Abstract
Untreated sleep bruxism (SB) can cause damage to the stomatognathic system, potentially reducing academic performance in children and negatively affecting their quality of life. Occlusal splints are considered the gold standard for the treatment of bruxism in children; however, they present many limitations, prompting the search for alternative therapies. Laser therapy has been proposed as a more favorable, painless and cost-effective treatment option for pediatric patients. Therefore, the aim of this study was to evaluate the effectiveness of photobiomodulation therapy (PBMT) and occlusal splints in the treatment of bruxism in children.
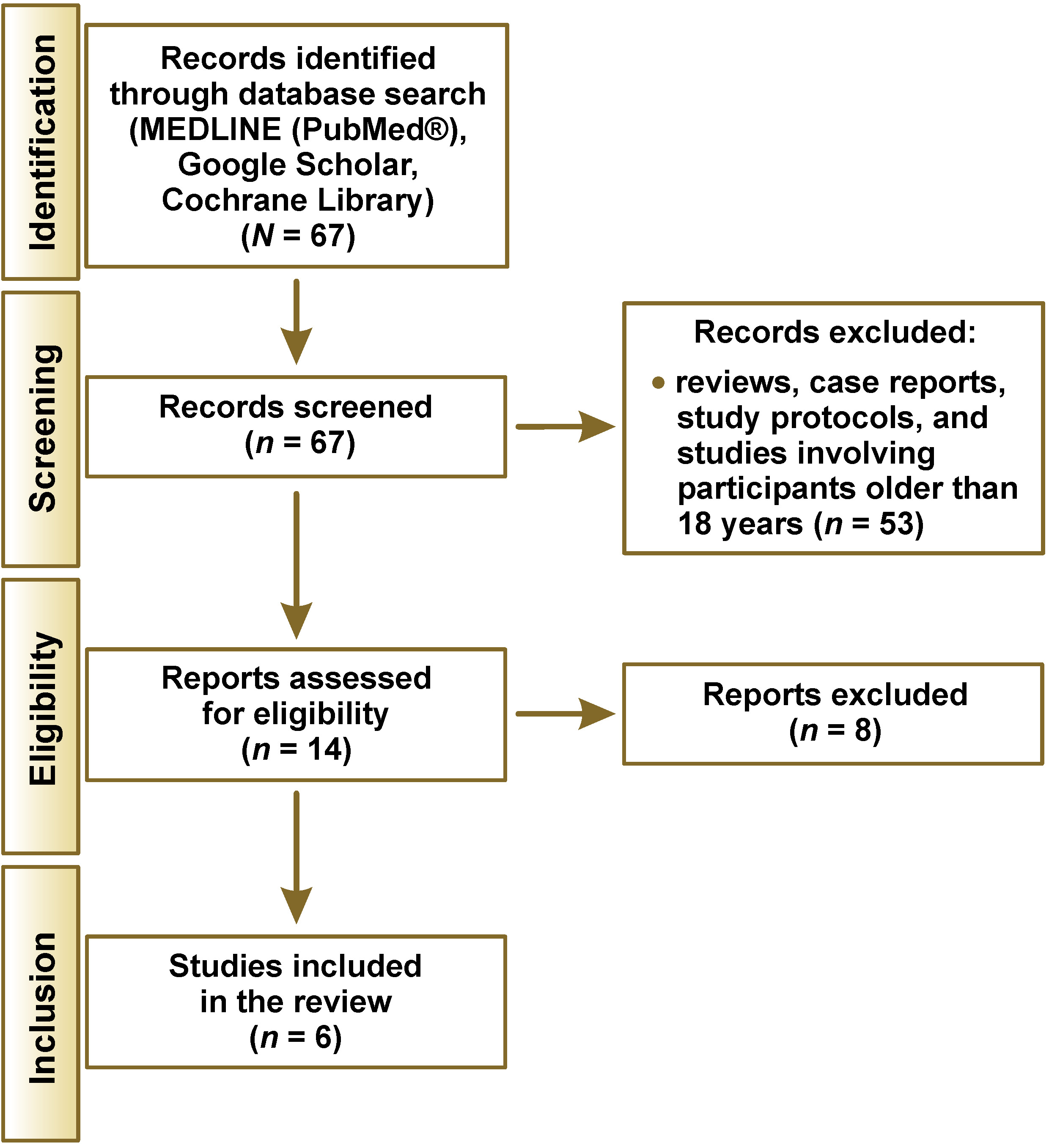
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines. Studies were identified through searches of the following databases: MEDLINE (PubMed®); Google Scholar; and the Cochrane Library. The review included articles published between January 2010 and June 2023. Studies evaluating the treatment of bruxism using occlusal splints and/or PBMT in participants under 18 years of age were included.
A total of 67 articles published in English were identified. After applying the eligibility criteria and assessing study quality using the Cochrane risk-of-bias tool, 6 studies were included in the final analysis. Of these, 4 investigated various types of occlusal splints, while 2 compared PBMT with occlusal splints. The papers also examined diagnostic methods, treatment outcomes, salivary cortisol levels, and dopamine levels.
Occlusal splints have limited effectiveness in managing the signs and symptoms of bruxism. Photobiomodulation therapy shows potential as a treatment method, but its effectiveness remains inconclusive. Due to the limited number of available studies, definitive conclusions cannot be drawn, and further research is necessary.
Keywords: photobiomodulation, occlusal splint, bruxism, children, therapy
Introduction
Bruxism is a repetitive, non-functional activity of the jaw muscles characterized by clenching or grinding of the teeth and/or by thrusting or bracing the mandible.1, 2 Two types of bruxism are distinguished based on the state of occurrence. When it occurs during wakefulness, it is referred to as awake bruxism, also known as secondary bruxism or daytime bruxism, whereas when it occurs during sleep, it is termed sleep bruxism (SB), also known as primary or nighttime bruxism.1, 2 The type of bruxism is typically determined through patient history and physical examination. Diagnostic tools such as the Diagnostic Criteria for Temporomandibular Disorders (DC/TMD), Oral Behaviors Checklist (OBC), can be used for the assessment of bruxism.3 Additionally, polysomnography is considered a reliable method for diagnosing sleep-related conditions.4
Sleep bruxism is common among children and adolescents, with reported prevalence rates ranging from 3.5% to 40.6%.5 Individuals who experience SB during childhood are more likely to continue experiencing it in adulthood.6 Although early management of bruxism is important to prevent its negative consequences, establishing a definitive diagnosis remains challening.7, 8 Untreated SB may cause teeth attrition, headaches, muscle pain, temporomandibular disorders (TMD), periodontal diseases, and damage to the stomatognathic system. Moreover, it may negatively affect academic performance and overall quality of life in children and adolescents.8
The exact etiology of SB in children remains unknown.9 However, bruxism is considered a multifactorial condition that may be associated with certain behavioral and psychological factors.10 Other contributing factors include genetic predisposition, malocclusion, occlusal factors, arterial hypertension, nutritional deficiencies (e.g., 25-hydroxyvitamin D deficiency), oral habits, sleeping habits, allergies, respiratory problems (apnea, snoring), alterations in neurotransmitters (e.g., dopamine), and overall sleep quality.11, 12, 13, 14, 15, 16
Awake bruxism is often associated with other parafunctional habits, such as excessive gum chewing, biting pens or pencils, or nail biting. These behaviors may begin in early childhood and persist throughout life, often intensifying during periods of stress and being associated with increased muscle tension.17
Various treatment approaches for bruxism have been suggested, including dental, psychobehavioral and pharmacological interventions. Pharmacological methods involve the use of medications such as beta-blockers, anticonvulsants, antidepressants, dopamine agents, and muscular relaxants.18, 19 Although drugs such as buspirone, fluoxetine and diazepam have been investigated, they have not demonstrated effectiveness in the treatment of bruxism, and concerns have been raised regarding their potential adverse effects.20, 21, 22
Botulinum toxin has also been proposed as a treatment for SB; however, it has not demonstrated short-term efficacy.23 Biofeedback has been used to manage masticatory muscle activity, with studies showing a significant reduction in muscle activity associated with its use.24 Similarly, injectable platelet-rich fibrin (I-PRF) has exhibited efficacy in alleviating symptoms of internal temporomandibular joint disorders.25
Occlusal splints are considered the gold standard for the management of bruxism in both children and adults.26 Among them, rigid occlusal splints are the most frequently used.27 However, these appliances have many limitations, which has encouraged the exploration of alternative treatment methods. Recently, photobiomodulation therapy (PBMT) has emerged as a non-pharmacological approach for the treatment of bruxism, following evidence of its effectiveness in patients with TMD.28
According to the American Society of Laser Medicine and Surgery (ASLMS), “photobiomodulation therapy is a form of light therapy that utilizes non-ionizing forms of light sources including lasers, LEDs and broadband light, in the visible and near-infrared spectrum”.29 Photobiomodulation therapy is used to accelerate the healing process by stimulating cells and increasing blood circulation.30, 31 Moreover, PBMT exhibits vasodilatory, analgesic and anti-inflammatory effects.31
The aim of this study was to evaluate the effectiveness of PBMT and occlusal splints in the treatment of bruxism in children.
Material and methods
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines for reporting systematic reviews.32 The terminology and definitions used were consistent with the current international consensus on bruxism.2
Search strategy
Studies were identified through searches of the following databases: MEDLINE (PubMed®); Google Scholar; and the Cochrane Library. Articles published between January 2010 and June 2023 were taken into consideration. The following keywords were used: [“Bruxism” OR “Teeth Grinding” OR “Teeth Clenching”] AND [“child” OR “children” OR “childhood” OR “kids” OR/AND “adolescents” OR “teenager”] AND [“therapy” OR “therapeutics”] AND [“laser” OR “laser biomodulation” OR “laser photo biomodulation” OR “splints” OR “occlusal splints”].
The search results were screened by reviewing the titles and/or abstracts to identify studies that met the inclusion and exclusion criteria. This process was conducted independently by 2 reviewers, and the results were then matched.
Eligibility criteria
The review included randomized controlled trials and clinical trials published in English that investigated the treatment of bruxism in children and adolescents (≤18 years of age) using low-level laser therapy (PBMT) and/or occlusal splints.
Studies involving participants older than 18 years, as well as case reports, study protocols and reviews were excluded from consideration.
Quality assessment
The quality of the included studies was assessed using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) guidelines. Furthermore, the risk of bias was evaluated using the Cochrane risk-of-bias tool.33
Results
A total of 67 English-language articles were identified through searches of MEDLINE (PubMed®), Google Scholar and the Cochrane Library. After applying the inclusion and exclusion criteria, 6 studies were included in the final analysis (Figure 1, Table 1).
Results of studies evaluating the effectiveness of occlusal splints
Four studies evaluated the effectiveness of occlusal splints alone in the treatment of bruxism. Three studies included children with mixed dentition,35, 36, 37 while 1 study included children with primary dentition.27 All 4 studies used rigid splints for treatment. Kolcakoglu et al. compared soft and rigid splints and found no significant differences between the 2 types in terms of masseter muscle activity.36
Restrepo et al. randomly assigned children with bruxism into 2 groups: an experimental group treated with rigid splints; and a control group.27 Although rigid splints were used for an extended period (up to 2 years, for at least 14 h per day), no significant differences were observed between the 2 groups when evaluating anxiety, TMD or dental wear.
The study by Bortoletto et al. suggested that bruxism may negatively affect craniocervical posture, and that a rigid occlusal splint (biteplate) may help reduce these negative effects, but only when the appliance is in place.37
In a pilot study by Giannasi et al., improvements in the bruxism-related symptoms, such as the absence of grinding sounds, decreased snoring (requiring further investigation) and fewer headaches, were observed after 90 days of nocturnal use of rigid splints.35 The study involved 9 participants and had a short follow-up period.35
Results of studies comparing occlusal splint therapy and photobiomodulation therapy
Two randomized clinical trials evaluating PBMT were included.31, 34 Both studies compared PBMT with occlusal splint therapy (OST).
Salgueiro et al. compared 4 different approaches and evaluated 2 variables, namely bite force, measured using a digital dynamometer, and salivary cortisol levels, assessed using enzyme-linked immunosorbent assay (ELISA) (Table 2).34
Kobayashi et al. compared 3 approaches and evaluated muscle activity using electromyography (EMG), as well as salivary dopamine levels measured by ELISA (Table 3).31 The masseter, anterior temporalis and upper trapezius muscles were assessed using EMG.31
Diagnosis of bruxism
All studies included in this review diagnosed bruxism based on parental or guardian reports of tooth grinding or clenching, combined with clinical signs such as tooth wear. In the study by Restrepo et al., parents or guardians were instructed to sleep next to their children for at least 2 weeks, and bruxism was diagnosed if tooth grinding or clenching occurred on at least 5 nights during this period.27 Additionally, the presence of bite marks on the buccal mucosa was included as part of the diagnostic criteria.34 Kobayashi et al. reported additional clinical signs, including dental marks on the tongue, the linea alba on the buccal mucosa, mandibular and/or maxillary tori, gingival recession, and fractures or cracks in the teeth.31
Inclusion and exclusion criteria across studies
The majority of the evaluated studies applied similar inclusion criteria, such as a confirmed diagnosis of bruxism, healthy pediatric participants, class I molar and canine relationships according to Angle’s classification, no prior treatment for bruxism, and the ability to cooperate during study procedures.
Additionally, the criteria for exclusion encompassed the presence of dental caries, physical or psychiatric conditions, malocclusions, and the use of medications such as antidepressants, analgesics, anti-inflammatory drugs, and muscle relaxants. Kolcakoglu et al. also excluded patients with intestinal parasites,36 while Restrepo et al. excluded participants with skeletal malocclusions confirmed by cephalometric radiographs.37
Discussion
According to the International Classification of Sleep Disorders (ICSD), the minimum criteria for diagnosing bruxism include parental reports of tooth grinding or clenching during sleep.38 Consequently, such reports are considered a reliable diagnostic method. Although polysomnography is regarded as the most reliable diagnostic tool, with an accuracy of 83.3% for nocturnal bruxism,39, 40 it is also considered the gold standard for diagnosing SB in adults.2 However, its use is limited by high cost, reduced practicality in pediatric populations, and its potential impact on sleep quality.41 Additionally, there is no standardized protocol for polysomnography in children.42 Kolcakoglu et al. introduced the BiteStrip® device as an alternative method for measuring muscle activity before and after treatment, demonstrating its usefulness in both diagnosis and evaluation.36
The adverse effects of bruxism are not limited to the stomatognathic system but may also involve the postural system and muscles of the craniofacial–neck–shoulder complex.43, 44 Therefore, early diagnosis is essential to prevent further complications. The ICSD states that 85–90% of the general population experience tooth grinding to varying degrees at some point in their lives; however, only 5% develop a clinically significant condition.45
In general, occlusal splints were ineffective in managing all signs and symptoms of bruxism, although some benefits were observed, such as reductions in pain, headache and deviations during mouth opening.27, 36 Prolonged use of splints did not appear to increase their effectiveness. Importantly, careful monitoring and follow-up are required when using occlusal splints in children due to ongoing growth, development and tooth eruption.
The only study reporting significant improvement in bruxism symptoms with occlusal splints was a pilot study with a small sample size of 9 participants.35 In some cases, occlusal splints produced immediate effects that persisted only when the appliance was worn and disappeared upon removal.37 This may be explained by the increase in vertical dimension during splint use, which promotes muscle relaxation and contributes to a more stable and functional joint position. Consequently, occlusal splints may help protect teeth, improve the function of the temporomandibular joint, and reduce abnormal muscle activity.43, 46
All included studies used conventional methods for manufacturing occlusal splints, involving traditional impressions and acrylic materials. Recent studies have introduced 3D-printed materials, including rigid and flexible resins with favorable mechanical properties and resistance.47, 48 Although they may offer advantages over traditional materials, further research is needed to confirm their clinical effectiveness.
In the present review, all studies investigating PBMT compared it with OST, as OST remains the gold standard and most widely used treatment approach. A major limitation of occlusal splints is the need for consistent cooperation from both children and their parents or guardians to ensure proper use.
Bruxism, as a repetitive motor activity, causes muscle contractions that can be measured by bite force. Bite force indicates the magnitude of masticatory muscle strength; a reduction in bite force following treatment may indicate muscle relaxation and diminished damage to anatomical structures.34 Low-level laser therapy demonstrated effectiveness in reducing bite force and showed superiority over occlusal splints in this parameter.34
Salivary cortisol levels were included as a variable to evaluate the effectiveness of bruxism treatment.49 Cortisol levels have been employed to assess stress-related responses in individuals with muscle disorders.50 An increase in salivary cortisol reflects an acute response to a stressor. However, the included studies found PBMT to be ineffective in reducing salivary cortisol levels. Therefore, Salgueiro et al. proposed that future studies should analyze hair cortisol instead of salivary cortisol, as salivary cortisol indicates acute responses to stressors, whereas hair cortisol is indicative of cumulative exposure to stress.34
Kobayashi et al. introduced salivary dopamine levels as a parameter for evaluating treatment effectiveness.31 Although their findings showed unfavorable and unexpected results when using occlusal splints, which manifested as an increase in the activity of the right and left temporal muscles and the left masseter muscles at rest after interference, the study did not clearly demonstrate whether PBMT had produced beneficial outcomes in SB treatment.31
Dopamine is a key neurotransmitter mediated by the central nervous system.51 An association has been identified between dopamine levels and neuromuscular disorders, including Parkinson’s disease, where a decrease in the concentration of dopamine was detected.52 Furthermore, dopamine can be analyzed from saliva swab samples, and an increase in its concentration has been observed in individuals with bruxism compared to controls.10, 31
Photobiomodulation therapy is considered a promising treatment method due to its ability to stimulate or inhibit cellular processes.53 It is particularly suitable for pediatric patients, as it is a painless, non-invasive and cost-effecitve procedure with a brief exposure time.49
Cerón et al. found that medications such as clonazepam and clonidine showed efficacy in reducing SB23; however, their use is limited by potential adverse effects. Similarly, treatments such as botulinum toxin and biofeedback have not demonstrated short-term efficacy and require longer follow-up periods.23
The findings of this review are consistent with previous literature indicating that no treatment provides a permanent solution for bruxism.54 Therefore, management strategies primarily focus on symptom reduction, protection of dental structures, pain relief, and improvement of sleep quality.18, 55
Due to the limited number of studies investigating PBMT in pediatric populations, no definitive conclusions can be drawn. Further studies are required to evaluate the effectiveness of PBMT in the treatment of bruxism among children. Additionally, restricting this review to English-language publications constitutes a limitation.
Conclusions
The adverse effects of bruxism are not limited to the stomatognathic system but extend to the postural system and the muscles of the craniofacial–neck–shoulder complex. Therefore, early diagnosis is essential to prevent further complications.
Based on the results of the analyzed studies, occlusal splints are not effective in managing all signs and symptoms of bruxism. However, they demonstrate some benefits, particularly in reducing pain, headaches and deviations during mouth opening.
There is a limited number of studies investigating the use of PBMT in the treatment of bruxism in children, which precludes definitive conclusions. Further research is needed to evaluate its clinical effectiveness in this population.
Ethics approval and consent to participate
Not applicable.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.