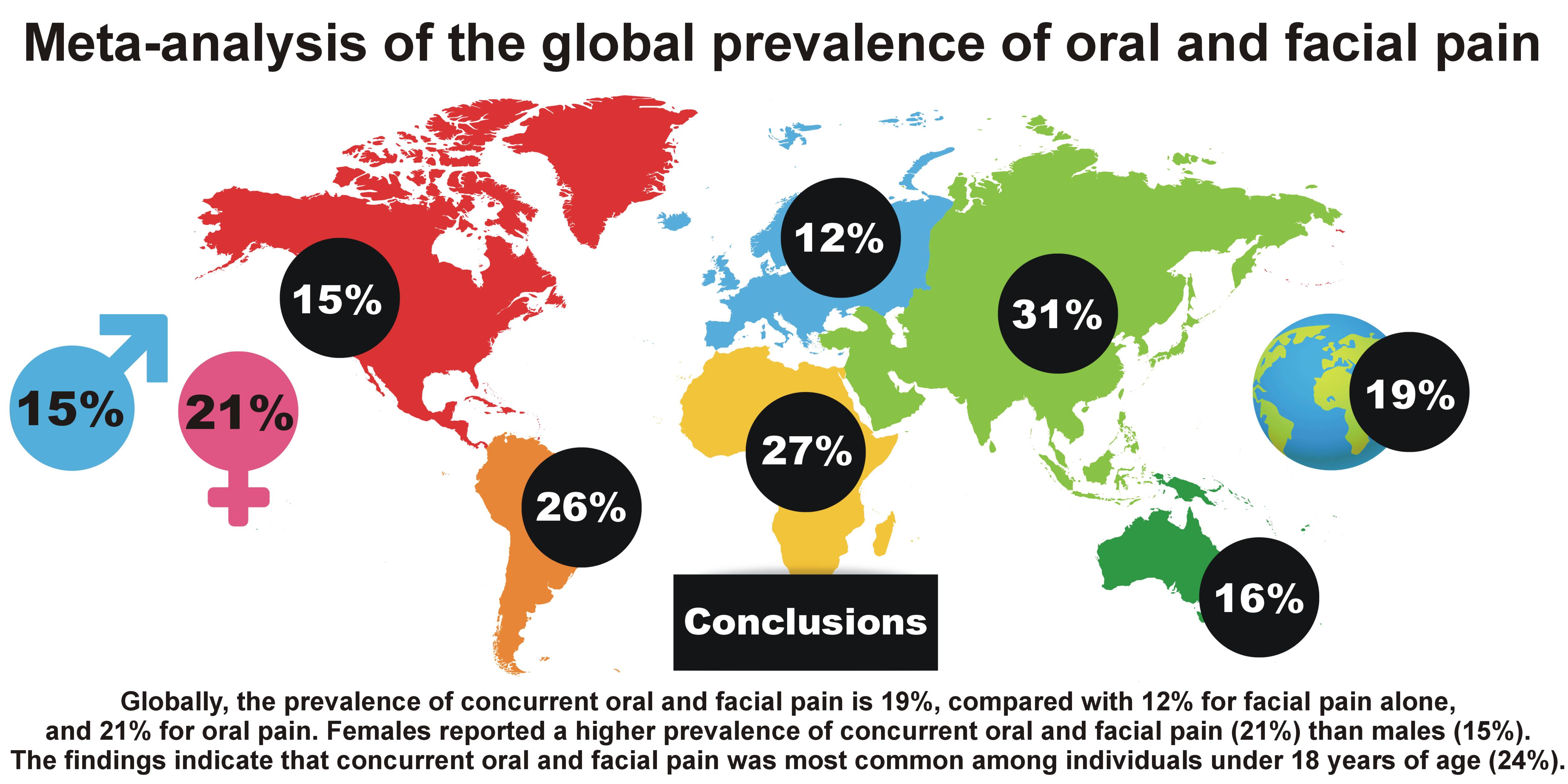
Results. The pooled global prevalence of concurrent oral and facial pain was 19.19%. By continent, the prevalence rates were as follows: Africa – 27.44%; Asia – 30.78%; Australia – 15.58%; Europe – 12.27%; North America – 14.53%; and South America – 25.61%.
Conclusions. Globally, the prevalence of concurrent oral and facial pain is 19%, compared with 12% for facial pain alone, and 21% for oral pain. Concurrent oral and facial pain was most common among individuals under 18 years of age (24%), decreasing to 16% among those aged 18–60 years and 10% in those aged >60 years. Females reported a higher prevalence (21%) of oral and facial pain than males (15%). Overall, the burden of concurrent oral and facial pain is greatest in Asia and South America, particularly among females, where prevalence exceeds 28%, while the lowest rates are found in Europe, especially among males (8%). The results of the present study should be interpreted with caution due to the high heterogeneity of the included studies. Further epidemiological research is recommended, employing rigorous methodology and adhering to current pain classification systems.
Keywords: prevalence, epidemiology, sex, orofacial pain, facial
Introduction
Pain is one of the most fundamental yet complex human biological experiences.1, 2 The International Association for the Study of Pain (IASP) defines it as “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage”.3 Pain is not merely a reaction to nociceptive stimuli but a multidimensional process integrating biological, psychological and social components.1, 2, 3, 4
In the context of the present work, it is essential to clearly distinguish between 3 related but distinct terms: “oral pain”; “facial pain”; and “orofacial pain”. Oral pain refers specifically to pain experienced within the structures of the oral cavity (e.g., teeth, gingiva, mucosa, tongue), while facial pain describes discomfort perceived in the facial region outside the mouth, such as the cheeks, jaw or periorbital area.5, 6 Orofacial pain, as used in the present study, is an overarching term that encompasses both oral and facial pain, irrespective of whether its origin is dental, musculoskeletal, neuropathic, or idiopathic.7, 8
Orofacial pain represents a distinct clinical category due to the anatomical complexity of the orofacial region, which contains a dense network of muscles, nerves and blood vessels. This complexity often makes the diagnosis and treatment of conditions affecting this area challenging for clinicians.7, 8 The IASP defines orofacial pain as a frequent form of pain perceived in the face and/or oral cavity.9 While facial pain of oral origin is commonly associated with intraoral dental or periodontal pathologies, differential diagnostic challenges arise when pain originates from other sources, such as temporomandibular disorders (TMD) or neuropathic pain.10 Therefore, the distinction between oral, facial and orofacial pain is not only terminological but also clinically significant, as it affects diagnostic strategies and therapeutic approaches.
Patients experiencing orofacial pain often present with impaired mental health, elevated anxiety levels, depression, and perceived stress, all of which significantly impact quality of life.11, 12 Beyond its high prevalence, the clinical significance of orofacial pain lies in its potential to cause long-term disability, reduced masticatory function, impaired communication, and psychosocial burden. Chronic orofacial pain contributes to sleep disturbances, reduced work productivity and increased healthcare utilization, making it a relevant public health issue.13, 14
Ethnic and cultural variations in pain perception constitute a significant area of investigation in pain medicine and health psychology.15, 16 Multiple studies have demonstrated that ethnic groups may differ in both pain threshold and pain tolerance, stemming from a combination of biological, psychological and sociocultural factors. Genetic predispositions may influence the functioning of nociceptive and pain-modulating systems, whereas cultural norms and behavioral patterns shape how individuals express or suppress pain-related complaints.1, 17, 18, 19 In addition to ethnic and cultural determinants, sex has been demonstrated to play a role in orofacial pain perception; estrogen levels have been shown to be associated with pain modulation in the temporomandibular joint and the orofacial region as a whole.20, 21
Recent evidence indicates substantial variation in the prevalence of orofacial pain across populations and regions. A systematic review conducted by Porporatti et al. reported that, in adults, the prevalence of pain in the oral and facial regions ranges from approx. 1% in burning mouth syndrome to over 80% in orofacial pain associated with cancer treatment. In pediatric populations, the prevalence varies from below 1% for temporomandibular joint osteoarthritis up to 83% for all types of headaches.22 Another study reported that 19% of individuals with dementia experience orofacial pain.23 Two meta-analyses published in 2024 identified regional differences in the prevalence of TMD and bruxism.24, 25 The prevalence of TMD was significantly higher in South America (47%) compared to Asia (33%), Europe (29%) and North America (26%).24 Additionally, the prevalence of bruxism (sleep and awake) was reported as 29% in North America, 25% in South America, 22% in Europe, and 19% in Asia.25 Further differences were observed in a meta-regression analysis examining the co-occurrence of bruxism and TMD.26
However, despite numerous studies addressing individual conditions such as TMD or bruxism, comprehensive population-based data on the global prevalence of orofacial pain as a unified entity remains limited. Previous meta-analyses have focused on specific disorders rather than the overall pain experience, leaving uncertainty regarding how orofacial pain differs across continents and demographic groups.
The present study aims to address this gap by providing the first meta-analytic estimate of the global and continental prevalence of orofacial pain in the general population. A secondary objective is to assess differences in prevalence according to age and sex. The working hypothesis of this study is that the global prevalence of orofacial pain does not exceed 30%. Clarifying these patterns is clinically relevant for identifying at-risk populations, guiding resource allocation, and improving culturally sensitive pain management strategies. Furthermore, establishing reliable prevalence data will support health policymakers in prioritizing early diagnosis and preventive care within dental and primary healthcare systems.
Material and methods
Building upon previously published and varied methodologies,27, 28, 29, 30 the first stage involved registering the project with the Open Science Framework (OSF) repository (https://osf.io/c8x2d). The project was registered on February 19, 2025, marking the official commencement of the research. The supplementary materials related to this study were made available in the OSF repository (https://osf.io/k7eds/files).
The study was conducted in accordance with the 2020 PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines.31 Literature searches were performed in 2 databases: MEDLINE and Scopus. The following keyword combinations were applied:
• “orofacial pain” AND “prevalence”;
• “orofacial pain” AND “epidemiology”;
• “orofacial pain” AND “population”;
• “facial pain” AND “prevalence”;
• “facial pain” AND “epidemiology”;
• “facial pain” AND “population”;
• “oral pain” AND “prevalence”;
• “oral pain” AND “epidemiology”;
• “oral pain” AND “population”.
In line with previous publications,25, 29 the analysis was restricted to studies published within the last 20 years, covering the period from January 1, 2004, to December 31, 2024.
The study design followed the PICO framework,32, 33 enabling the formulation of precise research questions and systematic data analysis:
• P (Population): individuals worldwide reporting orofacial, oral or facial pain, regardless of age or sex;
• I (Intervention): epidemiological studies assessing the prevalence of orofacial, oral or facial pain in different populations;
• C (Comparison): comparisons across geographical regions and demographic subgroups (age, sex);
• O (Outcome): estimation of the global prevalence of orofacial, oral and facial pain, and identification of potential factors influencing its distribution, particularly age and sex.
The following article types were excluded from the study: narrative reviews; systematic reviews and meta-analyses; opinion papers; case reports or case series; animal studies or biomechanical models; conference abstracts; and publications in languages other than English. Studies focusing on specific occupational or population groups (e.g., military personnel, musicians) were also excluded, unless a control group was included. In such cases, only the data from the control group was analyzed.
Grey literature was manually searched using Google, combining keywords with the names of continents, as per a previous study25:
• “orofacial pain” AND “North America, South America, Asia, Europe, Africa, Australia”;
• “facial pain” AND “North America, South America, Asia, Europe, Africa, Australia”;
• “oral pain” AND “North America, South America, Asia, Europe, Africa, Australia”.
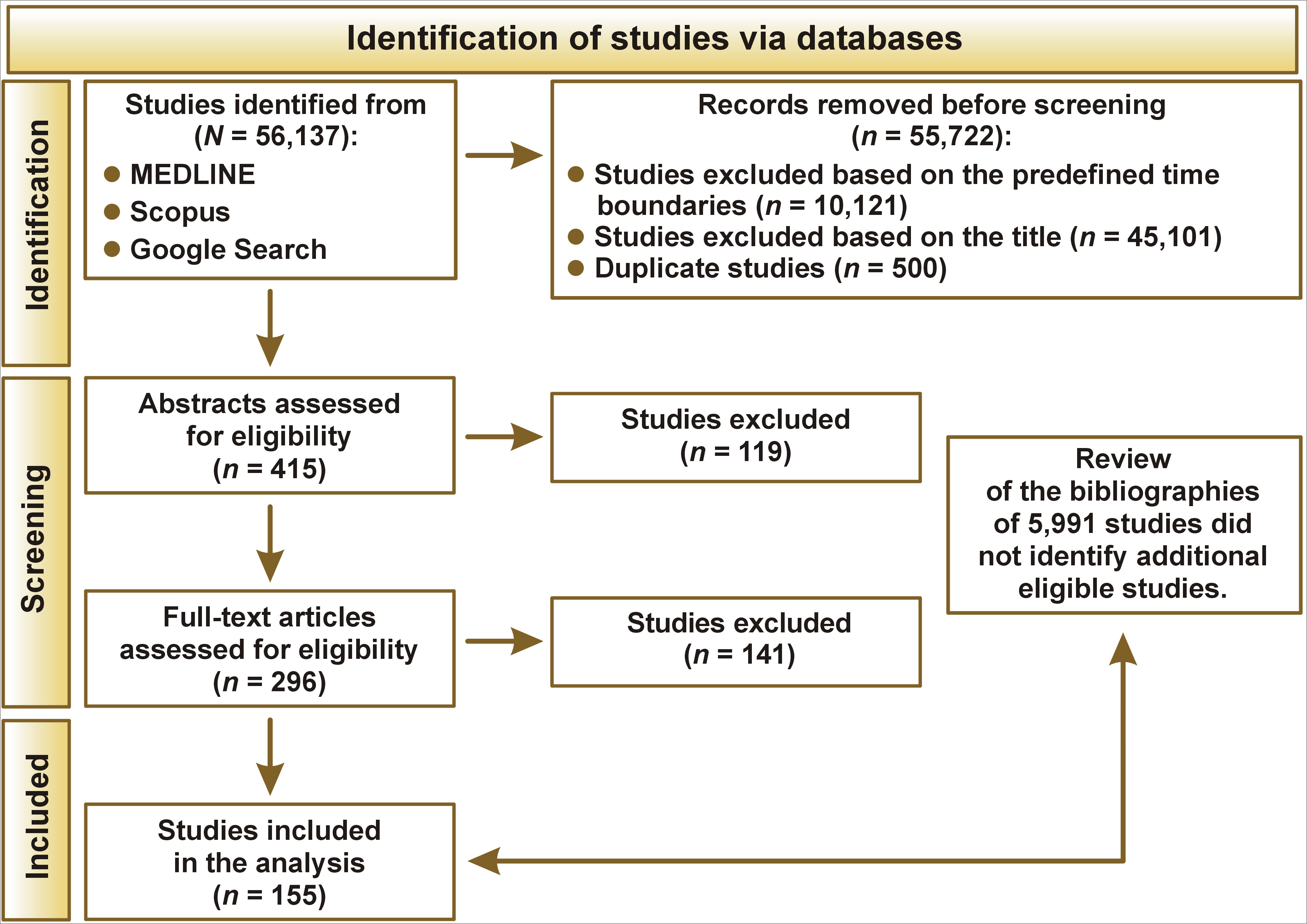
Additionally, the snowballing method was applied in accordance with Wohlin’s guidelines.34 Screening was conducted independently by 2 authors (AG and MWó) under the supervision of, and in consultation with, the first author (GZ), who had the deciding vote in cases of disagreement. The selection process was performed in 3 stages: title screening; abstract screening; and full-text assessment. It is worth emphasizing that one of the main inclusion criteria for the analysis was the presence of pain among the study participants. The flowchart of the study is presented in Figure 1.
The primary database included the following variables: DOI; first author’s surname; year of publication; continent where the study was conducted; participants’ age; total sample size (N); number of females; number of males; number of individuals reporting pain; number of individuals reporting pain stratified by sex; type of pain (facial or oral); classification according to the International Classification of Orofacial Pain (ICOP)10; and duration of pain symptoms (in months). In accordance with previously published methodology,24 participants were stratified into 3 age groups: <18 years; 18–60 years; and >60 years.
Due to differences in thematic scope and analytical approaches, the collected data was divided into 2 separate publications. This approach allows for a detailed discussion of each research area, ensures consistent argumentation and clear conclusions, and prevents excessive condensation of content that is essential to a comprehensive understanding of the presented findings.
In accordance with the stated aim, the study focuses on the global and continental prevalence of oral and facial pain in the general population. Information on the occurrence of oral and facial pain, classified according to the ICOP, is presented in the second publication.
The objectives and methodological descriptions of the analyzed studies were reviewed to assign them to specific categories: facial pain; oral pain; or general orofacial pain. Research papers that focused on the face were classified as facial pain, those concerning the oral cavity as oral pain, and works addressing general orofacial pain as orofacial pain. Classification was based on the assessment of the original study objectives and methodologies and was verified by the review authors.
Statistical analysis
The statistical methodology followed previously published papers.24, 25, 26 A meta-analysis of proportions was conducted to estimate the prevalence of orofacial pain.35 The proportion of orofacial pain cases, defined as the number of events divided by the total sample size per study, was analyzed. The logit transformation was applied to stabilize the variance of proportions and ensure that pooled estimates remained within the interval [0, 1] after back-transformation.36
The primary analysis employed a generalized linear mixed model (GLMM) with a logistic link function to directly model the binomial outcome of orofacial pain.37 This method was selected for its robustness in accounting for both within-study and between-study variability without requiring continuity corrections, making it well-suited for the dataset characteristics.38 Between-study variance (τ2) was estimated using maximum likelihood.36 Confidence intervals (CIs) for individual study proportions were constructed using the Wilson score method.39
A sensitivity analysis was performed using an alternative specification for the random-effects model based on the inverse variance method40 and restricted maximum likelihood (REML) estimation,41 which yielded comparable results with consistent heterogeneity estimates.
Subgroup analyses were conducted to explore differences in the prevalence of orofacial pain according to continent, age group and symptom duration, with separate pooled estimates calculated for each subgroup.42 Heterogeneity within and between subgroups was assessed using the I2 statistic and τ2 estimates.43 The significance of heterogeneity was evaluated using the Wald test and the likelihood ratio test (LRT). The subgroup analysis was specified to allow distinct between-study variances for each subgroup and to avoid assuming a common effect across subgroups.42 The back-transformation option was applied to present pooled proportions on the original scale for interpretability.36 The difference between the proportions of orofacial pain across subgroups was assessed using a Wald-type test.
Visualization of the pooled estimates, subgroup differences and heterogeneity statistics was conducted using forest plots and reported with 95% CIs.
Influential studies were identified using established diagnostics described by Viechtbauer and Cheung,44 including externally standardized residuals, difference in fits (DFFITS) values, Cook’s distance, covariance ratios, the leave-one-out amount of (residual) heterogeneity, the leave-one-out test statistic for (residual) heterogeneity, and differences in betas (DFBETAS).44
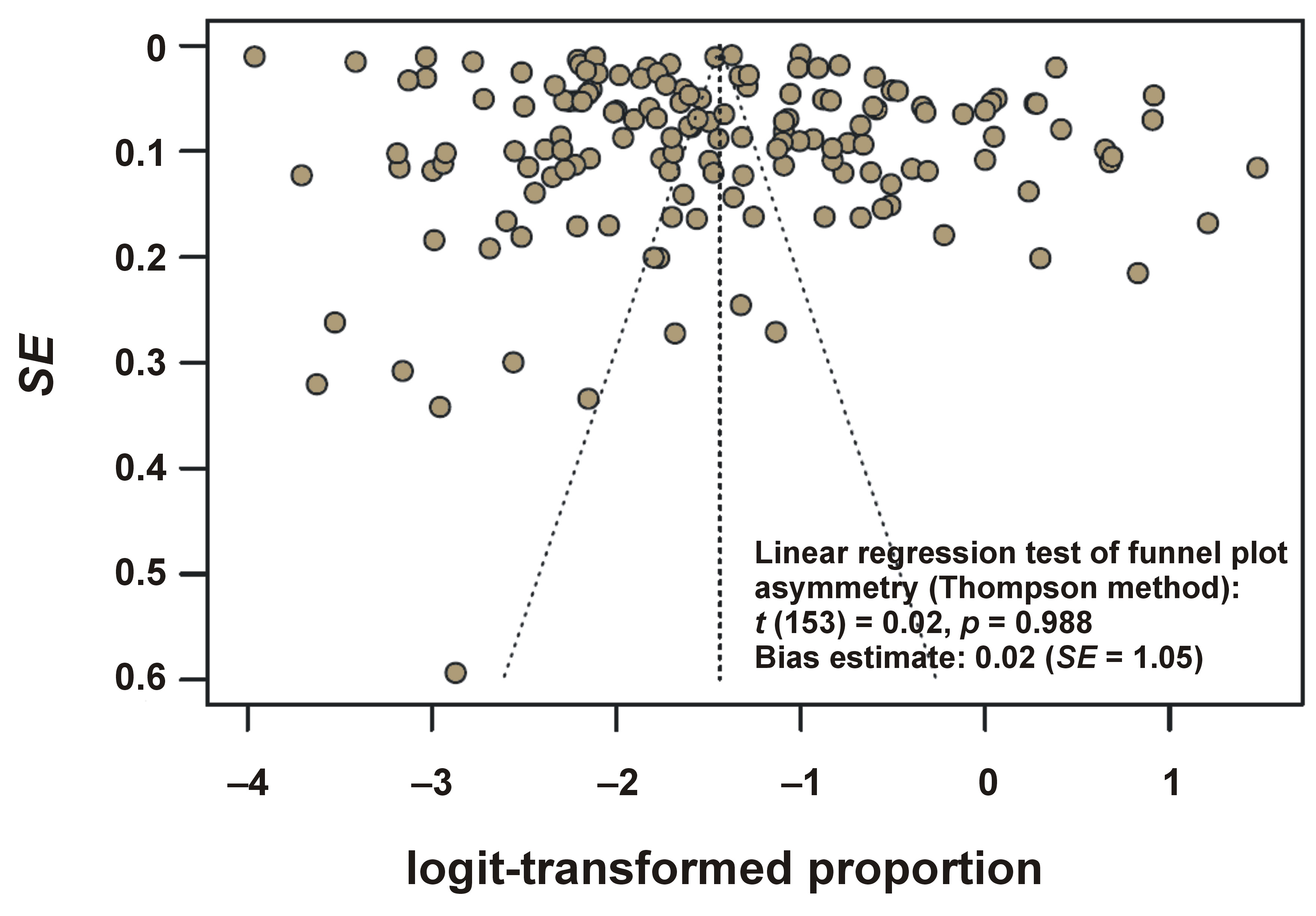
Potential publication bias was assessed using funnel plot visualization of study-specific proportion estimates against their precision (standard error (SE)).45 Asymmetry in the funnel plot, which may indicate publication bias or other small-study effects, was assessed visually and statistically.
The Thompson method was applied to formally test for funnel plot asymmetry, as it provides a regression-based approach suitable for meta-analyses of proportion data.46
The analyses were conducted using the R statistical language (v. 4.3.3; https://www.r-project.org) on Windows 11 Pro 64 bit (build 26100), and the packages meta (v. 7.0.0; Balduzzi et al.),47 dmetar (v. 0.1.0; Harrer et al.),48 report (v. 0.5.8; Makowski et al.),49 and dplyr (v. 1.1.4; Wickham et al.).50
Results
Due to the significant number of analyses, detailed information including the database, funnel plots with detailed descriptions, and exact CIs for all estimates have been included in the supplementary materials (https://osf.io/k7eds/files).
The current analysis synthesized data from 155 observational studies published between 2004 and 2024, investigating the prevalence of orofacial pain across diverse populations. After exclusion of 2 influential studies (Bölük et al.51 and Koopman et al.52), the final dataset comprised 1,712,161 participants. The mean sample size per study was 11,046 (median: 1,199; range: 42–500,488). Sex distribution was reported in 129 studies (total sample: 2,036,916), with a slight predominance of females (50.8%).
Most studies were conducted in Europe (58 studies, 945,233 participants), followed by South America (39 studies, 135,945 participants), Asia (32 studies, 96,781 participants), North America (15 studies, 415,842 participants), Africa (5 studies, 3,052 participants), and Australia (4 studies, 85,218 participants). Two studies spanned multiple continents (Asia–Europe: 1 study, 22,539 participants; North America–Australia: 1 study, 7,551 participants).
Age groups were categorized as <18 years (65 studies, 350,771 participants), 18–60 years (69 studies, 1,257,380 participants) and >60 years (11 studies, 52,206 participants). Additional categories included 18+ years (9 studies, 46,520 participants) and ≤60 years (1 study, 5,284 participants).
The reported occurrence periods for pain symptoms included 1 month (43 studies, 897,709 participants), ≥12 months (31 studies, 180,150 participants), 6 months (26 studies, 286,437 participants), and 3 months (9 studies, 236,325 participants), with 46 studies not specifying symptom duration.
The crude pooled prevalence of orofacial pain, calculated as the total number of events divided by the total sample size, was 9.53% (163,154 events). The mean study-level prevalence was 23.77% (median: 17.00%; range: 2.00–93.00%).
Concurrent oral and facial pain
A meta-analysis encompassing 155 studies, comprising 1,712,161 observations and 163,154 reported events, determined a pooled prevalence of concurrent oral and facial pain of 19.19% (95% CI: 16.59–22.08%). Substantial heterogeneity was observed across the studies (I2 = 99.9%), with a τ2 indicating considerable between-study variability and a Higgins’ H statistic reflecting extensive diversity. The statistical tests for heterogeneity confirmed this variability as highly significant, with a Wald test Q-value of 136,167.87 (degrees of freedom (df) = 154, p = 0) and an LRT p-value of 0. Sensitivity analysis using inverse variance with REML estimation produced consistent pooled estimates and heterogeneity values, confirming the robustness of the main model. To assess potential publication bias, a funnel plot presenting the distribution of study-specific proportion estimates against their precision was generated (Figure 2).
The analysis revealed no significant evidence of funnel plot asymmetry, with a test result of t = 0.02 (df = 153, p = 0.988) and a bias estimate of 0.02 (SE = 1.05). This minimal bias estimate supports the robustness of the pooled prevalence estimate, indicating that publication bias is unlikely to substantially influence the findings.
Subgroup analyses by continent provided detailed insights into regional prevalence patterns, as detailed in Table 1. In Africa, the pooled prevalence was 27.44% (95% CI: 20.86–35.18%). Asia exhibited a higher prevalence of 30.78% (95% CI: 22.81–40.08%), and Australia showed a prevalence of 15.58% (95% CI: 11.05–21.53%). Europe reported a lower prevalence of 12.27% (95% CI: 9.69–15.43%), while North America had a prevalence of 14.53% (95% CI: 9.26–22.07%), and South America displayed a prevalence of 25.61% (95% CI: 20.71–31.22%).
The test for subgroup differences indicated statistically significant variation across continents, with a Q-value of 40.59 (df = 5, p < 0.0001), highlighting the influence of geographic factors on prevalence estimates. Substantial heterogeneity was observed within the subgroups, with I2 values ranging from 88.5% in Africa to 99.9% in Europe and North America, and τ2 values varying from 0.1530 in Africa to 1.4143 in Asia, reflecting diverse study characteristics and population differences across regions. These findings underscore that the burden of concurrent oral and facial pain is most pronounced in Asia and Africa, with prevalence rates exceeding 25%, while Europe exhibits the lowest prevalence at 12.27%.
Subgroup analyses by age group provided detailed insights into age-specific prevalence patterns, as detailed in Table 2. The test for subgroup differences indicated statistically significant variation across age groups, with a Q-value of 15.74 (df = 2, p = 0.0004), highlighting the influence of age on prevalence estimates. Within-subgroup heterogeneity was also substantial, with I2 values ranging from 98.8% in the >60 years group to 99.9% in the 18–60 years group, and τ2 values varying from 1.0809 in the oldest group to 1.3368 in the youngest group, reflecting diverse study characteristics and population differences across age categories.
The above results emphasize that the burden of concurrent oral and facial pain is most pronounced among individuals aged <18 years, with a prevalence of 23.95%, followed by a decline to 16.50% in the 18–60 years group, and a further reduction to 9.83% in those older than 60 years.
Subgroup analyses by continent and age demonstrated distinct patterns in prevalence estimates (Table 2).
The test for subgroup differences indicated statistically significant variation across the 17 subgroups, with a Q-value of 253.28 (df = 16, p < 0.001), highlighting the combined influence of geographic region and age on prevalence estimates. Substantial heterogeneity was observed within the subgroups, with I2 values ranging from 75.8% in the Africa (<18 years) subgroup to 99.9% in several subgroups, including Asia (18–60 years) and Europe (18–60 years), and τ2 values varying from 0.0213 in the Africa (<18 years) subgroup to 2.3921 in the Asia (<18 years) subgroup, reflecting diverse study characteristics and population differences across regions and age categories. These findings indicate that the burden of concurrent oral and facial pain is most pronounced in Africa and Asia across all age groups, with prevalence exceeding 30% in several subgroups, while Europe and North America exhibit lower prevalence, particularly among older age groups.
Subgroup analyses by sex provided detailed insights into prevalence patterns. Among females, the pooled prevalence was 20.73% (95% CI: 16.88–25.19%), whereas among males, the prevalence was 15.20% (95% CI: 11.69–19.54%). The test for subgroup differences indicated marginally significant variation between sexes, with a Q-value of 3.51 (df = 1, p = 0.061), revealing a potential sex-related influence on prevalence estimates. Within-subgroup heterogeneity was substantial, with I2 values of 99.8% for both females and males, and τ2 values of 1.2450 for females and 1.7602 for males, reflecting diverse study characteristics and population differences across sex categories. These findings indicate a higher burden of concurrent oral and facial pain among females (20.73%) compared to males (15.20%) (Table 3).
The analysis of concurrent oral and facial pain by continent and sex is presented in Table 3. The statistical analysis indicated significant variation across the 10 subgroups, with a Q-value of 45.71 (df = 9, p < 0.001), highlighting the combined influence of geographic region and sex on prevalence estimates. Heterogeneity was substantial within the subgroups, with I2 values ranging from 98.0% in the Australia (male) subgroup to 99.9% in the North America (male) subgroup, and τ2 values varying from 0.15 in the Australia (male) subgroup to 2.65 in the North America (male) subgroup, reflecting diverse study characteristics and population differences across regions and sexes. These findings indicate that the burden of concurrent oral and facial pain is most pronounced in Asia and South America, particularly among females (>28%), while Europe exhibits the lowest prevalence, especially among males (8%).
Facial pain
A meta-analysis encompassing 36 studies, comprising 821,660 observations and 31,341 reported events, determined the pooled prevalence of facial pain to be 12.42% (95% CI: 9.17–16.62%) (Table 1). This estimate reflects a notable health burden associated with facial pain across the included studies. Substantial heterogeneity was observed across the studies, with an I2 of 99.9% and a τ2 indicating considerable variability between the studies. The statistical tests for heterogeneity confirmed this variability as highly significant, with a Wald test Q-value of 28,997.41 (df = 35, p < 0.001) and an LRT p-value <0.001. This finding indicates that facial pain affects a significant proportion of the population, with a pooled prevalence of 12.42% representing a substantial public health concern.
Subgroup analyses by continent revealed distinct regional variations in prevalence. In Asia, the pooled prevalence was 16.73% (95% CI: 13.67–20.30%), while Europe exhibited a lower prevalence of 10.30% (95% CI: 7.24–14.45%). North America showed a prevalence of 15.75% (95% CI: 7.37–30.53%), and South America displayed the highest prevalence at 33.44% (95% CI: 20.62–49.29%). The test for subgroup differences indicated statistically significant variation across the 4 continental subgroups, with a Q-value of 15.10 (df = 3, p = 0.002), highlighting the influence of geographic factors on prevalence estimates. Within-subgroup heterogeneity was substantial, with I2 values ranging from 78.4% in Asia to 99.9% in Europe, and τ2 values varying from 0.0229 in Asia to 1.0701 in Europe, reflecting diverse study characteristics and population differences across regions. These findings indicate that the burden of facial pain is most pronounced in South America, with a prevalence of 33.44%, while Europe exhibits the lowest prevalence at 10.30% (Table 1).
Oral pain
A meta-analysis encompassing 46 studies, comprising 400,884 observations and 65,592 reported events, determined the pooled prevalence of oral pain to be 21.04% (95% CI: 17.38–25.24%) (Table 1). This estimate highlights a significant health burden associated with oral pain across the included studies. Substantial heterogeneity was observed across the studies, with an I2 of 99.8% and a τ2 indicating considerable variability between the studies. The statistical tests for heterogeneity confirmed this variability as highly significant, with a Wald test Q-value of 22,566.93 (df = 45, p < 0.001) and an LRT p-value <0.001.
Subgroup analyses by continent revealed notable regional variations in prevalence. In Africa, the pooled prevalence was 30.79% (95% CI: 28.77–32.89%). Australia exhibited a prevalence of 20.61% (95% CI: 16.87–24.92%). Asia showed a prevalence of 24.90% (95% CI: 19.41–31.34%). Europe reported a prevalence of 16.49% (95% CI: 9.86–26.27%), and North America displayed a prevalence of 13.25% (95% CI: 10.19–17.05%). In South America, the prevalence was 24.22% (95% CI: 17.64–32.29%). The test for subgroup differences indicated statistically significant variation across the 6 continental subgroups, with a Q-value of 61.32 (df = 5, p < 0.001), highlighting the influence of geographic factors on prevalence estimates. Heterogeneity within the subgroups was substantial, with I2 values ranging from 66.7% in Africa to 99.8% in South America, and τ2 values varying from 0 in Africa to 0.9829 in Europe, reflecting diverse study characteristics and population differences across regions. These findings infer that the burden of oral pain is most pronounced in Africa, with a prevalence of 30.79%, followed by Asia and South America, both exceeding 24%, while North America and Europe exhibit lower prevalence rates of 13.25% and 16.49%, respectively (Table 1).
Prevalence of concurrent oral and facial pain by observation period
Subgroup analyses of the occurrence of oral and facial pain symptoms in months revealed distinct patterns. For pain reported within 1 month, the pooled prevalence was 16.19% (95% CI: 12.40–20.86%). For pain reported within 3 months, the prevalence was 12.06% (95% CI: 6.23–22.08%). For pain reported within 6 months, the prevalence was 25.30% (95% CI: 18.74–33.22%), while for pain reported over 12 months or more, the prevalence was 25.51% (95% CI: 19.80–32.20%) (Table 4). The test for subgroup differences indicated statistically significant variation across the 4 duration subgroups, with a Q-value of 11.04 (df = 3, p = 0.012), highlighting the influence of observation period on prevalence estimates. Heterogeneity within the subgroups was substantial, with I2 values of 99.9% in the 1-month group and 99.8% in the other duration groups, and τ2 values ranging from 0.83 in the ≥12 months group to 1.23 in the 3-month group, reflecting diverse study characteristics and population differences across duration categories. The results indicate that extending the assessment period to ≥6 months reveals a greater prevalence of concurrent oral and facial pain (>25%) compared with shorter intervals of 1–3 months (<16%).
Assessment of funnel plot asymmetry and publication bias
To evaluate potential publication bias and small-study effects, a linear regression test was conducted following the approach described by Thompson and Sharp.46 This analysis assessed the degree of asymmetry in the funnel plots generated for the included studies. A non-significant p-value indicated insufficient evidence to reject the null hypothesis of symmetry, suggesting no substantial asymmetry in the data and, consequently, no indication of publication bias (Table 5). Funnel plots for each subgroup are provided in the supplementary materials.
Discussion
The primary aim of this study was to determine the global prevalence of oral and facial pain in the general population and across continents. The results confirmed the initial hypothesis, demonstrating that the global prevalence of oral and facial pain remains below 30%, supporting the assumption of a moderate but clinically significant worldwide burden. To begin this discussion, it is important to emphasize that the analysis encompassed 155 studies and over 1.7 million observations. Attention should be drawn to the scale of the problem of comorbid oral and facial pain, as well as to the considerable variability in findings depending on continent, age, sex, and symptom duration. The estimated global prevalence of approx. 19% indicates a notable health burden that extends beyond the local context and should be regarded as a significant public health concern. However, the analyzed results demonstrated a high degree of heterogeneity, which profoundly influences the interpretation of these outcomes and reflects the multidimensional complexity of orofacial pain phenomena.
High heterogeneity (I2 values exceeding conventional thresholds) indicates that the included studies differ substantially in design, population characteristics and diagnostic definitions. From a methodological standpoint, this heterogeneity reduces the precision of pooled estimates, suggesting that the global prevalence should be interpreted as a broad epidemiological tendency rather than an exact quantitative measure.43, 46, 53 Clinically, it highlights the contextual dependence of orofacial pain, the expression and reporting of which vary according to cultural, socioeconomic and healthcare system factors. Therefore, while heterogeneity limits the statistical generalizability of the results, it simultaneously enriches understanding by revealing the complexity of pain as a biopsychosocial construct.
When comparing our findings with previous epidemiological studies, it is worth recalling data from the last century, which estimated that orofacial pain occurred in approx. 10% of the adult population.54, 55 The observed increase over the past 25 years may have multiple causes, ranging from improved diagnostics and greater awareness of the problem among both patients and clinicians to lifestyle changes, stress, an increasing number of risk factors, and the residual effects of the coronavirus disease 2019 (COVID-19) pandemic.11, 26, 56, 57, 58 The COVID-19 pandemic likely influenced pain perception and prevalence indirectly through increased psychosocial stress, changes in access to dental and medical care, and altered health-seeking behaviors. Lockdowns and healthcare disruptions may have contributed to delayed diagnoses, while elevated anxiety and bruxism during the pandemic period could have temporarily increased the prevalence of orofacial pain in certain populations.18, 25, 59
When analyzed by continent, a particularly striking contrast emerges between Asia and Africa, where prevalence rates exceed 27–30%, and Europe or North America, where the rates are approx. 12% and 14.5%, respectively. This suggests that geographic factors, including cultural, economic and biological determinants, play a key role in shaping the distribution of such conditions. These findings have been underscored in recent (2024–2025) meta-analyses and forecasts.24, 25, 26, 27 However, it is important to recognize that such substantial intercontinental variation reflects not only true epidemiological differences but also methodological heterogeneity among studies. Differences in sampling strategies, diagnostic criteria, data collection methods, and reporting standards may contribute to variability in prevalence estimates. Therefore, heterogeneity in this context should not be treated merely as statistical noise, but rather as an expression of the inherent variability in pain-related experiences across human populations.
It can be assumed that these differences arise from variations in dental care patterns, access to pain management, dietary habits, and psychosocial determinants such as stress and socioeconomic status.24, 60 Cultural norms also influence responses to pain: in some societies, open expression of suffering is socially acceptable, while in others, restraint is emphasized.60, 61, 62 Such cultural frameworks shape not only the interpretation and reporting of pain, but also coping strategies.60, 63, 64
A similar pattern of heterogeneity is evident across age groups. The highest prevalence was observed among individuals under 18 years of age (23.95%), suggesting that children and adolescents may be particularly vulnerable to such conditions. Contributing factors include frequent orthodontic problems, dental caries and psychosocial determinants such as greater susceptibility to academic stress and challenges associated with developmental changes.65, 66, 67 By contrast, older adults (>60 years) showed a markedly lower prevalence of pain (9.83%). This paradoxical trend warrants deeper analysis. One possible explanation involves neurobiological adaptations to chronic nociceptive stimuli, leading to altered pain processing (hypoalgesia) with advancing age.68, 69, 70, 71 Furthermore, age-related degeneration of peripheral nociceptors, the use of analgesic or anti-inflammatory medications, and potential underreporting due to reduced pain awareness or social normalization of discomfort in older age may contribute to this phenomenon.68, 69, 70, 71 Psychologically, older adults may also demonstrate greater emotional regulation and coping efficiency, diminishing perceived pain intensity. Thus, the age-related paradox likely reflects a complex interplay between biological desensitization, pharmacological influences and sociocognitive factors.70, 72, 73
Sex-based differences provide another dimension of variability. Women reported orofacial pain more frequently than men (20.73% vs. 15.20%), consistent with broader observations in pain research. The higher prevalence of pain among women may be partially explained by hormonal influences, as female hormones have been shown to modulate pain perception.20, 21 A greater burden of orofacial pain in women is a well-documented finding in the literature.24, 74 Nevertheless, the magnitude of sex differences varies substantially across studies, reflecting heterogeneity in methodologies and populations.
Separating oral pain from facial pain yielded additional insights. Oral pain (21.04%) was more prevalent than facial pain (12.42%), suggesting that dental and periodontal conditions are primary drivers of the problem. Marked regional differences are also apparent: in Africa, 30.79% of individuals experience oral pain, compared with 13.25% in North America. The highest prevalence of facial pain was observed in South America (33.44%), once again highlighting the influence of environmental, economic and healthcare access factors. However, caution is warranted when interpreting these results, as heterogeneity in study quality and pain definitions could partially inflate apparent differences.
Analyses focusing on Africa and Australia are pioneering, as earlier meta-analyses highlighted significant gaps in the literature for these regions.24, 25 Notably, the reported prevalence of oral pain in Africa (30.79%) closely aligns with projected rates of TMD for the continent in 2030, estimated at 37% (95% CI: 32–42%).27 In the South American context (facial pain prevalence of 33.44%), it is relevant to compare these findings with the results of a 2025 meta-regression showing that in North America, comorbidity between bruxism and TMD reached 70%, with a mean TMD prevalence of 98.3% among patients with bruxism.26 These observations underscore the urgent need for further research and preventive measures on these continents.
At the beginning of this century (2002), it was reported that the prevalence of orofacial pain was 7% over a 7-day period and 16% over a 12-month period.54 Likewise, our analysis demonstrated an increasing trend in pain prevalence with longer assessment windows, although current global prevalence rates are higher. Short observation periods yielded lower prevalence estimates (16.19% for up to 1 month and 12.06% for up to 3 months), whereas prevalence exceeded 25% when pain was assessed for 6 months or longer.54, 75, 76
These findings have several implications for public health and clinical practice. First, in terms of healthcare resource allocation, regions with high prevalence of orofacial pain (e.g., Africa, South America and Asia) should prioritize expanding access to dental and pain management services. Second, regarding screening recommendations, standardized pain assessment tools should be incorporated into routine dental and primary care visits to facilitate early detection. Third, preventive strategies should emphasize education on oral hygiene, stress reduction and early management of temporomandibular dysfunctions. Collectively, these approaches may improve global oral health outcomes and reduce the long-term burden of orofacial pain.
The primary limitation of the present study is the high heterogeneity among the included studies, which reduces the precision of pooled estimates. The database was created based on published data provided by the original study authors, which introduces a potential risk of reporting bias; however, this approach is commonly accepted in meta-analytic research.24, 25 Furthermore, the study did not account for additional covariates such as local pain response, healthcare quality or the reliability of self-assessment.
Another important limitation is that the vast majority of included studies relied on self-reported pain assessment tools, the validity and comparability of which remain limited. Instruments such as the visual analogue scale (VAS), numeric rating scale (NRS) or various pain questionnaires are not equivalent either in what they measure (e.g., intensity, frequency, presence of pain, or impact on daily functioning) or in how participants interpret the questions. The diversity of applied tools can lead to systematic differences in reporting. Some scales tend to produce higher pain scores, while others may underestimate intensity.77, 78 This lack of standardization significantly complicates cross-study comparisons and increases the risk of measurement error, which in turn may contribute to over- or underestimation of the true global prevalence of orofacial pain.
It should also be emphasized that self-reported pain is susceptible to both recall bias and cultural differences in pain expression. Participants often report pain retrospectively, based on general impressions rather than precise recollection of pain episodes, which can lead to over-reporting among individuals with chronic pain and under-reporting in those with episodic pain. Additionally, cultural norms regarding the acceptability of expressing discomfort, displaying suffering, or expectations related to healthcare interactions may shape self-reports. In some cultures, minimizing complaints is more typical, while in others, detailed and open reporting of pain is normative.60, 61, 62, 63, 64 These cultural factors, combined with the inherent subjectivity of self-reports, may result in substantial population-level differences that do not necessarily reflect actual prevalence but rather distinct styles of communication and perception of discomfort.
In the current study, a formal risk-of-bias assessment at the level of individual studies was not conducted,79, 80 as the analysis was designed as a proportion meta-analysis primarily based on statistical methodology.
In summary, the present meta-analysis provides compelling evidence of a substantial population-level burden associated with oral and facial pain, while also demonstrating that this phenomenon is strongly modulated by age, sex, geographic region, and symptom duration. Crucially, the considerable heterogeneity observed across studies should not be seen merely as a methodological challenge but rather as a reflection of the complex, context-dependent nature of orofacial pain. Understanding this variability offers valuable insights into underlying biological, social and cultural mechanisms. Thus, although heterogeneity complicates straightforward interpretation, it enriches the discussion and underscores the need for standardized research approaches and context-sensitive prevention strategies.
Conclusions
1. The present study indicates that the global prevalence is 19% for concurrent oral and facial pain, 12% for facial pain and 21% for oral pain.
2. A relatively high prevalence of oral pain (31%) and combined oral and facial pain (27%) was observed in Africa. Further research on facial pain in this region is recommended. These findings infer that the burden of oral pain is particularly pronounced in Africa.
3. A prevalence of 31% for concurrent oral and facial pain was observed in Asia, with 17% experiencing facial pain and 21% oral pain.
4. Australia exhibited a lower overall prevalence of concurrent oral and facial pain (16%), but the prevalence of oral pain was notably higher (25%). Due to the limited number of studies available, these results should be considered preliminary and interpreted with caution. It is recommended that further research on facial pain be conducted in this region.
5. Comparatively low prevalence rates were observed in Europe across all categories: 12% for concurrent oral and facial pain; 10% for facial pain; and 16% for oral pain. These findings indicate that facial pain has the lowest prevalence in Europe.
6. North America presented moderate and consistent levels, with 15% experiencing concurrent oral and facial pain, 16% experiencing facial pain and 13% experiencing oral pain. These results suggest that oral pain has the lowest prevalence in North America.
7. The highest recorded prevalence of facial pain (33%) was observed in South America; in this region, the prevalence of oral pain was 24% and that of concurrent oral and facial pain was 26%. These findings indicate that the burden of facial pain may be most pronounced in South America.
8. Concurrent oral and facial pain was most prevalent in individuals up to 18 years of age (24%). This prevalence decreased to 16% among those aged 18–60 years and further declined to 10% among individuals aged >60 years, highlighting a clear age-related downward trend.
9. When considering both continent and age group, concurrent oral and facial pain was most prevalent in Africa and Asia, where rates exceeded 30% in several subgroups. In contrast, Europe and North America exhibited lower prevalence levels, particularly among older age groups.
10. Females demonstrated a higher prevalence of concurrent oral and facial pain (21%) compared with males (15%). Overall, the burden of concurrent oral and facial pain was highest in Asia and South America, particularly among females (exceeding 28%), whereas the lowest prevalence was observed in Europe, especially among males (8%).
11. The occurrence of pain symptoms across different observation periods is as follows: within 1 month, 16% of the population experienced pain; within 3 months, 12%; within 6 months, 25%; and within 12 months or longer, 26%. These findings indicate that the prevalence of concurrent oral and facial pain is most pronounced for observation periods of 6 months and longer, exceeding 25%, while shorter durations (1 and 3 months) show lower prevalence.
12. The results of the present study should be interpreted with caution due to the high heterogeneity among the included studies. Further epidemiological research is recommended, employing rigorous methodology and adherence to current pain classification systems.
Ethics approval and consent to participate
Not applicable.
Data availability
The data related to this article, including supplementary materials, is available in the Open Science Framework database (https://osf.io/k7eds/files). The script used in the analysis is available from the corresponding author upon reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.