Abstract
Background. Children with autism spectrum disorder (ASD) have higher rates of feeding problems and sleep disorders. Research on feeding problems in children with ASD has focused on behavioral, psychological and nutritional aspects. However, the biomechanics underlying these issues remains unknown.
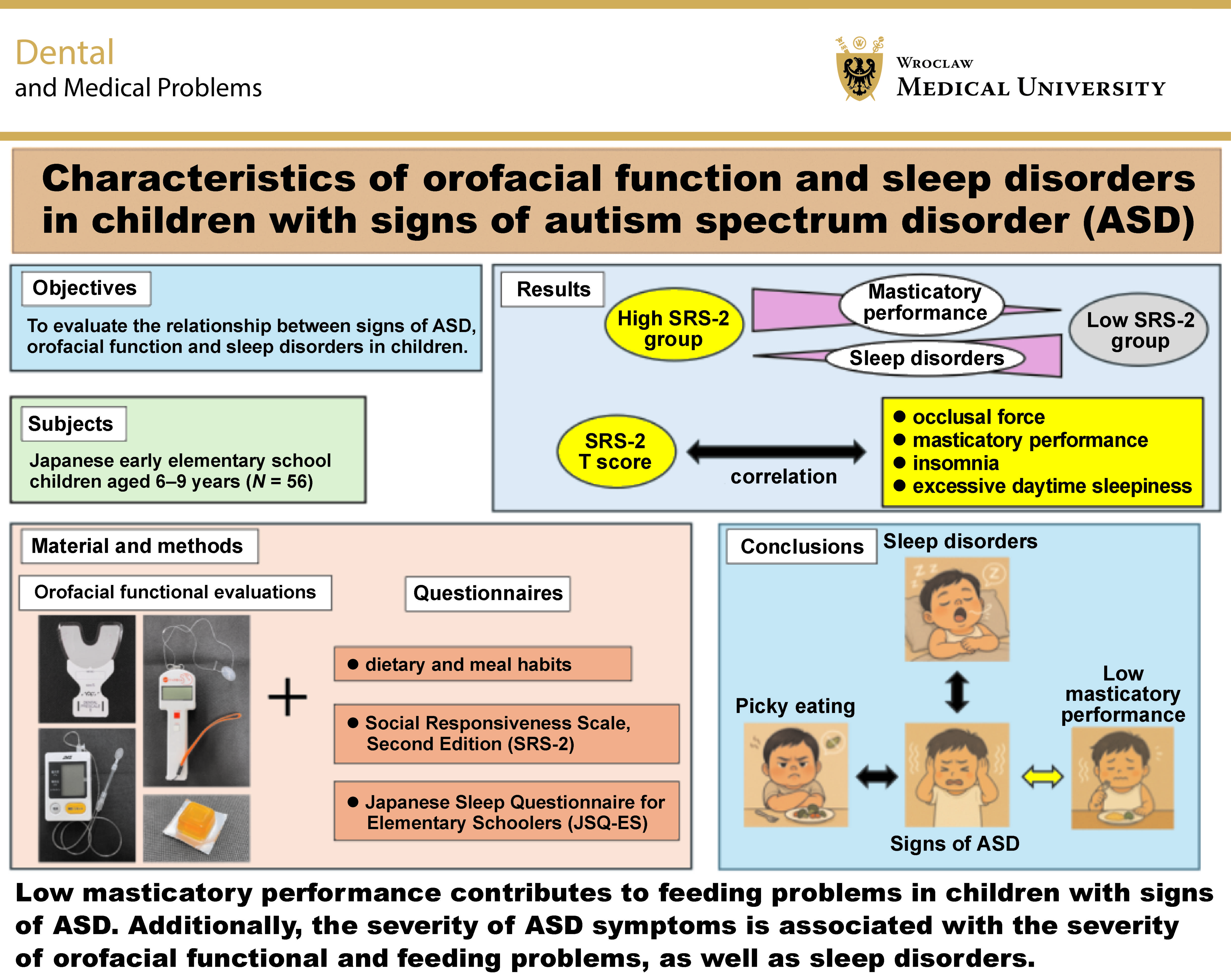
Objectives. The present study aimed to evaluate the relationship between signs of ASD, orofacial function and sleep disorders in children.
Material and methods. A total of 56 Japanese early elementary school children aged 6–9 years were recruited. The subjects underwent physical examinations, intraoral inspections and orofacial functional assessments. The parents or legal guardians of the children completed questionnaires regarding the subjects’ dietary and meal habits, the Social Responsiveness Scale, Second Edition (SRS-2), and the Japanese Sleep Questionnaire for Elementary Schoolers (JSQ-ES). Each assessment item was compared between 2 groups divided according to the SRS-2 scores, and the relationships with psychological traits were investigated using Spearman’s rank correlation coefficient.
Results. Thirteen of the 56 children had SRS-2 T scores ≥60, indicating possible ASD. Masticatory performance was significantly lower in the high SRS-2 group than in the low SRS-2 group (p < 0.05). Additionally, the high SRS-2 group showed significantly higher T scores on the JSQ-ES for insomnia (p < 0.05) and excessive daytime sleepiness (p < 0.01). Occlusal force (p < 0.05), masticatory performance (p < 0.05), insomnia (p < 0.001), and excessive daytime sleepiness (p < 0.001) were significantly correlated with the SRS-2 score.
Conclusions. These results suggest that low masticatory performance contributes to feeding problems in children with signs of ASD. Additionally, the severity of ASD symptoms is associated with the severity of orofacial functional and feeding problems, as well as sleep disorders.
Keywords: autism spectrum disorder, sleep disorder, school children, orofacial function, masticatory performance
Introduction
Autism spectrum disorder (ASD) is a common neurodevelopmental condition characterized by social and/or communication difficulties, as well as the presence of restrictive or repetitive behaviors.1 Autism spectrum disorder has a worldwide prevalence of approx. 1–3% and occurs nearly 4 times more frequently in boys than in girls.2 Previously, children with autism were diagnosed at ages older than 3–4 years. Currently, toddlers are more frequently diagnosed due to early recognition of atypical development.3 However, high-functioning individuals are often diagnosed late or remain undiagnosed and latent.3
Autism spectrum disorder is frequently accompanied by sleep problems such as insomnia, circadian rhythm disorder and obstructive sleep apnea (OSA).4 Approximately 60–80% of pediatric patients with ASD experience sleep difficulties, with insomnia being the most common.5, 6 As determined by actigraphy or polysomnography, children with ASD have reduced total sleep time, longer sleep latency and decreased sleep efficiency compared to typically developing children.7 Additionally, children with ASD demonstrate higher rates of OSA, with a frequency of approx. 30–60%.4, 8 The severity of sleep problems in ASD is associated with the severity of ASD symptoms.9
Children with ASD are 5 times more likely to experience feeding problems than their peers, including unusual eating habits, feeding difficulties and restrictive diets.10, 11 Limited food preference is the most common feeding problem behavior in children with ASD, followed by hypersensitivity to food textures and eating only one brand of food.11 Thus, research on feeding problems in children with ASD has focused on behavioral, psychological and nutritional aspects.10, 11, 12 Additionally, pediatric patients with ASD frequently have hypotonia and apraxia, especially oral motor apraxia, manifesting as excessive drooling, an open mouth at rest, and an inability to pucker the lips, lick the lips with the tongue, or blow bubbles.13 However, the majority of studies on oral motor skills in children with ASD have focused on speech.14 Of the few publications addressing feeding, one reported significantly lower mylohyoid muscle activity among autistic children during eating.14, 15 Other studies have usually relied upon caregiver questionnaires. Therefore, further investigation of feeding problems associated with ASD in children, with a focus on the biomechanics of feeding, is warranted.
Mastication is a rhythmic movement regulated by a central pattern generator, and is the first step in the digestive process, in which food is broken down for swallowing.16, 17 The coordinated actions of the jaws, teeth, connecting muscles, lips, and tongue are critical in the mastication process.18 Oral motor dysfunction, such as tongue protrusion, incoordination of eating and breathing, lack of rhythmic movement, and insufficient lip closure, can be associated with masticatory disabilities.19, 20 To evaluate masticatory function in children, masticatory performance is usually measured by determining the size of food particles after a standardized number of chewing cycles.21 However, few studies have evaluated masticatory performance in children based on neurodevelopmental aspects.
Recent research has reported that improvements in orofacial function may contribute to enhanced sleep quality in postoperative residual OSA.22 This indicates that orofacial dysfunction and sleep disorders could be mutually correlated in children with ASD. One study has recommended the incorporation of routine sleep screening into the clinical practice of general pediatric clinics, as there could be a specific subgroup of patients with sleep-disordered breathing (SDB) that may go undetected.23 Therefore, using questionnaire-based assessments of SDB and ASD in pediatric dental practice may be useful to clarify the relationship between these 2 separate problems in children with ASD.
The present study aimed to assess the relationship between sleep problems, signs of ASD and orofacial function in children using screening tools. Additionally, the significance of interventions for these problems was discussed.
Material and methods
Ethics statement
The present study was conducted in strict accordance with the Declaration of Helsinki. The study protocol was approved by the Ethics Committee of the Graduate School of Dentistry at the University of Osaka, Japan (approval No. R3-E5). All parents or legal guardians of the patients were informed of the content of the study and provided with written information as well as verbal explanations. Written informed consent for study participation was obtained from all parents/guardians, and verbal agreement and written informed assent were obtained from all children.
Participants
Fifty-six Japanese children aged between 6 and 9 years (38 boys and 18 girls; mean age: 7.8 ±0.9 years) who attended the Pediatric Dentistry Clinic at The University of Osaka Dental Hospital from October 2021 to August 2024 were recruited through announcements posted in the clinic. The participants had undergone regular oral health checks at the clinic; some had previously visited with primary complaints of dental caries, dental trauma, occlusion problems, and mesiodentes, while others had visited seeking regular oral care. The inclusion criteria encompassed children with normal language comprehension, no reported health problems (systemic diseases or soft tissue abnormalities including cleft lip and palate), completed caries treatment, no clinical diagnosis regarding neurodevelopmental or comorbid conditions, and no history of psychotropic medication use. Pediatric patients who were uncooperative during clinical examinations and those with incomplete questionnaires from parents/guardians were excluded. No participants declined to participate or dropped out of the study.
Psychological examination (symptom measurement)
The severity of ASD symptoms was assessed using the Social Responsiveness Scale, Second Edition (SRS-2), as reported by the parents or legal guardians of the participants.24 Its predecessor, the SRS, has been one of the most frequently used quantitative measures of autism symptoms, with strong measurement properties in healthy and autism-affected samples.25 For individuals aged 4–18 years, the SRS-2 represents the same item set as the SRS. The SRS-2 is an ordinally scaled (from 1 = not true to 4 = almost always true) quantitative assessment measuring 65 items regarding a child’s behavior. The items are clustered into 5 subdomains: social awareness; social cognition; social communication; social motivation; and restricted repetitive behaviors. The discriminant validity of the SRS-2 is supported by sensitivity/specificity metrics and area under the curve (AUC) values across populations. The internal consistency (Cronbach’s α) was 0.95 in the clinical sample and 0.97 in the non-clinical standardization sample, indicating high reliability. The total raw scores were assessed and converted into T scores, with values of 60–65, 66–75 and ≥76 indicating mild, moderate and severe ASD symptoms, respectively.
Examination of sleep disorders
The scores for sleep disorders were calculated using the Japanese Sleep Questionnaire for Elementary Schoolers (JSQ-ES), as reported by the parents or legal guardians of the participants.26 The JSQ-ES is a validated screening tool designed to assess sleep problems in Japanese elementary school children. The JSQ-ES is an ordinally scaled (from 1 = strongly disagree/false/inapplicable to 6 = strongly agree/true/applicable) quantitative assessment measuring 38 items regarding sleep disorders and sleep habits in children. Exploratory and confirmatory factor analyses supported a nine-factor structure: restless legs syndrome; SDB; morning symptoms; nighttime awakenings; insomnia; excessive daytime sleepiness; daytime behavior; sleep habits; and irregular/delayed sleep phase. Scores clearly differentiated children with clinically diagnosed sleep disorders from the community sample, with an optimal cut-off score of 80 points. The internal consistency (Cronbach’s α) was 0.88 in the community sample and 0.91 in the clinical sample, indicating high reliability. T scores and their sum in the 9 subdomains were assessed. Additionally, sleep bruxism was evaluated using an ordinal scale ranging from 1 to 6.
Questionnaires regarding dietary and meal habits
The following information was collected from participants’ parents or legal guardians to evaluate dietary and meal habits: amount of food consumed per meal (excessive food intake, insufficient food intake, variable food intake); eating speed (too fast, too slow); picky eating (severe, mild, none); and behavior during meals (calm, standing up and playing).
The above 3 questionnaires were collected after the completion of the clinical examination and orofacial functional evaluation.
Clinical examination
All examinations were performed by a dentist (MK) under the supervision of a pediatric dentist with over 10 years of specialized experience (MO). The physical examinations included anthropometric measurements of height and weight. During the oral examinations, the number of erupted teeth and the total number of decayed, missing, and filled teeth (dmft/DMFT) were recorded by visual inspection with a dental mirror under lighting according to the criteria established by the World Health Organization (WHO).27 Additionally, the number of teeth (deciduous + permanent teeth) and Hellman’s dental age (IIA, IIC, IIIA, IIIB, IIIC) were evaluated. Lip seal was recorded by observing the child’s appearance in a resting position as they entered the room before they were aware of the pending examination. Incompetent lip seal was defined as the natural separation of the lips.28, 29 After the physical and oral examinations, orofacial functional evaluations were performed in the order delineated below. All participants were placed in the same room under the same lighting conditions and used the same chairs and desks.
Occlusal force testing
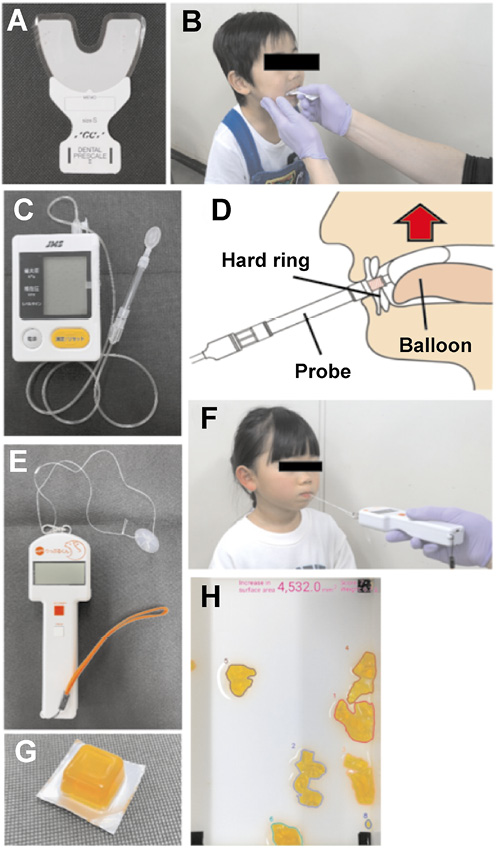
The occlusal force was measured using Dental Prescale II (GC Corporation, Tokyo, Japan) (Figure 1A) and occlusal force analysis software (Bite Force Analyzer; GC Corporation).30 The subjects were instructed to practice biting in the maximum intercuspal position 2 or 3 times before the measurement. The measurement was taken with the Frankfort horizontal plane parallel to the floor surface so that the occlusal state was as stable as possible. During the measurement, the examiner took care to avoid allowing the patient to slide or brux when the upper and lower teeth touched, and the occlusal state was recorded for approx. 3 s while biting down (Figure 1B).31
Maximum tongue pressure
Maximum tongue pressure was measured with the use of a tongue pressure measurement device (JMS, Hiroshima, Japan) (Figure 1C).32 The subjects were instructed to practice biting the hard ring of the probe with their upper and lower incisors in an upright seated position and then raise their tongues and compress the balloon onto the palate, with the Frankfort plane maintained horizontally and the soles of their feet placed flat on the floor before the measurement (Figure 1D). During the assessment, the examiner ensured that the balloon was positioned vertically between the palate and the tongue. The measurements were recorded 3 times with a rest interval between each, and the largest of the 3 measurements was used for analysis.
Lip-closing strength
Lip-closing strength was measured using a digital force gauge (Lipplekun; Shofu Inc., Kyoto, Japan) (Figure 1E).33 The subjects were instructed to insert a Lippule button (Shofu, Inc.) into the space between their incisors and lips, and to hold it with minimal mouth opening in a relaxed sitting position. Subsequently, they were asked to hold the button tightly in their mouths, and a string with a length of approx. 10 cm was tied to the center of the button. The strain force gauge was attached to the end of the string and pulled parallel to the floor. The strength, measured as the highest tension before the button was pulled from the mouth, was recorded 3 times with a rest interval between each, and the largest of the 3 measurements was used for analysis (Figure 1F).
Masticatory performance
Masticatory performance was assessed using test gummy jellies (20 mm × 20 mm × 10 mm; UHA Mikakuto, Tokyo, Japan) (Figure 1G).34 The subjects were asked to sit in an upright position and chew the gummy jelly freely 30 times without swallowing, as they normally would. Thereafter, they were asked to spit out the particles onto cotton gauze placed over the top of a disposable cup without leaving any residue in their mouth. The gummy particles were then rinsed with tap water to prevent further dissolution and transferred into a prepared box containing 30 mL of water to prevent overlapping of the particles. Digital images of the box containing the comminuted pieces were captured using a smartphone camera and analyzed to calculate the increase in surface area and weight of the comminuted gummy jelly (Figure 1H).35
Statistical analysis
Descriptive analyses included calculation of relative frequencies, mean ± standard deviation (M ±SD) values, and medians (Mes) (interquartile ranges (IQRs)) in 2 groups based on the SRS-2 total T scores: the high SRS-2 group (T scores ≥60); and the low SRS-2 group (T scores <60). The Shapiro–Wilk test was used to examine the normality of data distribution. The χ2 test or Fisher’s exact test, and Student’s t-test or the Mann–Whitney U test, where appropriate, were used to compare the 2 groups. Additionally, Spearman’s rank correlation coefficient was employed to investigate the relationships between the SRS-2 T score and each assessment item, as well as to evaluate the relationships between sleep disorder scores, dietary and meal habits, and orofacial functional scores. The data was analyzed using the IBM SPSS Statistics for Windows software, v. 28.0 (IBM Corp., Armonk, USA). The level of statistical significance was set at p < 0.05. For all significant comparisons, the effect sizes (Cohen’s d or Cramer’s V) or 95% confidence intervals (CIs) were reported. Additionally, power analysis was performed with the G* Power program, v. 3.1.9.6.36 Given an anticipated effect size of 0.5, a two-tailed test, a significance level of 5%, and a total sample size of 56, the estimated power was 0.981.37
Results
Descriptive statistics
Of 56 children, 13 (23.2%) had SRS-2 T scores of 60 or more and were regarded as having signs of ASD (Table 1). The high SRS-2 group had substantially higher T scores than the low SRS-2 group (p < 0.001, Cohen’s d = −3.272). There were no significant differences in age, sex, height, weight, or body mass index (BMI) between the 2 groups.
Sleep disorder scores
Table 2 presents sleep disorder scores according to the JSQ-ES. The high SRS-2 group showed significantly higher T scores for restless legs syndrome (p < 0.01; Cohen’s d = −0.981), nighttime awakenings (p < 0.01; Cohen’s d = −1.078), insomnia (p < 0.05; Cohen’s d = −0.679), excessive daytime sleepiness (p < 0.01; Cohen’s d = −0.957), daytime behavior (p < 0.01; Cohen’s d = −1.005), irregular/delayed sleep phase (p < 0.01; Cohen’s d = −0.789), and the sum of the 9 domains (p < 0.001; Cohen’s d= −1.125) than the low SRS-2 group. There were no significant differences in SDB, morning symptoms, sleep habits, or sleep bruxism between the 2 groups.
Dietary and meal habits
The scores for dietary and meal habits are presented in Table 3. There were no significant differences between the 2 groups regarding the amount of food consumed per meal, eating speed or picky eating. However, scores for standing up and playing during meals were significantly higher in the high SRS-2 group than in the low SRS-2 group (p < 0.01; Cramer’s V = 0.410).
Orofacial functional scores
Results of the oral examination and the orofacial functional scores are displayed in Table 4. There were no significant differences between the 2 groups regarding the dmft/DMFT index, Hellman’s dental age or incompetent lip seal. In the orofacial functional evaluation, owing to the gagging reflex, occlusal force could not be measured in 1 child in the high SRS-2 group, maximum tongue pressure could not be assessed in 2 children in the high SRS-2 group, and masticatory performance could not be evaluated in 1 child in the low SRS-2 group. There were no significant differences in the occlusal force, maximum tongue pressure or lip-closing strength between the 2 groups. However, masticatory performance was significantly lower in the high SRS-2 group than in the low SRS-2 group (p < 0.05; Cohen’s d = 0.773).
Correlation of the SRS-2 scores with assessment items
Table 5 presents the correlation coefficients of the SRS-2 scores with orofacial functional and sleep assessment items. Regarding the sleep disorder items, restless legs syndrome (r = 0.496; 95% CI: 0.260–0.675, p < 0.001), SDB (r = 0.393; 95% CI: 0.137–0.600, p < 0.01), morning symptoms (r = 0.310; 95% CI: 0.044–0.536, p < 0.05), nighttime awakenings (r = 0.557; 95% CI: 0.338–0.719, p < 0.001), insomnia (r = 0.461; 95% CI: 0.218–0.651, p < 0.001), excessive daytime sleepiness (r = 0.548; 95% CI: 0.326–0.713, p < 0.001), daytime behavior (r = 0.570; 95% CI: 0.354–0.728, p < 0.001), irregular/delayed sleep phase (r = 0.440; 95% CI: 0.193–0.635, p < 0.001), the sum of sleep scores (r = 0.569; 95% CI: 0.353–0.727, p < 0.001), and sleep bruxism (r = 0.425; 95% CI: 0.175–0.624, p < 0.01) showed a significant correlation with the SRS-2 T score.
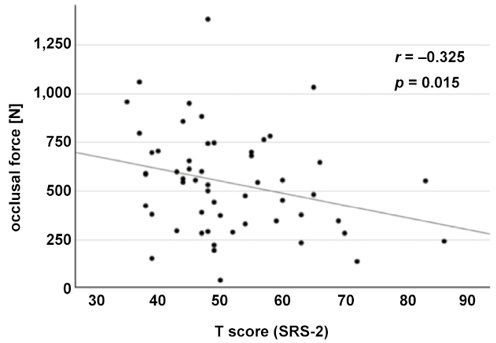
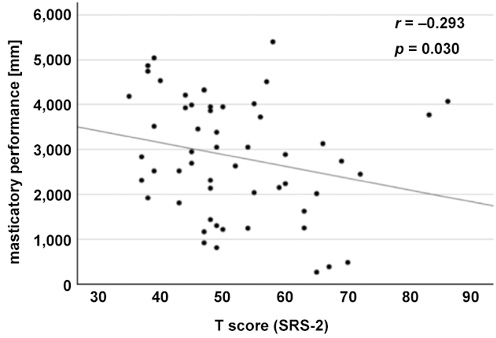
Additionally, in the orofacial functional items, occlusal force (r = −0.325; 95% CI: −0.549–−0.057, p < 0.05) and masticatory performance (r = −0.293; 95% CI: −0.524–−0.022, p < 0.05) were significantly negatively correlated with the SRS-2 T score (Figure 2,Figure 3). With regard to dietary and meal habits, picky eating (r = 0.324; 95% CI: 0.058–−0.546, p < 0.05) and standing up and playing during meals (r = 0.390; 95% CI: 0.134–0.597, p < 0.01) were positively associated with the SRS-2 T score.
Correlation of dietary and meal habits and orofacial factors with sleep disorder scores
The correlation of dietary and meal habits and orofacial factors with sleep disorder scores is presented in Table 6. Excessive food intake was associated with SDB (r = 0.457; 95% CI: 0.212–0.647, p < 0.001), excessive daytime sleepiness (r = 0.307; 95% CI: 0.040–0.533, p < 0.05), irregular/delayed sleep phase (r = 0.311; 95% CI: 0.044–0.536, p < 0.05), the sum of JSQ-ES T scores (r = 0.304; 95% CI: 0.037–0.531, p < 0.05), and sleep bruxism (r = 0.276; 95% CI: 0.007–0.509, p < 0.05), while insufficient food intake was significantly correlated with SDB (r = −0.284; 95% CI: −0.515–−0.015, p < 0.05). Eating too fast showed significant associations with restless legs syndrome (r = 0.267; 95% CI: −0.003–0.501, p < 0.05), insomnia (r = 0.301; 95% CI: 0.033–0.528, p < 0.05), excessive daytime sleepiness (r = 0.328; 95% CI: 0.063–0.550, p < 0.05), and sleep bruxism (r = 0.284; 95% CI: 0.015–0.515, p < 0.05). Additionally, picky eating demonstrated correlations with restless legs syndrome (r = 0.289; 95% CI: 0.020–0.519, p < 0.05), nighttime awakenings (r = 0.402; 95% CI: 0.148–0.607, p < 0.01), daytime behavior (r = 0.395; 95% CI: 0.140–0.601, p < 0.01), irregular/delayed sleep phase (r = 0.301; 95% CI: 0.034–0.528, p < 0.05), and the sum of JSQ-ES T scores (r = 0.326; 95% CI: 0.061–0.548, p < 0.05), while standing up and playing during meals was related to restless legs syndrome (r = 0.301; 95% CI: 0.038–0.532, p < 0.05) and sleep bruxism (r = 0.273; 95% CI: 0.003–0.506, p < 0.05). Furthermore, masticatory performance was associated with daytime behavior (r = −0.277; 95% CI: −0.511–−0.005, p < 0.05).
Discussion
The results of our study reveal that children with signs of ASD have problems with orofacial function as well as with eating habits and sleep. Although healthy children who had not been diagnosed with neurodevelopmental disorders by a doctor participated in the present study, 23.2% of the participants had the SRS-2 T scores of 60 or more (Table 1). In the SRS-2, a T score of 60 or above is typically associated with clinically significant ASD.24 The high SRS-2 group had a T score of 68.4 ±8.0, indicating a population with moderate ASD symptoms, while the low SRS-2 group had a T score of 46.6 ±6.2, reflecting a population without clinically significant ASD. These results show that the 2 groups differed significantly in the severity of ASD signs. High-functioning individuals with ASD are often diagnosed at a later age than recommended and may remain undiagnosed and latent.3 Additionally, some of the participants in the present study were referred by general dentists to the Pediatric Dentistry Clinic due to uncooperative behavior during dental treatment. Therefore, it is likely that there was a certain amount of latent ASD reflected in the SRS-2 T scores of the participants. However, uncooperative behavior during dental treatment may be an indicator of developmental problems, including orofacial dysfunction and sleep disorders. In this regard, the generalizability of the present results to the typical pediatric population should be interpreted with caution.
The high SRS-2 group had significantly higher T scores than the low SRS-2 group for the majority of items related to sleep disorders (Table 2). The difference in the T scores between the high SRS-2 group (63.0 ±10.0) and the low SRS-2 group (50.6 ±11.3) can be regarded as clinically significant.26 Most children with ASD have sleep problems, and their sleep is characterized by reduced total sleep time, longer sleep latency and decreased sleep efficiency,5, 6, 7 which was reflected in the present results for nighttime awakenings, insomnia, excessive daytime sleepiness, daytime behavior, and irregular/delayed sleep phase, all of which were considered clinically significant.26 Additionally, most scores for the sleep disorder items were significantly positively correlated with the SRS-2 T scores (Table 5), indicating that the severity of these sleep problems is associated with the severity of ASD symptoms, as found in a previous study.9 Furthermore, the T scores for SDB were significantly positively correlated with the SRS-2 T scores (Table 5), which suggests that even among healthy children, those with signs of ASD tend to have a certain level of SDB. This association with signs of ASD may be evident in morning symptoms as well (Table 2,Table 5).
Although the frequency of eating too fast and picky eating was higher in the high SRS-2 group compared to the low SRS-2 group, no significant differences were observed. However, standing up and playing during meals was reported significantly more frequently in the high SRS-2 group (Table 3). Additionally, picky eating and standing up and playing during meals were significantly and positively correlated with the SRS-2 T score (Table 5). Limited food preference is known to be the most common feeding behavior in children with ASD.11 Our results suggest that the severity of ASD symptoms is associated with the severity of picky eating. Additionally, leaving the table is one of the most frequently demonstrated disruptive mealtime behaviors in children with feeding problems and can indicate food refusal.38, 39 In the present study, standing up and playing during meals may also be attributed to food refusal. The developmental stage from age 3 to 6 is fundamental to physiological changes in growth and adaptability, and habits established during this time can persist throughout an individual’s entire life.40 Children with ASD demonstrate sensory preferences and difficulty with motor control.38, 39 These sensitivities can be associated with a restricted intake of tolerated foods as well as low masticatory performance in the studied age group.
Few studies have investigated the relationship between neurodevelopment and orofacial function in children, and little quantitative data is available on oral function in children with ASD. The strength of the present study lies in the analysis of dynamic orofacial function (masticatory performance) and static orofacial function (lip pressure, tongue pressure) in early elementary school children with signs of ASD. The present study showed that masticatory performance was significantly lower in the high SRS-2 group than in the low SRS-2 group (Table 4). Although occlusal force, maximum tongue pressure and lip-closing strength were lower in the high SRS-2 group than in the low SRS-2 group, there were no significant differences in these values between the 2 groups, nor in the dmft/DMFT scores and the frequency of incompetent lip seal. Additionally, occlusal force and masticatory performance were significantly negatively correlated with the SRS-2 T score (Table 5). Although children with ASD frequently present with orofacial dysfunction characterized by excessive drooling and an open mouth at rest,13 the condition is not necessarily the same, and the pathophysiology is not uniform, as there is a great deal of individual variation due to differences in body size as well as in the tension and relaxation of each muscle. However, mastication, due to its complex coordinated movement involving the perioral and masticatory muscles, can represent a common problem with orofacial function among children with signs of ASD. Focusing on developmental coordination disorder, which occurs in approx. 80–90% of children with ASD,41 may be useful for understanding the association between whole-body and orofacial movements in future research.
Orofacial conditions, including tonsillar hypertrophy, adenoid hypertrophy, retrognathic mandible, and lingual abnormalities, have been linked to sleep problems, especially OSA.42, 43 Additionally, recent studies have reported that dietary intake and breakfast habits are associated with sleep disorders in children.44 In the present study, the amount of food consumed per meal, eating speed, picky eating, and standing up and playing during meals were significantly related to sleep problems, although these items were binary or categorical variables (Table 6). The amount of food consumed per meal and eating speed may be indirectly related to sleep problems through obesity,45 and picky eating and eating habits may be indirectly associated with sleep disorders through neurodevelopment. However, considering that chewing ability is also related to sleep disorders (Table 6), eating problems may be an indicator of oral function, which is closely related to sleep and neurodevelopment.46 Furthermore, sleep problems in children can be negatively correlated with oral function and oral hygiene47, 48; thus, further research is needed to investigate the relationships between oral health, sleep health and neurodevelopment.
Limitations
The present study had some limitations that should be considered. First, this cross-sectional study analyzed data from early elementary school children aged 6–9 years, with a relatively small sample size. To mitigate this limitation, simplified measurements were employed to evaluate orofacial function. These multiple measurements can be challenging in uncooperative subjects. The results were based on exact and objective data with only a few dropouts; however, sample bias (e.g., the study population was not representative of the general population and the study did not employ a strictly controlled design) could not be avoided, and the generalizability to the typical pediatric population should be interpreted with caution. Additionally, the multiple measurements may have caused fatigue in the children, and the values should be analyzed considering this factor. Based on the results of this study, future cohort and comparative studies are warranted to elucidate the relationship between oral function and sleep in children with developmental difficulties. Second, all factors related to sleep disorders and signs of ASD in the present study were evaluated based exclusively on scaled quantitative assessment questionnaires, and these judgments were not definitive. However, subjective assessments using questionnaires may be more closely related to specific clinical symptoms than objective sleep assessments such as polysomnography.49 Additionally, it is recommended that routine sleep screening be incorporated into dental clinical practice because there could be a specific subgroup of SDB patients that may go undetected in general pediatric clinics.23 The screening for ASD with the SRS-2 in this study has not been validated against clinical observational diagnoses such as the Autism Diagnostic Observation Schedule, Second Edition (ADOS-2),3 and participants may have been misclassified as having other disorders that cause similar symptoms. Nevertheless, questionnaire-based assessment remains the only strategy for the screening of sleep disorders and signs of ASD in a pediatric dentistry clinic, and it is a common strategy, especially for early elementary school children. Signs of ASD and sleep disorders are considered to have been assessed adequately in the present study. Third, although we demonstrated relationships between signs of ASD and orofacial function as well as sleep disorders, these connections do not indicate causation but merely correlation. Hypotonia, impaired coordination, and the resulting mouth breathing and maxillofacial underdevelopment, which are characteristic of children with ASD, may be associated with orofacial dysfunction and sleep problems.14, 50 A detailed analysis that considers individual factors such as age and socioeconomic factors will likely clarify the underlying mechanisms. Fourth, multiple regression analyses could not be conducted, and some factors and biases could not be considered due to the small sample size. Additionally, many statistical tests in our study were performed as exploratory analyses, and the statistical significance level was not adjusted. Therefore, insufficient power and statistical errors may exist, and the results should be interpreted with caution. Nevertheless, the present study quantified dynamic orofacial function as well as static orofacial function in early elementary school children, revealing that children with signs of ASD have low masticatory performance, a type of dynamic oral function, and indicated the importance of focusing on functional aspects as well as behavioral, psychological and nutritional aspects in ASD-related eating problems. Further studies focusing on orofacial and neurodevelopmental conditions would be useful for assessing vital functions in children with and without signs of ASD.
Conclusions
Within the limitations of this experimental study, it can be concluded that low masticatory performance, as well as behavioral and psychological factors, may contribute to feeding issues in early elementary school children with signs of ASD. Additionally, the severity of ASD symptoms is associated with the severity of problems with orofacial function, feeding behavior and sleep. The results of this study underscore the importance of interventions targeting orofacial function and sleep disturbances in children with signs of ASD.
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of the Graduate School of Dentistry at the University of Osaka, Japan (approval No. R3-E5). Written informed consent for study participation was obtained from all parents/guardians, and verbal agreement and written informed assent were obtained from all children.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.