Abstract
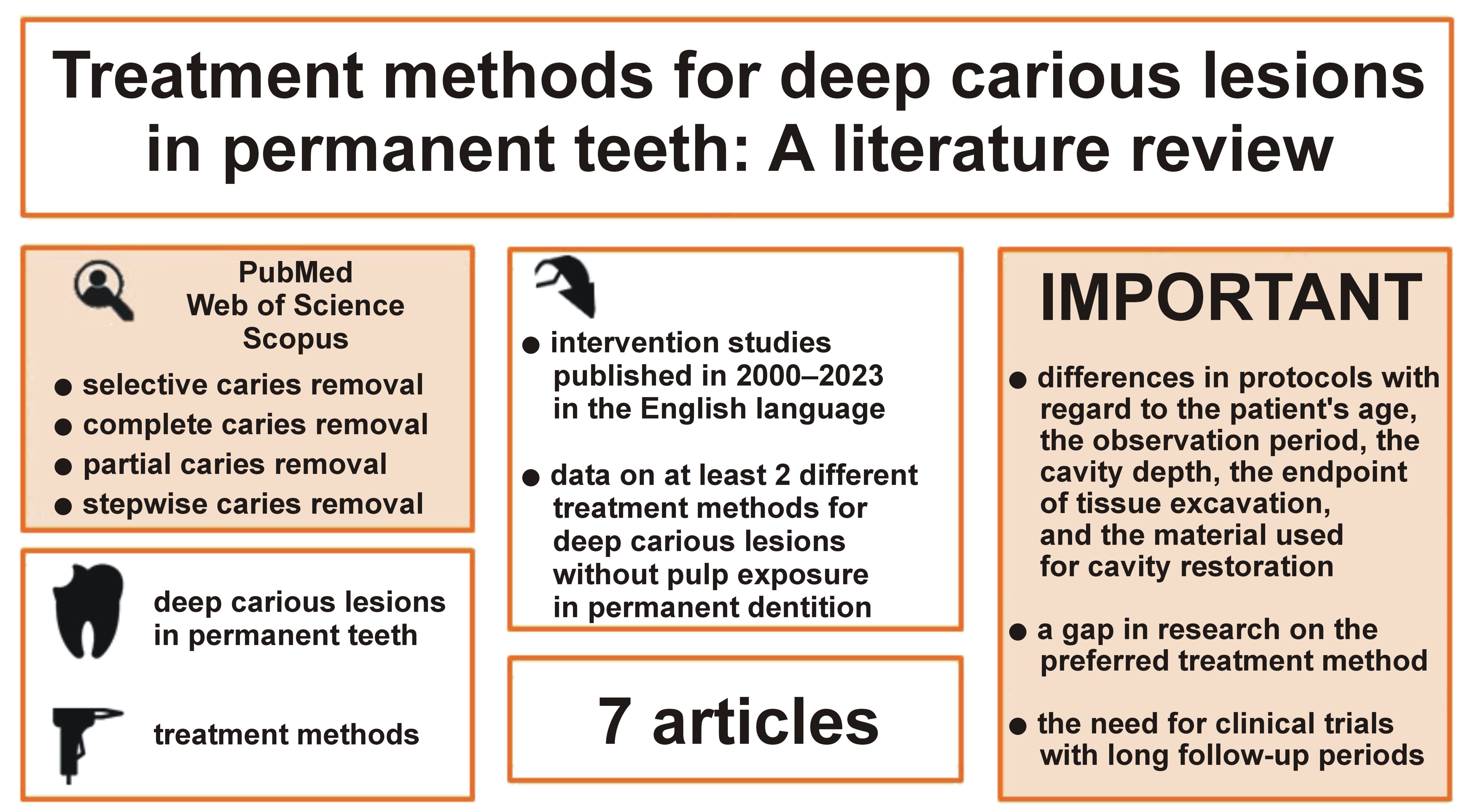
Complete removal of carious dentin is currently regarded as overtreatment, and the stepwise (two-step) or selective (one-step) caries removal procedures are recommended. This literature review was aimed to summarize research findings on deep caries lesion management approaches in permanent teeth, to determine which method provides better outcomes and to identify possible research gaps. Only intervention studies published between 2000 and 2023 in the English language were considered. The PubMed, Web of Science and Scopus databases were searched in September 2023, and 7 relevant records were considered for assessment. This literature review has shown that the number of studies comparing the methods of deep caries lesion management is limited, and the significant differences in protocols regarding the cavity depth, the endpoint of tissue excavation and the material used for cavity restoration indicate the need for the standardization of treatment. Both one- and two-stage caries removal significantly reduce the risk of pulp exposure in comparison with complete excavation; however, further clinical trials with long follow-up periods are necessary to determine which caries removal approach, stepwise or selective, provides better outcomes.
Keywords: permanent teeth, selective caries removal, stepwise caries removal, complete caries removal, deep caries treatment
Introduction
The traditional approach to caries treatment is based on the concept of complete removal of carious dentin, leaving only hard dentin that meets tactile and color criteria.1, 2 The rationale for the above is to stop decay by eliminating bacteria, and to remove soft and demineralized dentin to provide a solid base for the restoration.1, 2 This approach has been used for decades and is still preferred by numerous dentists worldwide.3, 4 However, contemporary dentistry regards such cavity preparation as overtreatment.5, 6 Non-selective caries removal increases the risk of pulp exposure and pulp damage due to the diffusion of toxic compounds through the thin remaining dentin barrier over the pulpal wall. This contradicts one of the fundamentals of caries treatment, namely the preservation of pulp vitality.7 In addition, non-selective caries removal may weaken the tooth structure and increase the tooth’s susceptibility to damage.2 Current evidence-based recommendations for the treatment of carious lesions state that it is not necessary to remove the entire carious tissue from the pulpal wall.1, 5 According to the minimal intervention dentistry (MID) guidelines, treatment should be restricted to the removal of the infected dentin only.8 The remineralization of affected dentin can be achieved by the action of odontoblasts or by the diffusion of fluoride, calcium and phosphate ions from dental materials.8
The nomenclature and modern techniques for caries management have recently been discussed in the literature.1, 5, 6, 8, 9, 10 There are 2 main approaches: two- and one-step treatment. The 1st method – stepwise caries removal (SwCR) – comprises 2 stages. First, carious tissue is removed down to soft dentin and the cavity is filled with a temporary material with a remineralizing effect for a certain period of time. The amount of the removed carious tissue should be sufficient to allow the placement of a durable restoration.5 During the re-entry visit, the cavity is reopened for the removal of the remaining decayed tissues up to firm dentin and the final filling is provided. The response of the pulp–dentin complex after treatment can be induced by the effect of dental materials (liners, temporary and permanent restorations) and several mechanisms, including the remineralization of dentin, the production of tertiary dentin and the reduction of post-operative pulpitis.11, 12 The 2nd approach – selective caries removal (SCR), also known as incomplete, partial or minimally invasive, consists in one-visit treatment. The idea is to leave carious (leathery/firm or soft) tissue on the pulpal wall and to seal the cavity with a permanent restoration. Both methods strictly require the preparation of external cavity walls up to sound enamel and hard dentin.1, 2, 5, 9
Dental treatment should also be considered in terms of cost-effectiveness. There is evidence that the SCR approach saves up to 40% of costs and is associated with high success rates.13, 14, 15 Stepwise excavation involves additional treatment costs, as a reopening visit is required; besides, some failure, such as a tooth fracture or damage to a temporary filling, may occur between treatment visits.13 Schwendicke et al. found that most unfavorable outcomes in stepwise excavation were the result of the cavity reopening.16
The non-complete caries removal techniques were previously recommended for uncooperative and disabled children with severe dental caries, and as atraumatic restorative treatment (ART) in underdeveloped countries with a limited access to adequate dental equipment.10 Recent research studies on the attitudes of dentists and dental students to deep carious lesion management show an increasing trend toward the implementation of modern approaches to the treatment of permanent teeth in the general population. On the other hand, those concepts have not yet been adopted by many dental practitioners; especially those with longer work experience are more likely to perform non-selective cavity preparation.3, 4, 17, 18
There are several literature reviews on different aspects of incomplete carious dentin removal.2, 7, 8, 19, 20, 21 However, there is only one paper comparing the effectiveness of the stepwise and selective caries removal techniques,21 and no review specifically focuses on permanent dentition. Therefore, the aim of this review was to summarize research findings on deep caries lesion management approaches in permanent teeth and to identify possible research gaps.
Material and methods
A literature review was performed to assess how the research comparing different approaches to deep caries lesion management in permanent teeth has been conducted, which method provides better outcomes and what are the research gaps in this field. Two research questions were formulated: “Which approach, stepwise/selective caries removal vs. non-selective caries removal, provides better outcomes in permanent teeth?”; and “Which approach, stepwise caries removal vs. selective caries removal, provides better outcomes in permanent teeth?”. The main criterion for including records in the present literature review was: articles published in peer-reviewed journals that described the results of at least 2 different treatment methods for deep carious lesions without pulp exposure in permanent dentition. Intervention studies published between 2000 and 2023 in the English language were considered. The exclusion criteria were as follows: non-research articles, such as protocols, books, proceedings, reviews, or letters to editors.
The keywords for search were developed by 3 authors (SB, KG and JB) based on a preliminary analysis of the literature. The following terms were used as a search strategy: ((((((((selective caries removal) OR (complete caries removal)) OR (partial caries removal)) OR (stepwise caries removal)) AND (permanent teeth)) OR (permanent dentition)) AND (deep caries)) NOT (case study)) NOT (review). The PubMed, Web of Science and Scopus databases were searched on September 8–9, 2023, to find relevant studies. This search was supplemented by the analysis of the reference lists of the retrieved articles and gray literature. The records were processed in EndNote Web (Clarivate™, London, UK) to remove duplicates. The results were analyzed by 3 authors (JB, KG and SB) according to the titles and abstracts to select relevant articles. Other authors (RŁ and ER) were asked for their opinion in case of doubts as to whether the article should be included in the analysis or not.
In the following step, the data for the analysis was collected using an Excel spreadsheet (Microsoft Office Professional Plus 2019; Microsoft Corporation, Redmond, USA). It comprised information on the authors and their affiliation (country), the year of publication, the study type, the number of cases, the patients’ age, the tooth type, the criteria for caries depth assessment, the kind of intervention, the caries treatment procedure, the liner and the material used for restoration, the cavity re-entry period (if applicable), the outcome criteria, the follow-up period, and the authors’ main conclusions. The form for data charting was developed by JB and RŁ, and then accepted by all authors. The analysis of the articles, the synthesis of the obtained results and data charting were carried out by 2 authors (KG and SB), and then another 2 authors (JB and ER) reviewed the records obtained.
Results
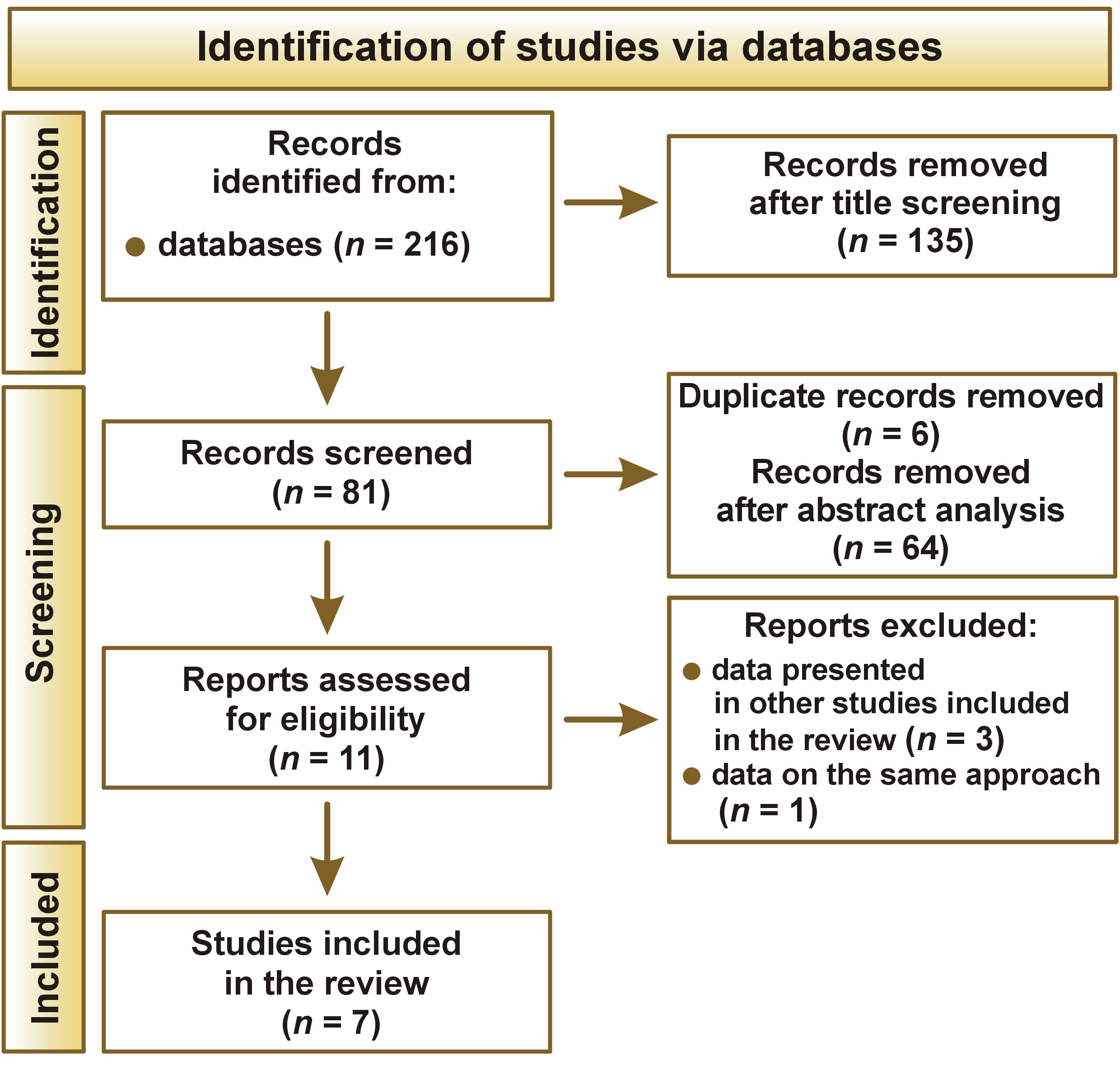
Figure 1 presents the literature search flow diagram. An initial search showed 216 articles (PubMed – 99, Web of Science – 62, Scopus – 55). Manual search did not reveal any additional articles. After examining the titles, 81 articles remained (PubMed – 35, Web of Science – 23, Scopus – 23). After applying the de-duplication function in the citation management software EndNote Web, 75 records were left. Based on the analysis of the abstracts, 11 manuscripts were selected for evaluation. However, after a detailed analysis of the content of the articles, 3 of them were excluded, since they concerned prospective studies, and their final results were presented in the papers by Bjørndal et al.22 and Maltz et al.23 One paper was excluded due to the evaluation of 2 protocols for the SCR method.24
The final number of records was 7 (Table 1).22, 23, 25, 26, 27, 28, 29 Among the studies included in this review, 1 was a multicenter Scandinavian study,22 2 studies were from India,25, 28 and others were from Brazil,23 Egypt,26 Turkey,27 and Pakistan.29 All papers were published between 2017 and 2021. Five records compared modern caries removal approaches and CCR (Table 2).22, 25, 27, 28, 29 Three of those studies applied the stepwise method22, 27, 28 and in the other two, SCR was used.25, 29 Further 2 studies summarized in Table 3 compared one- and two-step caries removal with each other.23, 26
Each study was conducted as a randomized clinical trial (RCT), but there were many differences in the study protocols. With regard to the patients’ age, most studies were conducted on adults, but some included also the permanent teeth of young children (>6 years)23 and teenagers (>14 years).25 Another difference was the group of teeth – some studies were conducted exclusively on molars or on lateral teeth,23, 25, 26, 28, 29 while other studies included whole dentition.22, 27 A deep carious lesion was diagnosed radiographically, but the definition of such a lesion varied from the involvement of ≥½ of the dentin layer to ¾ or more. One study defined a deep carious lesion as involving ⅔ of dentin.26
The protocols of intervention are described in detail in Table 2 and Table 3. During complete carious dentin removal, the decayed tissues were removed to hard dentin with or without the use of Caries Detector dye, and then the tooth was restored with a glass-ionomer cement (GIC) base and a resin composite/amalgam filling.22, 25, 27, 28, 29 Manhas et al. sealed the pulpal wall with calcium hydroxide, and followed with temporary restoration with zinc oxide–eugenol cement (ZOE).28 At the revisit, calcium hydroxide was left on the pulpal wall and the tooth was restored with a resin composite.28 Stepwise caries removal was performed by hand excavation or using a bur to soft dentin or firm dentin.22, 23, 27, 28 In this method, the remaining carious dentin was usually sealed with calcium hydroxide cement, and GIC or modified ZOE were used for a temporary filling. Only Labib et al. sealed the cavity directly with GIC.26 The re-entry visit was carried out between 2 and 6 months, and it included the removal of the temporary filling, the complete removal of carious tissues (to hard or firm dentin) and the final filling of the cavity. In the SCR technique, most protocols consisted in removing the infected dentin down to a soft, moist layer on the pulpal wall, and the final restoration was made with GIC and a resin composite/amalgam.23, 25, 26, 29
The follow-up period was 1 year, 18 months, 62 months, or 5 years.22, 23, 25, 26, 27, 28, 29 The outcome criteria were based on the response of pulp and periapical tissues, and they included: a positive response to pulp testing; the absence of spontaneous pain and pain on palpation/percussion; the absence of fistulae/swelling; and a normal radiological image of the periapical area. The overall success rate of the stepwise method was higher or similar to that of CCR.22, 27, 28 The selective removal of carious tissues showed a similar outcome as compared to teeth with complete excavation (after excluding teeth with pulp exposure during excavation).25, 29 However, in the long-term observations lasting around 5 years, the effectiveness rate of SwCR was lower than in short-term observations, and ranged, after excluding teeth with uncompleted treatment, between 60.2% and 75%.22, 23 Taking into account stepwise and selective excavation, the studies showed comparable results.23, 26 Maltz et al. concluded that the effectiveness of the stepwise technique was highly influenced by the cases without complete treatment.23 In all the studies reporting the level of pulp exposure, both one- and two-stage caries removal significantly reduced the risk of such events in comparison with complete excavation.22, 25, 28, 29
Discussion
This literature review showed that the number of studies comparing different methods of removing carious dentin in permanent dentition is limited. The evaluated studies varied in terms of important factors that may influence the outcome (the patient’s age, the threshold of deep caries, the restorative method, the observation period). However, all records showed that the stepwise and selective approaches had a success rate at least comparable to the traditional caries removal technique. There were fewer cases of pulp exposure during one- and two-step caries removal than during complete excavation. On the other hand, due to a small number of records, no clear conclusion could be drawn as to which method, the one- or two-stage approach, is more beneficial for permanent dentition. No statistically significant differences in the success rates were found in the studies comparing modern approaches. Therefore, there is a gap in research on the preferred treatment method, and more clinical trials with long follow-up periods should be conducted. However, there are opinions in the literature that one-step incomplete excavation reduces the risk of failure as compared to two-step removal.16
The depth of carious lesions should be taken into account when choosing the treatment method, since the dentin thickness and permeability can influence the outcome. However, a clinical assessment of the residual dentin thickness is difficult.7 Recent recommendations define deep caries as a lesion reaching the inner third or quarter of dentin on radiographs, with the risk of pulp exposure.5 The European Society of Endodontology (ESE) has proposed a division into deep and very deep lesions.30 The former are diagnosed when a carious lesion reaches up to a quarter of dentin on a radiograph, but a zone of radiopaque dentin separating the demineralized tissue from pulp can be found. Very deep caries means the presence of demineralized dentin throughout the thickness of the pulpal wall, with a high probability of bacterial invasion within tertiary dentin and even pulp. Thus, finding features of a very deep cavity on a radiographic examination may be a disqualifying factor in choosing the SCR method.7 All the studies included in the present review used the radiographic evaluation to diagnose deep caries, but authors established different thresholds – from ½ to ¾ of the dentin layer, which made it difficult to compare the effectiveness of these methods.22, 23, 25, 26, 27, 28, 29
Other differences between the evaluated studies comprised the method for removing carious dentin, the endpoints of cavity preparation (soft or firm dentin) and the restoring method. So far, no consensus has been reached as to where to stop tissue excavation and which material is most suitable for filling the cavity during non-invasive caries removal.31 However, the hand excavation of decomposed dentin on the pulpal wall seems to be more appropriate. Mechanical removal with round metal burs leads to excessive cavity preparation. Lim et al. emphasized that the determination of the level of removal of the involved dentin should be based on the dentin texture rather than its color.6 The amount of the excavated infected tissue is one of the major concerns of the partial caries removal approach. According to Maltz et al., the recommended method for deep carious lesions is selective removal to soft dentin.1 The evaluated studies confirmed that soft dentin did not have to be completely removed from the pulpal wall to maintain a long-term positive outcome.
In the analyzed studies, the products containing calcium hydroxide were mainly used in the stepwise technique. The sealing of carious dentin with calcium hydroxide reduces the number of microorganisms even below the level found in dentin after the conventional caries removal.12 However, according to a recent recommendation, there is no need to seal soft dentin with cavity liners.1 In contrast, the cavities treated by non-selective caries removal were usually restored with the combination of GIC and a resin composite. Glass-ionomer cement has a well-known high remineralization potential. Other materials, such as mineral trioxide aggregate (MTA), BioCeramic, silver diamine fluoride, propolis, or hesperidin, were tested as cavity sealers in SCR.32, 33 However, Gözetici-Çil et al. found that calcium silicate cement used in SCR to soft dentin provided no additional benefit.24
The tooth’s resistance to occlusal forces was not investigated in the studies included in this review. Undoubtedly, this aspect should be taken into account when planning treatment. Leaving non-hard dentin can be a factor affecting the biomechanical properties of the tooth tissue and restoration. There are reports stating that teeth after SCR have lower fracture resistance and increased deflection of cusps; therefore, restorative materials that can support the tooth structure should be chosen.34 On the other hand, Scholz et al. found that SCR did not impair the marginal integrity of the restoration.35
Limitations
This review has some limitations. Only studies comparing at least 2 different approaches were included; therefore, some publications confirming the advantages of stepwise or selective caries removal were excluded from the analysis. Papers evaluating outcomes in primary dentition were not included. The decision to exclude them from the assessment was based on the fact that the risk of failure is higher for deciduous teeth due to difficulty in proper sealing and the short lifespan of deciduous teeth, which excludes the possibility of a long-term evaluation.1 The small number of studies available for comparison and differences in the study design highlight the need for standardized long-term clinical trials on treatment approaches for deep caries lesions in permanent dentition.
Conclusions
This literature review has shown that the number of studies comparing the methods of deep caries lesion management is limited, and the significant differences in protocols regarding the cavity depth, the endpoint of tissue excavation and the material used for cavity restoration indicate the need for the standardization of treatment. Further clinical trials with long follow-up periods are necessary to determine which caries removal approach, stepwise or selective, provides better outcomes.
Ethics approval and consent to participate
Not applicable.
Data availability
The datasets supporting the findings of the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.