Abstract
Background. According to the World Health Organization (WHO), malocclusion is the most common oral disease in children after dental caries. Disorders pertaining to smile aesthetics and appearance can cause psychosocial problems and feelings of marginalization in children.
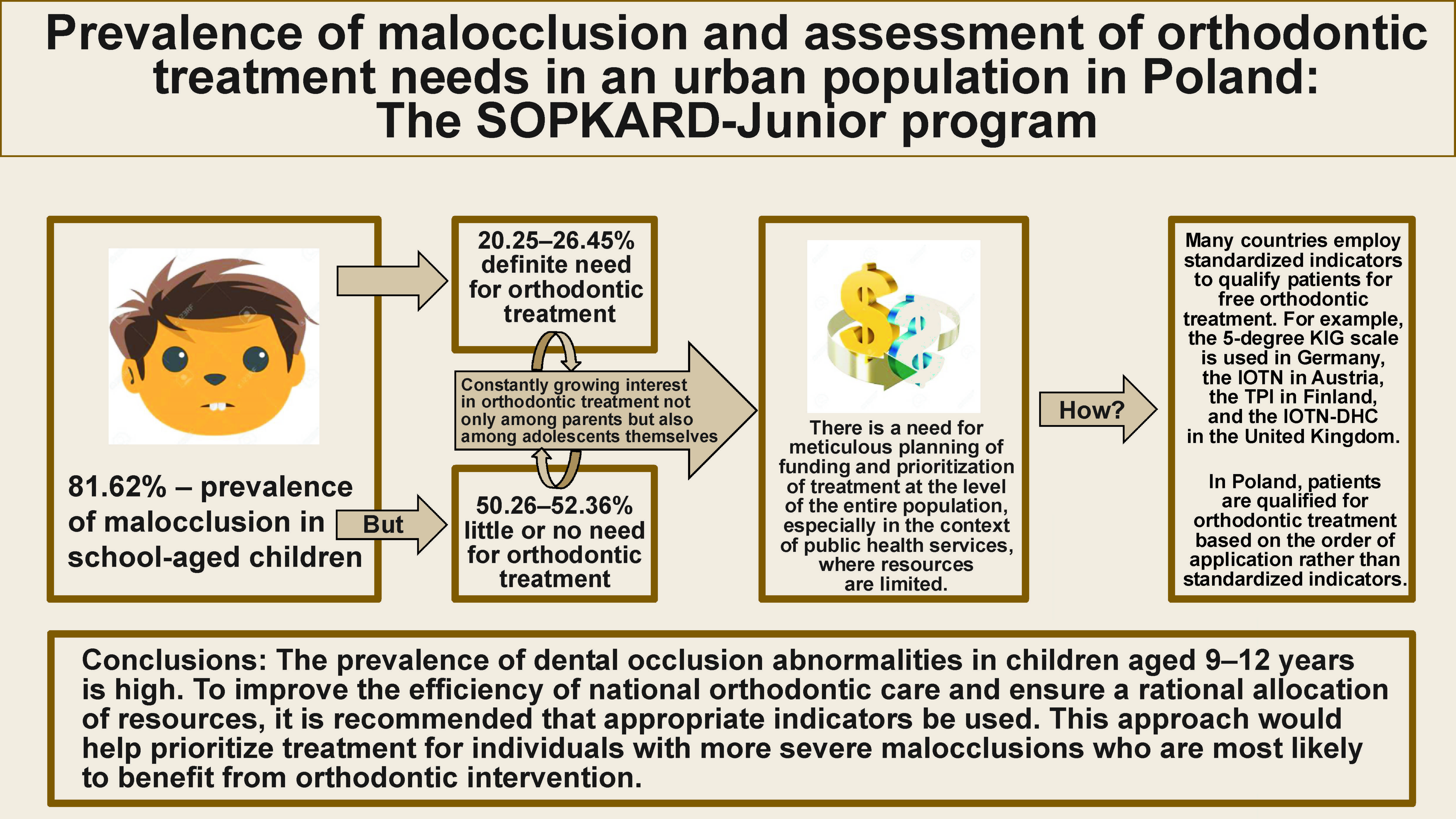
Objectives. The aim of the study was to assess the prevalence of malocclusion and to compare the need for orthodontic treatment in children treated with removable appliances and those who are not treated orthodontically.
Material and methods. The study sample consisted of 653 children aged 9–12 years (349 boys and 304 girls) from a selected urban population in Poland. The clinical study was based on the evaluation of Angle’s classification and analysis of other occlusal characteristics (overjet, overbite, crossbite, scissor bite, crowding, diastema, and midline shift). The assessment of orthodontic treatment needs was carried out according to the Dental Health Component of the Index of Orthodontic Treatment Need (IOTN-DHC).
Results. In the sample group, 533 children (81.62%) were diagnosed with malocclusion. The most frequent diagnoses were class I malocclusions (43.80%) and class II malocclusions (35.99%), as well as crowding (37.98%). Among the children studied, 28.95% were receiving orthodontic treatment and using removable appliances. As many as half (50.26%) of the children treated with removable appliances exhibited no or minimal need for orthodontic treatment. The study revealed no significant association between the severity of patient’s need for treatment and the probability of receiving orthodontic treatment with removable appliances.
Conclusions. The prevalence of malocclusion in the studied population is high. However, not all children with a diagnosed malocclusion require orthodontic treatment. For an effective plan of orthodontic care and rational budgeting, it is recommended that appropriate indicators be used to identify individuals with the most severe malocclusions who are eligible for treatment.
Keywords: children, prevalence, Index of Orthodontic Treatment Need, malocclusion
Introduction
The results of epidemiological studies that assessed oral health in children across different age groups show that the 3 predominant conditions of the masticatory organ in children and adolescents are dental caries, malocclusion and periodontal diseases.1, 2, 3 Due to its high prevalence, malocclusion is an important public health problem. For many individuals, malocclusion constitutes a major aesthetic issue that affects their quality of life. The orofacial region is an area of particular concern for the patient, as it attracts the most attention during interpersonal interactions and reflects the emotional state of an individual. Misaligned teeth can cause psychosocial problems related to appearance and result in marginalization or social exclusion.4 Some malocclusions can also have a negative impact on dental and facial development, contributing to impaired oral functions (e.g., chewing, breathing, speech, swallowing). According to some authors, malocclusions increase susceptibility to dental trauma and the development of caries, and can cause periodontal problems.5, 6
Organizing orthodontic care requires up-to-date information on the prevalence of different types of malocclusion and the need for orthodontic treatment. The data is important for the planning and subsequent implementation of preventive and therapeutic orthodontic interventions, especially in children at an early school age. On the other hand, most countries observe a constantly growing interest in orthodontic treatment not only among parents but also among adolescents themselves. This underscores the need for meticulous planning of funding and prioritization of treatment at the level of the entire population, especially in the context of public health services, where resources are limited.7
In Poland, reimbursement for orthodontic treatment is available for children up to the age of 12, therefore, the interest remains high. Insurance coverage is limited to treatment involving removable appliances. No indicators are used when qualifying a patient for treatment, and the application order is followed instead. Taking into consideration limited financial resources, it seems reasonable to determine whether the lack of objective guidelines, particularly in the qualification of patients for reimbursable orthodontic treatment, is appropriate.
Hence, the purpose of this study was to evaluate the prevalence of malocclusion and the existing system for qualifying patients for treatment by comparing the actual needs for orthodontic treatment in children treated with removable appliances with those who were not treated orthodontically. The analyzed data can be then used to formulate policies for healthcare systems.
Material and methods
The study was carried out within the framework of the SOPKARD-Junior program for early detection of risk factors of civilization diseases. The study received the approval from the Bioethics Committee for Scientific Research (approval No. NKBB/510-386, 395/2015). The SOPKARD-Junior is a preventive program, the main purpose of which is to assess the health status and health behavior of children and adolescents. The program welcomed all fifth-grade students from public elementary schools in Sopot, Poland. The study began after written consent had been received from children’s parents or legal guardians. Information on orthodontic treatment was obtained from a questionnaire completed by the parents.
A total of 720 children were examined, but the sample group included 653 individuals, as children treated with fixed appliances and those whose parents did not complete the questionnaire regarding past orthodontic treatment were excluded.
The clinical examinations of subjects were conducted in schools, specifically in quiet classrooms without external interference, under natural or artificial illumination. The assessment of dental occlusion was carried out using latex gloves, dental mouth mirrors and millimetric rulers. The analysis did not incorporate radiographs or study casts.
The evaluation of the occlusal conditions was carried out during 1 appointment by a single dentist with 14 years of clinical experience, specializing in orthodontics.
Orthodontic variables
Molar relationship
Angle’s classification was used to determine the relationship of the dental arches in the anteroposterior plane. The evaluation was based on the mutual relationship of first permanent upper and lower molars. Patients with different Angle’s classification on both sides of the dental arch were assigned to class II or class III malocclusions based on the predominant occlusal features and/or the mutual relationship of canines.8, 9, 10
Overjet and overbite
Overjet was classified as normal (0–4 mm), increased (>4 mm) or reverse (<0 mm). Similarly, overbite was defined as normal (0–4 mm), increased (>4 mm) or negative (<0 mm).8, 9, 10
Lateral crossbite and scissor bite
The analysis of the relationship of the dental arches in the transverse plane included an assessment of occlusion in the lateral segments. Lateral crossbite or scissor bite was diagnosed if it involved at least 1 tooth in the lateral segment of the arches.2, 8, 9
Midline shift
In the transverse plane, the symmetry of the dental arches in close contact was assessed based on the congruence or lack of congruence of the medial line of the upper and lower dental arches. An offset of the medial line of more than 2 mm was defined as a lack of congruence.8, 9, 11
Crowding and diastema
The presence of a diastema was determined when the distance between maxillary central incisors was more than 2 mm.8, 9
The deficiency of space in the arch was evaluated using the index of irregularity and crowding.12
Orthodontic treatment need
The need for orthodontic treatment was clinically assessed according to the Dental Health Component of the Index of Orthodontic Treatment Need (IOTN-DHC) (Table 1).13
Statistical analysis
All statistical calculations were carried out using the data analysis software system (Statistica, v. 13.; TIBCO Software Inc., Palo Alto, USA) and a Microsoft Excel spreadsheet (Microsoft Corp., Redmond, USA).
Quantitative variables were characterized by arithmetic mean (M) and standard deviation (SD). Qualitative type variables, on the other hand, were presented as means of counts and percentage values.
The Shapiro–Wilk test was used to test whether a quantitative variable came from a population with a normal distribution.
The statistical significance of the observed differences between the 2 groups was tested with Student’s t-test. In instances where the conditions for the application of Student’s t-test were not met or for variables measured on an ordinal scale, the Mann–Whitney U test was used.
Qualitative variables were analyzed with the use of the χ2 test of independence, and the Yates’ correction was applied for cell counts of less than 10. The Cochran’s conditions were determined and Fisher’s exact test was conducted.
In order to determine the association, strength and direction between variables, an analysis of correlation was applied by calculating Pearson’s and/or Spearman’s correlation coefficients. In all calculations, a p-value of 0.05 was considered statistically significant.
Results
The sample group consisted of 653 children aged 9–12 years, including 349 boys (53.45%) and 304 girls (46.55%). The mean age of the participants was 10.39 ±0.59 years, which was similar in both sexes. It was observed that 464 (71.06%) subjects did not receive orthodontic treatment, while 189 (28.94%) individuals were treated with removable appliances. The statistical analysis confirmed that girls were significantly more likely to undergo orthodontic treatment than boys (p = 0.024) (Table 2).
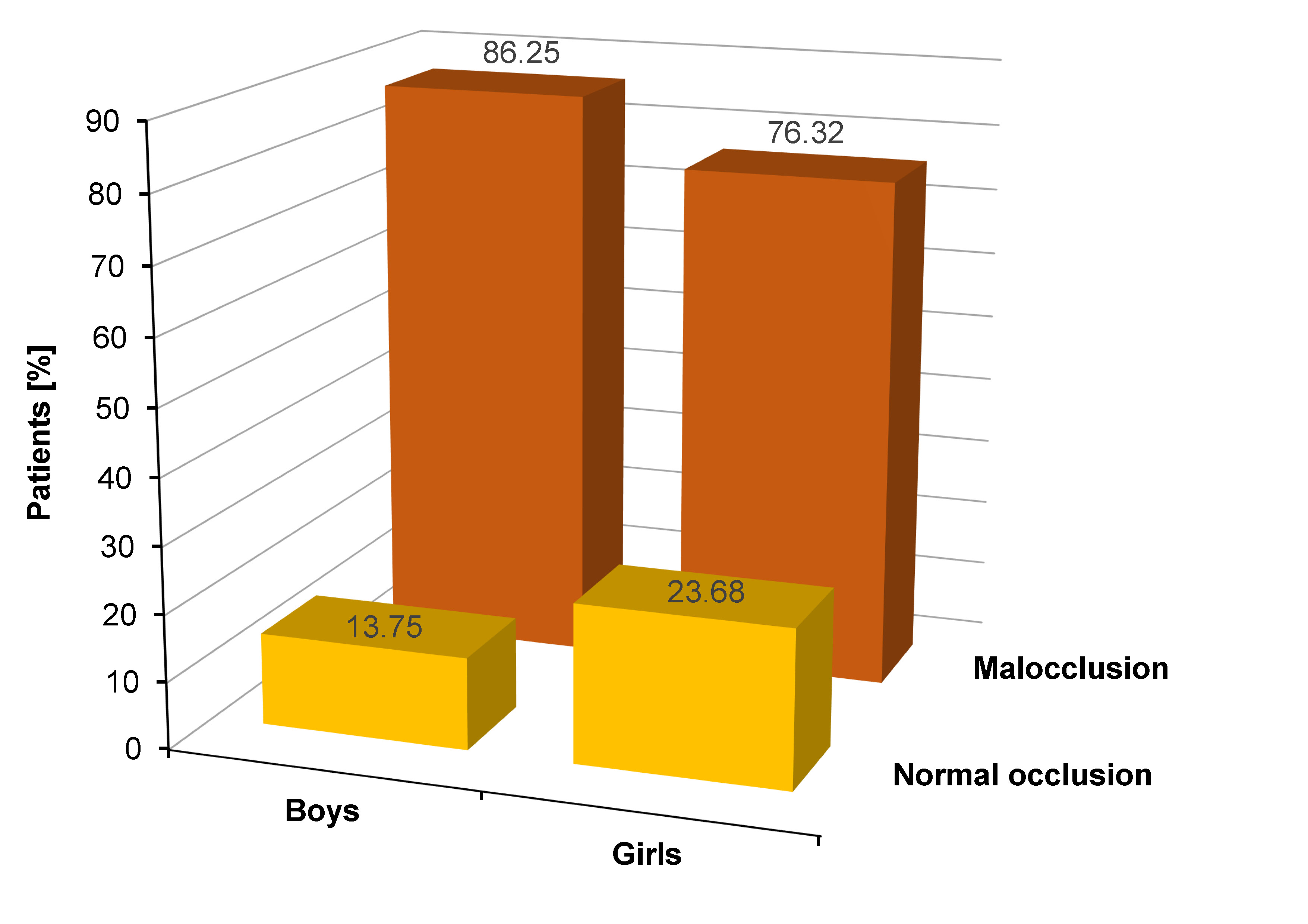
In the study sample, normal occlusion was present in 18.38% of the children, while abnormalities were identified in 81.62% of the subjects. Normal occlusion was more prevalent in females (23.68%) than males (13.75%) (Figure 1).
According to Angle’s classification, class I malocclusions were found in 43.80% of the subjects, with a significantly higher prevalence in males (p = 0.038). Class II malocclusions were identified at a comparable rate in both girls (35.19%) and boys (36.67%), whereas class III malocclusions were diagnosed in 1.88% of the subjects (Table 3).
In the study sample, an overjet within normal limits was found in 85.76% of the subjects. It occurred significantly more often in the group of girls (88.82%) (p = 0.037). In the female sample, a reverse overjet was not observed, whereas it was present in 2 boys (0.58%). An increased overjet was diagnosed more often in male participants, but the difference was not statistically significant (p = 0.058) (Table 3).
An overbite within normal limits was present in 86.68% of the subjects. It was observed more frequently in female participants (p = 0.002). A negative overbite was diagnosed very rarely, affecting only 2 children. In addition, increased overbite was significantly more frequent in the male subjects (p = 0.002) (Table 3).
In the sample group, the occurrence of deepened overbite was evaluated in defects of class I malocclusions (8.87%) and class II malocclusions (20.85%). The results of the study proved that excessive overlapping of the upper teeth over the lower teeth more often coincides with class II defects according to Angle’s classification.
Lateral crossbite was observed in 8.73% of the subjects, and scissor bite was diagnosed in 3.06% of the children. A midline shift (>2 mm) was found in 2.58% of boys and 6.58% of girls (Table 3).
Crowding of varying degrees of severity was present in 37.98% of the subjects, whereas it was absent in 37.83% of the children. In the remaining participants, the index was not applied due to the lack of erupted permanent canines or incisors. Correct tooth alignment was more frequently observed in female subjects (44.08%; p = 0.002) (Table 4).
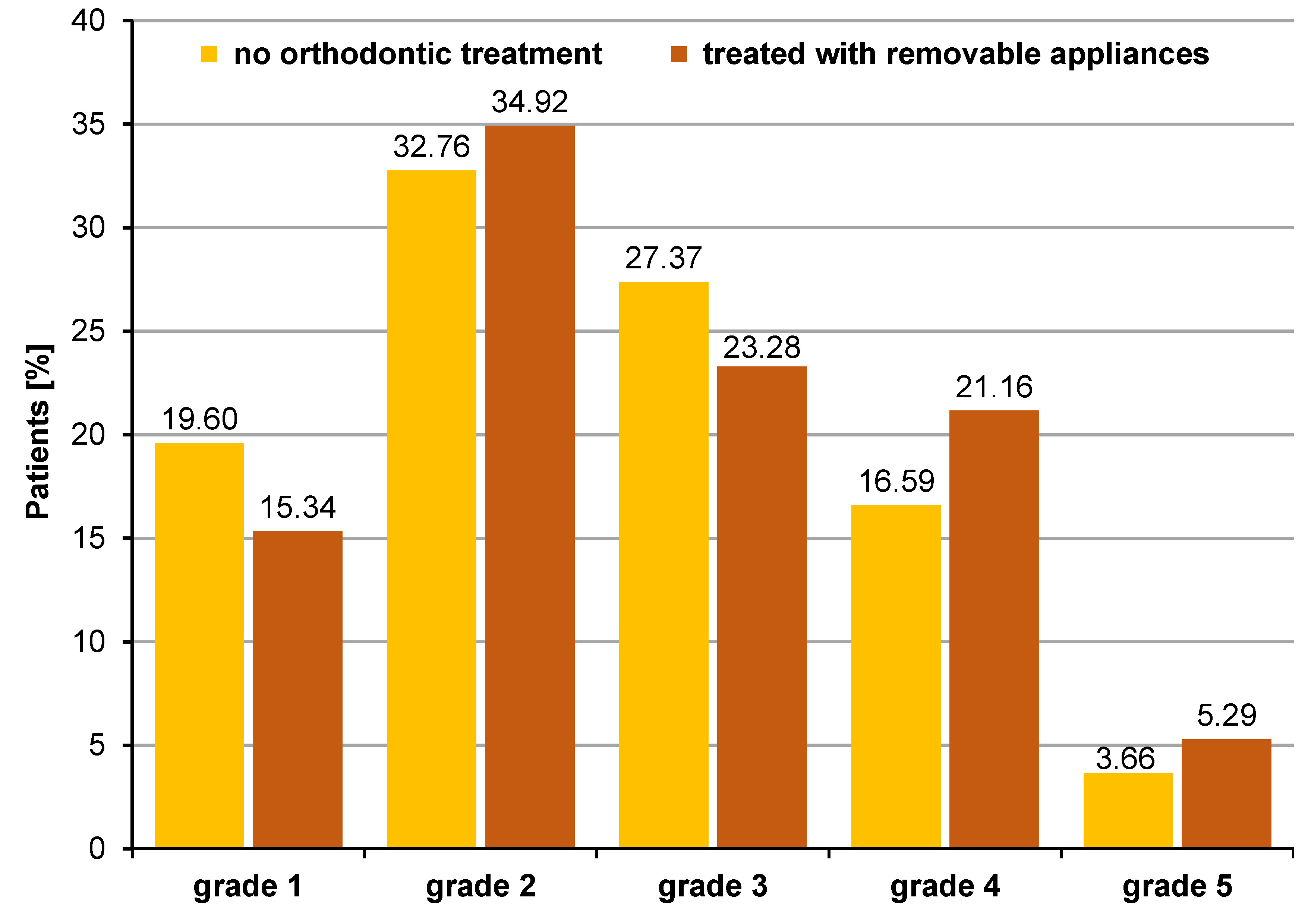
Among patients who did not undergo orthodontic treatment, 52.36% of respondents exhibited no or minimal need for treatment (grades 1–2). Meanwhile, 27.37% of the children demonstrated borderline need (grade 3), and 20.25% of students exhibited definite need for treatment (grades 4–5). In the group of patients treated orthodontically with removable appliances, no or minimal need for orthodontic treatment was noted in 50.26% of the subjects. A borderline need for treatment was identified in 23.28% of the children, while a definite need for treatment was found in 26.45% of the study sample (Figure 2).
The statistical analysis did not confirm that patients with severe and extreme need for treatment are more likely to receive orthodontic treatment (p = 0.083).
Discussion
In Poland, the prevalence of malocclusion has been analyzed in many studies, but there are few works assessing the actual need for treatment in children. The present study demonstrated a high prevalence of malocclusion in the study population, amounting to 81.62%. A similar percentage of individuals with bite abnormalities was reported in many countries.4, 14 A higher prevalence of malocclusion (84.6–95.6%) was found in Colombia, Libya and Lithuania,7, 15, 16 whereas a lower prevalence of malocclusion (56–71%) in school-aged children was reported in Brazil, Sweden, Slovenia, and Tanzania.1, 17, 18, 19
Class I malocclusion (43.80%) was most commonly reported in the sample group. A comparison of the results of studies conducted globally yielded a similar value, as evidenced by a study from Bosnia and Herzegovina.20 On the other hand, a higher prevalence of this abnormality, ranging from 61.4% to 72.5%, was observed in Italy, Romania, Iraq, and Morocco.8, 9, 21, 22, 23 Additionally, some studies have reported a lower prevalence of class I malocclusion compared to that noted in the present study.10
In the analyzed study sample, class II malocclusion occurred in 35.99% of the subjects. A similar prevalence was documented in Italy.9 The defects manifested at a higher frequency in Turkey.10 Lower values, ranging from 9.35% to 25.40%, were reported in several countries.7, 15, 21, 24
The prevalence of class III malocclusion in the sample group was the lowest, amounting to 1.88%. These abnormalities, among all malocclusions based on Angle’s classification, are the least frequently diagnosed in most studies in Poland and around the world. Exceptionally different results were obtained in Mexico, where class III defects were detected in 39.09% of subjects, and they were more common than class I defects.5
In the present study, an increased overjet was found in 13.96% of the study subjects. These results are low when compared to those obtained by foreign authors. Some studies noted a similar number of children with an increased overjet,9 but the values are higher in the majority of works.4, 7, 8, 25, 26 The differences in the obtained results may be due, among other factors, to the use of different normative ranges for defining normal, increased and reverse overjet. Many studies consider a measurement range of 0–4 mm as normal,8, 9, 10, 18 a finding that aligns with the methodology employed in the present study. The upper limit of the norm adopted by other authors is 3 mm,4, 14, 22 3.5 mm15, 16 or 2–3 mm.23
Based on the present study, a reverse overjet was found in 0.31% of the subjects. Having analyzed the results of studies around the world, the value seems rather low. A similar or higher number of children with a reverse overjet was reported in many countries.8, 9, 25 No study, however, found these values to be lower.
In the present study, an increased overlap of upper incisors on lower incisors was present in 13.02% of the subjects. Many factors affect the degree of vertical overbite. One of them is the inclination or tilting of the incisors, with the condition of the dentition playing an important role in this process. In groups with a high prevalence of caries in deciduous and permanent teeth, the incidence of increased overlap is higher. Differences may also be attributable to varying criteria for defining normal, increased and reverse overbite: 0–4 mm8, 9, 10; 0–3 mm14, 16; and 1–2 mm, respectively.23 In some works, an increased overbite is diagnosed when the upper incisors cover more than ⅔ of the surface of the lower incisors.27
Among the school-aged children, an increased overbite was more frequently associated with class II malocclusion, and this condition was more common among boys. Thilander et al. and Lux et al. obtained similar findings.7, 28 A higher prevalence of this abnormality was also observed in studies conducted in Colombia, Turkey, Germany, and France.7, 10, 25, 28 Sexual dimorphism may be related to differences in skeletal maturity and/or eruption of permanent teeth.28 In the sample group, a negative overbite was found in 0.31% of the subjects. A similar percentage of this abnormality was documented in Italy (0.70%).8 A higher prevalence (2.03–16.50%) was reported in numerous countries worldwide, predominantly those outside of Europe.7, 14, 23 Studies have also been conducted in which no cases of open bite were reported.29 The reason for this may be that the sample size was too small, thereby complicating the detection of less prevalent malocclusions.
A crossbite in lateral sections was present in 8.73% of the examined school-aged children. The global prevalence of this defect ranges from 5.4% to 15.2%.8, 23, 28, 29 In the present study, no significant differences were found in the incidence of crossbite, whether unilateral or bilateral. Although, studies conducted among children from Iraq reported a higher prevalence of this abnormality when present bilaterally.23 Considering that the majority of the study participants were aged 10–11 years, the percentage of students with lateral crossbite may appear high. It is important to note that this disorder requires early orthodontic intervention. Many studies have identified crossbite as a crucial aspect of dental health that necessitates intervention from early childhood.30
A relatively rare disorder found in the transverse plane is scissor bite. In the present study, it was found in 3.06% of children. The condition is diagnosed with equal rarity worldwide.7
Tooth crowding is most often the result of a quantitative discrepancy between the clinical length of the dental arch and the sum of the mesial and distal widths of the teeth. Crowding was the second most prevalent (37.98%) abnormality identified in the sample group. A number of studies have documented extremely high percentages of subjects with crowding. However, these studies predominantly entailed the analysis of the amount of space on models, potentially enhancing the study’s precision.31 In the sample group, no statistically significant correlation was identified between the incidence of arch space deficiency and sex, contrary to the study by Thilander et al., who noted a higher prevalence of the condition in female subjects.7
Among the surveyed children from elementary schools in Sopot, 28.95% of boys and girls were treated with removable appliances. Compared to other European countries, this percentage is high. In the UK, the prevalence was 8% among 12-year-old children and 14% among adolescents aged 15–16.32 In France, only 2.4% of children use braces, and in Latvia, 18% of boys and girls undergo orthodontic treatment.25, 33 There may be various reasons for these discrepancies, including the increasing interest in orthodontic treatment and the fact that in Poland, only removable appliances are reimbursed by the Polish National Health Fund (NFZ) for children up to the age of 12. The results of the present research demonstrate that females undergo orthodontic treatment more frequently. This finding aligns with the results of many authors.32, 34 However, there are few works that show a greater interest in braces therapy among male subjects.35 The increased frequency of malocclusion correction needs among women may be indicative of societal stereotypes regarding gender roles, where societal norms place a higher value on physical attractiveness for women. Female patients are more likely to prioritize the aesthetic appeal of straight teeth compared to their male counterparts, which leads to a higher demand for orthodontic treatment among females. Girls and their parents are also more likely to accept long-term orthodontic treatment.36
As the demand for orthodontic treatment increases, there is a growing need for reliable information regarding the actual necessity of such treatment. The diagnosis of dental occlusion abnormalities does not invariably necessitate intervention, as defects of low severity are not always an indication to start therapy. Therefore, of those reporting a desire for orthodontic treatment, it would be advisable to select individuals with the greatest treatment need. The use of dedicated indicators is instrumental in facilitating such an assessment. These tools also help classify malocclusion and prioritize qualifying patients for reimbursable orthodontic treatment.37 One of the most commonly used indicators for assessing the need for orthodontic treatment in both children and adults is the IOTN-DHC, which was used in the present study.
The analysis showed that 23.35% of children require orthodontic treatment (grades 4 and 5). The percentage increased to 48.68% when students with grade 3 of the IOTN-DHC were also taken into account. The definite need for treatment (grades 4 and 5) is analogous to that reported in school-aged children in many countries.8, 25, 38, 39
In line with the findings of most of the studies on the subject, the present study revealed no statistically significant differences with regard to the need for orthodontic treatment in relation to sex.8, 21, 25, 38, 40 In contrast, a study conducted in Bosnia and Herzegovina identified a higher prevalence of treatment needs among female subjects.41 The sex disparity was also noted in studies undertaken in Brazil, where a greater need for orthodontic treatment was found among male individuals.42 In contrast, Baubiniene et al. stated that sex has an impact on the need for orthodontic treatment, but its influence changes with age.43
In the study population, the extreme need for treatment was found to be slightly higher among subjects treated with removable appliances compared to those who did not undergo orthodontic treatment. Although this result is expected, the statistical analysis did not confirm the significance of these differences. This finding emphasizes that children afflicted with the most severe malocclusions do not necessarily benefit from orthodontic treatment with removable braces, a treatment that is largely reimbursed in Poland.
In the group of patients treated with removable appliances, there was no or minimal need for orthodontic treatment in 50.26% of the subjects. A borderline need for treatment was found in 23.28% of the participants, while 26.45% of the children demonstrated a definite need for treatment. The absence of specific guidelines for qualifying patients for orthodontic treatment frequently results in the initiation of treatment that is not determined by the severity of malocclusion, but, for example, by the subjective assessment of the patient or the order in which the patient reports to the orthodontist. A rational solution to this situation is to establish more objective criteria for the qualification for orthodontic treatment, such as appropriate indicators.
Without objective assessment tools, judging the need for orthodontic treatment becomes subjective and unreliable. For this reason, many countries employ standardized indicators to qualify patients for free orthodontic treatment. For example, the 5-degree KIG scale is used in Germany, the IOTN in Austria, the Treatment Priority Index (TPI) in Finland, and the IOTN-DHC in the United Kingdom.29, 44, 45
The present study confirms the need for epidemiological orthodontic research, especially at this stage of occlusal development, as children represent an ideal population for planning and evaluation of the effectiveness of preventive and therapeutic programs, as well as for monitoring bite development.
Limitations
The study sample consisted of children who had not undergone orthodontic treatment or those treated with removable appliances. Children treated with fixed appliances were excluded from the study. Many researchers additionally exclude individuals with removable appliances,3, 25, 30, 38, 43 yet this is not a universal practice.46 According to some researchers, the exclusion of patients with any kind of appliances may create a misleading picture of the actual need for therapeutic treatment, as these individuals may still require orthodontic care.38, 47 Nevertheless, the severity of malocclusion in children treated with removable appliances may change over time, a tendency that is reflected in the study findings.
Conclusions
The prevalence of dental occlusion abnormalities in children aged 9–12 years is high, though not all cases require orthodontic treatment due to the low severity of malocclusions. The most common dental occlusion disorders are class I and class II defects, increased overjet and overbite, and dental crowding. Notably, up to half of the children currently treated with removable appliances show little or no need for such therapy. To improve the efficiency of national orthodontic care and ensure a rational allocation of resources, it is recommended that appropriate indicators be used. This approach would help prioritize treatment for individuals with more severe malocclusions who are most likely to benefit from orthodontic intervention.
Ethics approval and consent to participate
The study was approved by the Bioethics Committee for Scientific Research (approval No. NKBB/510-386, 395/2015).
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.