Abstract
Background. The preparation of model teeth for prosthetic crowns plays a crucial role in preclinical dental education. Its primary objective is to ensure optimal conditions for training students to function in clinical settings.
Objectives. The aim of the study was to assess the quality of dental students’ education regarding the preparation of model teeth for cast metal-ceramic crowns. An additional objective was to compare the agreement between measurements made by examiners on the model teeth prepared by the students.
Material and methods. A total of 180 model premolar teeth (KaVo) were used for the tests. The teeth were prepared by the third-year dental students, who created a shoulder finish line on the buccal surface and a chamfer finish line on the palatal surface. Two examiners assessed the convergence angles of walls, the margin width of surfaces, the reduction in the height of functional and non-functional cusps, the extent of the preparation, the smoothness of the preparation, and the continuity of the finish line using simple measuring tools.
Results. The students’ most proficient parameters were margin width, the extent of the preparation, and the finish line continuity. The least accurate results were observed in the wall convergence angles and the reduction in the height of functional and non-functional cusps. The interexaminer reliability was considerable for convergence angles, the margin width and the reduction in the height of cusps (intraclass correlation coefficient (ICC) >0.75). The examiners demonstrated moderate agreement (kappa: 0.60–0.79) for parameters such as the extent of the preparation, wall smoothness and finish line continuity.
Conclusions. The exercises provided a solid foundation for the students. However, practice and more targeted feedback are necessary to improve performance in the more challenging aspects of tooth preparation. The traditional analytical approach that uses simple measuring tools to assess the tooth preparation procedure is a reproducible method that examiners can use to effectively evaluate students’ work.
Keywords: dental students, evaluation, dental education, prosthodontic tooth preparation
Introduction
The quality of education in dentistry is contingent upon numerous factors, including a well-organized curriculum, effective teaching methods, modern educational tools, and appropriate academic support. A well-designed curriculum should cover a wide range of topics and be regularly updated. The efficacy of teaching methods and tools is paramount in ensuring that students can thoroughly master both theoretical and practical issues. Teachers play a crucial role in education, as their approach to delivering knowledge, assessing students and providing feedback significantly influences students’ skills. These elements contribute to the training of skilled dentists who can provide patients with a high standard of dental care. Prosthodontics is a field of dentistry that requires theoretical knowledge and high practical skills. Students initially develop their precision and manual skills through preclinical exercises, followed by clinical exercises.1, 2
Preparing simulated model teeth for prosthetic crowns plays a crucial role in preclinical dental education in the field of prosthodontics. Its primary objective is to ensure optimal conditions for training students to function in clinical settings. The preclinical training assumes the form of practical sessions that offer dental students the opportunity to engage with a novel learning environment. Besides providing theoretical knowledge, these classes are designed to develop the students’ manual skills and foster an understanding of “spatial vision”.2, 3 Initially, students are required to complete a series of theoretical sessions, encompassing seminars and lectures, that prepare them for practical exercises. Subsequently, they perform activities demonstrated to them beforehand on specially prepared simulated models, and only after successfully completing these sessions they can transition to working with actual patients. Preclinical sessions introduce students to deviations from the ideal (standard) preparation and encourage them to identify their shortcomings and to work on improvements. The evaluation of students’ performance at the preclinical stage is a pivotal aspect of education, as it serves to reinforce the learning process. It enables early error detection and guides students in their work. Furthermore, it provides teachers with insights into the specific work stages or parameters that pose the greatest challenges for students and require special attention or repetition. All these factors translate into easier, less stressful, and improved patient care.4, 5 There is a positive correlation between students’ grades in preclinical and clinical exams, indicating that appropriate preparation in the earlier stages of education can positively influence clinical competencies of students.6
The identification and implementation of effective methods for assessing students’ performance remains a significant challenge for academic teachers and educators.7, 8 There are noticeable differences in tooth preparation assessments, with discrepancies noted both between assessors and between the assessments made by the same examiner evaluating the same procedure at different times.9 The development of objective approaches to evaluating tooth preparation is a critical aspect of dental education. Current methods for the assessment of tooth preparation can be divided into traditional and digital techniques.4
The traditional approach is the most often adopted by examiners experienced in a specific field, who compare the work of students with a standard model. In traditional practice, researchers distinguish between a global assessment (inspection and evaluation) method and an analytical (using rubrics) method. The former is a straightforward visual technique in which the examiner provides a comprehensive grade for the student’s work. This subjective method rarely produces consistent results.10 According to some researchers, examiner fatigue is a particularly important factor contributing to inconsistencies between ratings.9 Conversely, the analytical method involves the creation of rubrics, based on textbooks and publications, to assess individual components of tooth preparation. Specific parameters are evaluated by measuring certain distances and angles using basic measuring tools such as a ruler, a compass and a protractor. The parameters that are frequently measured in this manner include the convergence angles between the walls, the width of the prepared margin, the reduction in the height of the occlusal surface, the extent of the prepared finish line, and the smoothness of the preparation.4 In this method, proper calibration of the assessors is vital. This process involves the formulation of the objective assessment criteria for the preparations, so that the latter are easy to measure, interpret and reproduce. This approach enhances accuracy and precision, thereby mitigating the risk of subjectivity and inconsistency in evaluations. For students engaged in the learning process, consistent, definite and repeatable feedback from educators regarding the quality of their work is of the utmost importance. Such feedback enables students to absorb knowledge in a specific field more rapidly and to focus on the learning process rather than on wondering whether the grade they have received is fair or accurate.8 Research suggests that the reliability of student assessments can be increased by employing 2 assessors, as opposed to the traditional method in which a single examiner is involved.8, 11 Without assessor calibration, there is a risk of diverging assessments made by different teachers.
In recent years, more advanced evaluation methods have been introduced, such as digital assessments of tooth preparations that employ various scanners and computer-aided design software. The efficacy of these methods is primarily attributable to their accuracy. They can also serve as an additional educational approach in preclinical sessions.12, 13 While digital technologies facilitate the acquisition of manual skills, there is no evidence regarding the long-term impact of digital training methods on clinical outcomes and student competencies.14 Despite the immediate feedback provided by these methods, studies have demonstrated that students prefer receiving feedback from a teacher during sessions and also benefit from digital methods. Similarly, during exams, they seek evaluation from both human examiners and computers. Students perceive digital methods as an objective source of feedback and a valuable addition to teaching practical skills. Yet, they do not want to entirely abandon traditional assessment methods in favor of newer technologies.15, 16 Sometimes, students achieve low or inconsistent results when first interacting with a digital assessment system.3 The implementation of these methods requires appropriate training, and due to their relatively high cost and the need for special maintenance, they remain unavailable in most academic centers for use in preclinical sessions. As a result, the primary educational approach continues to rely on the traditional method for assessing students’ readiness.15, 16
The aim of the study was to assess the quality of dental students’ education regarding the preparation of model teeth for cast metal-ceramic crowns. An additional objective was to compare the agreement between measurements made by examiners on the model teeth prepared by the students.
Material and methods
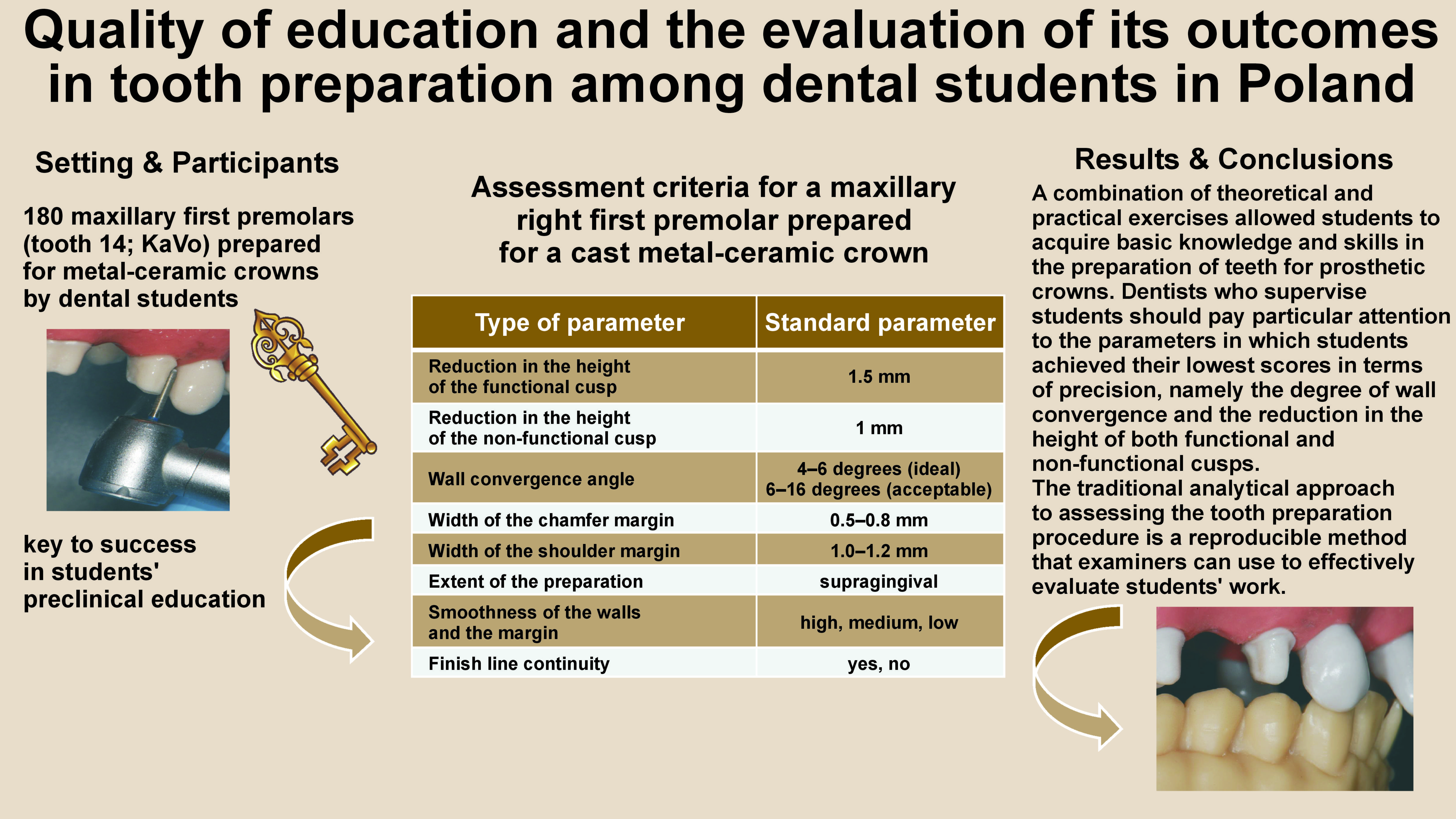
The present study was based on 180 models of maxillary right first premolars provided by KaVo (Biberach, Germany) and prepared by third-year dental students at the Jagiellonian University Medical College (Krakow, Poland). A total of 180 students, with an average age of 22 years, participated in the study. The study protocol followed the ethical guidelines established by the 1975 Declaration of Helsinki and was approved by the Institutional Ethics Committee at Jagiellonian University Medical College (approval No. 118.6120.109.2023). Prior to their involvement in the study, each student provided informed consent.
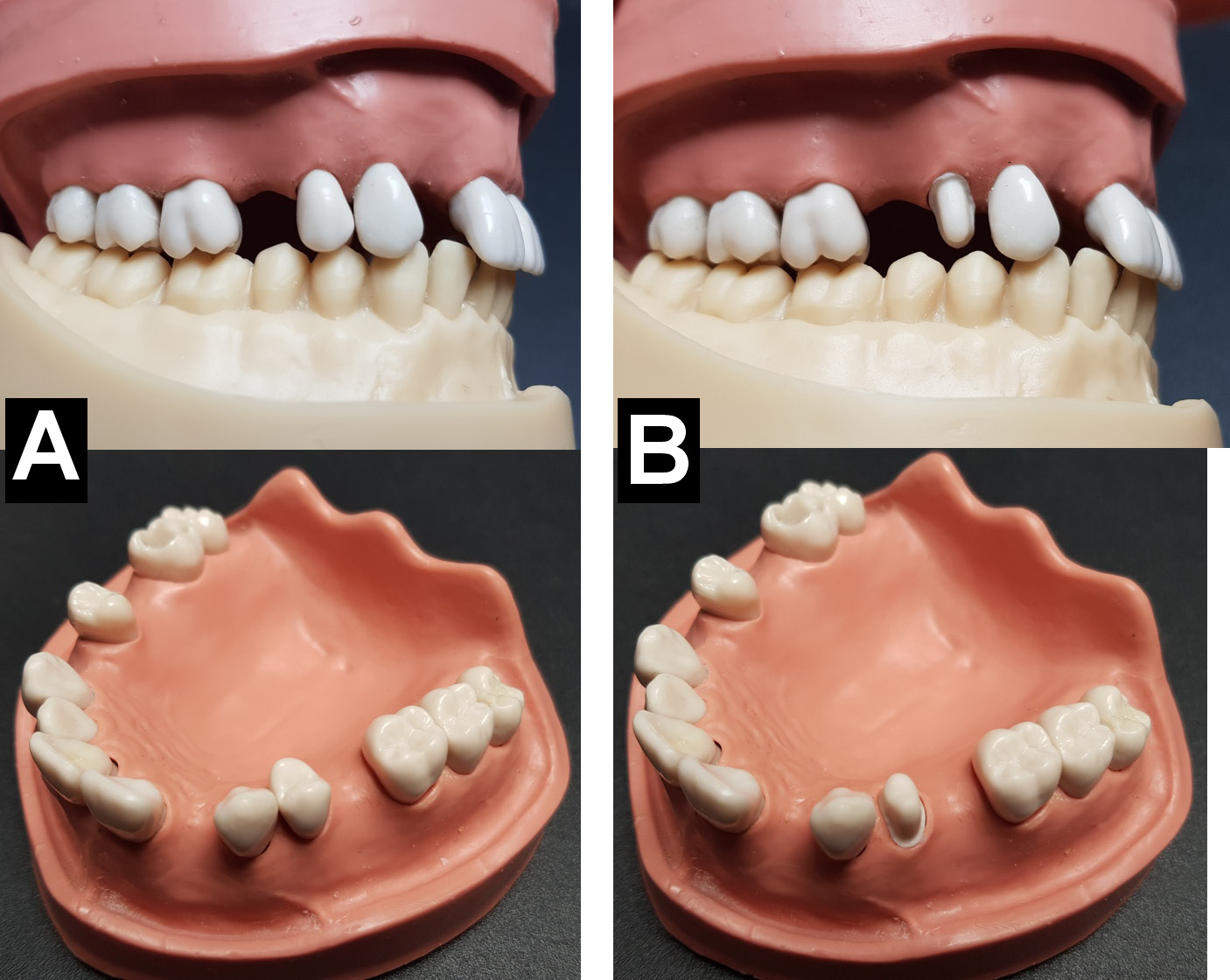
The preparation stage was preceded by a series of theoretical lessons, including lectures and seminars. The students attended a total of 3 h of lectures, which were delivered by a professor and included a range of subjects, such as the definition of prosthetic crowns, the various types of prosthetics crowns and the indications for their use. Additionally, the lectures covered the general principles of tooth preparation. The seminars were led by academic teachers and consisted of 2 sessions, each with a duration of 45 min. During these sessions, students were acquainted with the principles for properly preparing the maxillary right first premolar for a cast metal-ceramic crown (Table 1). The students received instructions verbally and in the form of an instructional video. The preparation process involved creating a shoulder margin on the buccal surface, a chamfer margin on the palatal surface, and a smooth transition between these finish lines on the proximal surfaces. Directly after the second seminar, the students began the practical exercises. The participants had 2 h and 30 min to perform the preparation. This task constituted the students’ first experience with a tooth preparation procedure. A specific bur set, designed by Prof. Stanisław W. Majewski and Prof. Bartłomiej W. Loster (Olident, Cologne, Germany) and intended for a crown with a step-type finish line preparation was used. To mimic the natural conditions of the oral cavity, the model teeth were mounted on partial dentition study models (OK T12; KaVo) and then on dental patient simulators (KaVo). The practical part was supervised by academic teachers. During the preparation phase, the students did not communicate with each other. Once the exercises were completed, the teeth were extracted from the study models, collected and numbered by the examiners. Figure 1 presents the premolar tooth 14 mounted on the partial dentition study model before and after preparation.
The authors adopted an analytical method for evaluating the prepared teeth, wherein each parameter was assessed individually. The measurements were made by 2 independent examiners (examiner A and examiner B) who were dental practitioners and academic teachers with over a decade of professional experience. The examiners familiarized themselves with the preparation assessment criteria (Table 1), and they were calibrated before proceeding with their evaluations. The calibration was performed on a model of an ideal preparation, indicating how deviations from the standard model should be assessed. After the calibration and before the evaluation, the examiners assessed a random sample of 15 prepared teeth to ensure the consistency of the evaluations and the comprehension of the assessment criteria. Each examiner independently evaluated 15 preparations, after which the results were analyzed and discussed collectively.
The authors assessed the convergence angles mesiodistally and buccopalatally, the width of the margin at the midpoint of the mesial (m), distal (d), buccal (b), and palatal (p) surfaces, the reduction in the height of functional and non-functional cusps, the extent of the preparation from the mesial, distal, buccal, and palatal sides, the smoothness of the preparation, and the continuity of the finish line. The convergence angles were measured using a white sheet of paper, a pencil (Faber-Castell Grip 2001 “H”; Faber Castell, Stein, Germany), a plastic ruler (Herlitz, Hanover, Germany), and a plastic protractor (Herlitz). The analysis involved placing and stabilizing the tooth on a piece of paper, marking 2 lines using a pencil and a ruler along the prepared tooth surfaces, and measuring the angle at which the lines intersected using a protractor. This procedure was repeated twice for each tooth – first for the mesiodistal angle and then for the buccopalatal angle after the tooth was flipped. The margin widths were measured at the midpoint of each surface with an analog calliper (Högert Technik GmbH, Pruszków, Poland) after which they were remeasured with a ruler.
The height of the cusp reduction was measured using a calliper, with the measurement extending from the cementoenamel junction to the highest point of each cusp. The actual value was then determined with a ruler [mm]. The remaining parameters were visually assessed by the examiners, according to the established criteria (Table 1). Each examiner had 3 min to complete a single tooth assessment. The examiners were instructed to perform this task independently, that is, without consulting one another.
Statistical analysis
The continuous variables were presented as medians and interquartile ranges, while the categorical variables were expressed as frequencies and percentages. The interexaminer reliability in the case of convergence angles, margin width and reduction height was assessed by means of the intraclass correlation coefficient (ICC). In the case of finish line continuity, Cohen’s kappa was used, while for the extent and smoothness of the preparation, the weighted kappa was the method of choice. The significance level was set at p < 0.05. The calculations were performed using the IBM SPSS Statistics for Windows software, v. 26.0 (IBM Corp., Armonk, USA).
Results
For examiners A and B, the mesiodistal (m-d) walls exhibited median convergence angles of 22.5 (IQR: 17–28) and 20.5 (IQR: 15–28) degrees (ICC = 0.821), and for the buccopalatal (b-p) walls, the angles were 23 (17–30) and 22 (16–29) degrees (ICC = 0.938), respectively. The differences in the margin width, as measured by examiners A and B, yielded the following medians: for the mesial margin – 0.50 (0.25–0.75) mm and 0.50 (0.25–0.50) mm, respectively (ICC = 0.774); for the distal margin – 0.75 (0.50–1.00) mm and 0.50 (0.25–1.00) mm, respectively (ICC = 0.866); for the buccal margin – 1.00 (0.75–1.00) mm and 1.00 (0.50–1.00) mm, respectively (ICC = 0.818); for the palatal margin – 1.00 (0.75–1.25) mm in the case of both examiners (ICC = 0.858). The median values for the functional cusp reduction height were 1 (IQR: 1–1.5) mm for examiner A and 1 (IQR: 1–2) mm for examiner B (ICC = 0.830). For the non-functional cusps, the medians were 2.0 (1.5–2.3) mm and 2.0 (1.5–2.5) mm, respectively (ICC = 0.893). With regard to the agreement between the doctors on the students’ measurements of the extent of the preparation, the values were as follows: mesial kappa = 0.694; distal kappa = 0.600; buccal kappa = 0.728; and palatal kappa = 0.616. The smoothness of the wall and finish line continuity yielded kappa values of 0.726 and 0.617, respectively.
There was considerable agreement between the examiners (ICC > 0.75) regarding aspects such as the m-d and b-p wall convergence angles, margin widths, and the reduction heights of both the functional and non-functional cusps. Moderate interexaminer reliability was observed for the extent of the preparation, wall smoothness, and finish line continuity, with the kappa values ranging from 0.600 to 0.728. The most significant discrepancy between the examiners’ measurements concerned the extent of the preparation on the distal side, while the b-p convergence angle exhibited the least variance (Table 2).
Table 2 presents the number of students who met the optimal benchmarks for individual preparation parameters, segmented by each evaluator’s assessment. According to examiner A, only 6 (3.3%) students achieved the optimal m-d wall convergence angle, whereas examiner B identified 4 (2.2%) such students. For the b-p angle, examiners A and B identified 6 (3.3%) and 8 (4.4%) students, respectively. In the case of the acceptable m-d wall convergence angle, they found 37 (20.7%) and 50 (27.8%) students meeting the criteria, respectively. The corresponding numbers for the b-p angle were 37 (20.7%) and 46 (25.6%). With regard to the ideal shoulder margin width, 89 (49.4%) students satisfied the criteria according to examiner A and 113 (62.8%) according to examiner B. The optimal chamfer margin width was achieved by 152 (84.4%) students for examiner A and 136 (75.6%) for examiner B. Only 25 (13.9%) students achieved the correct reduction height for functional cusps in examiner A’s assessment, while 39 (21.7%) did so according to examiner B. Examiner A reported that 26 (14.4%) students attained the correct reduction height for non-functional cusps, while examiner B noted this achievement in only 15 (8.3%) individuals. One area in which the students excelled was the extent of the preparation on specific tooth surfaces. According to examiners A and B, the supragingival preparation was accomplished by 85.6–96.1% and 75.0–93.3% of the students, respectively, and depended on the tooth surface. A majority of the students, namely 80 (44.4%) students in the case of examiner A and 89 (49.4%) according to examiner B, produced a preparation with average wall smoothness. According to examiners A and B, a high degree of surface smoothness was achieved by only 61 (33.9%) and 46 (25.6%) students, respectively. The majority of the students managed to maintain the finish line continuity of the maxillary right first premolar, e.g., 112 (62.2%) of the students evaluated by examiner A and 94 (52.2%) of those assessed by examiner B. The students’ most proficient parameters were the shoulder and chamfer margin widths, the extent of the preparation, and the finish line continuity. Conversely, the most challenging areas were the wall convergence angles and the reduction heights of both the functional and non-functional cusps.
Discussion
Preparing a tooth for prosthetic crowns is one of the most challenging manual procedures that students encounter during their dental training. In a study conducted by Hattar et al., the confidence levels of fifth-year students were evaluated by a questionnaire when performing various dental procedures.17 The students felt most competent and assured when performing direct restorations and endodontics, and least confident when dealing with fixed prosthodontics. In the context of fabricating indirect restorations, they exhibited a notable decrease in confidence during the preparation of tooth crowns when compared to taking impressions or trying in the prosthetic restoration.17 Appropriate training during preclinical sessions is of the utmost importance in enhancing student skills and bolstering their confidence in the field of fixed prosthodontics.
The present study identifies specific areas in dental education that require improvement to enhance students’ practical skills in tooth preparation for prosthetic crowns. It also highlights the importance of detailed and consistent assessments in education.
The students demonstrated the highest level of skills in achieving optimal margin widths on various surfaces, the extent of the preparation, and maintaining finish line continuity.
A high percentage of students met the criteria for optimal shoulder and chamfer margin widths. Specifically, from 49.4% (examiner A) to 62.8% (examiner B) of students achieved the ideal shoulder margin width, and from 75.6% (examiner B) to 84.4% (examiner A) achieved the optimal chamfer margin width. Maintaining finish line continuity was achieved by more than half of the students. This finding aligns with the conclusions of other authors. In a study by Sadid-Zadeh et al., 75% of the cases attained the desired width and continuity for the given crown type.18 Al-Omari and Al-Wahadni reported an average margin width of 0.86 mm buccally, 0.74 mm palatally, 0.7 mm mesially, and 0.66 mm distally.19 These values were lower than the recommended 1.0–1.2 mm for a shoulder-type margin. An excessively wide margin violates the biological principles of tooth preparation. Conversely, a margin that is too narrow may result in an aesthetically pleasing tooth restoration, especially when it comes to less translucent materials. The presence of a discontinuous finish line may compromise the marginal adaptation of the restorations.
One parameter in which students achieved good results was the location of the finish line relative to the gum line. In over 75% of the prepared specimens, the required supragingival margin was achieved. This adequate tooth preparation, which approaches the standard, is instrumental in maintaining proper hygiene and sealing prosthetic restorations. This finding is consistent with the research, wherein students also obtained favorable results for this parameter.4
Most students achieved an average level of smoothness of the prepared tooth stump surface. A lack of wall smoothness can reduce the fit of the prosthetic restoration. Smoothness is particularly important at the gingival level of the finish line, as its absence in this area can cause the prosthetic restorations to leak. In addition, the findings of other authors indicate that this is not an easy parameter to achieve.18 The required smoothness of the prepared stumps was achieved by less than half of the students.18
In the present study, the students were the least precise in their preparation of the convergence angles of the mesiodistal and buccopalatal walls, greatly exceeding the presumed margins of error (optimal values). The standard guidelines for wall convergence angles during the crown preparation procedure consider an angle within the range of 4–6 degrees as ideal, and 7–16 degrees as acceptable.20, 21 The more the opposing prepared walls lie parallel to one another, the greater the retention of the final prosthetic restoration. However, achieving these recommendations in clinical practice can present challenges as it requires a high level of precision and clear visibility in the operative field. Factors such as the position of the tooth within the dental arch, anatomical structure and the practitioner’s experience all play significant roles. Achieving almost parallel walls without the risk of undercuts in the tooth preparation is challenging. Excessive reduction of the tooth stump, resulting in an increased convergence angle, may compromise the retentive properties of the abutment.20, 22 Numerous researchers have noted overly high convergence angles among dental students practicing on model teeth. In a study by Ayad et al., no more than 47% of the teeth prepared by dental students had acceptable convergence angles.21 Al-Omari and Al-Wahadni examined 157 tooth samples prepared for metal-ceramic crowns, finding average convergence angles of 22.4 degrees and 25.3 degrees for buccopalatal and mesiodistal walls, respectively.19 Strain et al. analyzed articles from 11 countries, published between 1978 and 2014, encompassing a total of 2,306 preparations.23 In these studies, students failed to achieve wall convergence angles between 4 and 14 degrees. Most papers reported angles ranging from 10 to 20 degrees.23
Another challenging parameter in the study was the reduction in the height of both functional and non-functional cusps. Less than one-fourth of the students achieved correct results in these parameters. Excessive reduction of the occlusal surface may lead to poorer retention of the prosthetic restoration. Insufficient occlusal reduction necessitates thinner layers of restorative materials, which can potentially affect the crown’s resilience, longevity and aesthetics. Sadid-Zadeh et al. found optimal cusp reduction values difficult to achieve.18 Out of 223 teeth prepared by students in preclinical sessions, only 53.7% obtained optimal cusp reduction values.18 Al-Omari and Al-Wahadni reported occlusal surface reduction ranging from 1.8 mm to 2.2 mm, with an average reduction of 2 mm. These values are slightly above the ideal but nevertheless still ensure crown durability and good aesthetics.19
Achieving the correct convergence angle and cusp height reduction values is challenging for the majority of dental students and requires vigilant oversight from supervising clinicians. Students should prioritize refining their skills in areas in which they received lower scores from the examiners.
In the present study, the work of the students was assessed using the traditional analytical method. To further increase the credibility of the assessments, 2 independent examiners participated in the research. Each examiner evaluated the work of the students separately. The traditional analytical method of evaluation has been used in the field of dentistry for many years, and it is considered reliable and repeatable.24 A validated and properly executed assessment process can reduce students’ stress levels and have an impact on achieving better results in exercises. Studies indicate that the most significant sources of stress for students include assessments, exams, and the atmosphere created by clinical professors.25, 26 According to the literature, the level of specialist knowledge did not influence preclinical assessments based on the analytical method. Both younger and older lecturers reported similar results. Differences in assessments were only observed in groups with no prior experience in fixed prosthodontics.9, 27 Thus, it can be regarded as a universal method of assessment that can be successfully applied by less experienced individuals in the event of a shortage of senior training staff. However, the criteria for individual parameters should be precisely defined and the evaluators properly calibrated. Esser et al. observed significant discrepancies between the correlations of maxima and medians when examiners visually assessed students’ individual preparation parameters, thus indicating insufficient calibration of the evaluators.5 They emphasized that both targeted calibration and more precisely formulated criteria could improve the quality of results.5 The study noted a very high level of interexaminer reliability in the case of the wall convergence angle, cusp reduction height and margin width, as assessed using simple measuring tools. These results demonstrate that when an examination is correctly prepared, even simple methods and instruments such as a compass and a ruler may suffice to properly assess students’ work in preclinical classes. There was a moderate agreement between the evaluators with regard to parameters such as the extent of the preparation, surface smoothness, and finish line continuity. These parameters were assessed visually based on the established criteria. The evaluation of parameters that were not quantifiable was more difficult despite the existence of precise criteria and the calibration of examiners.
The conducted study emphasizes the importance of standardizing dental curricula across educational institutions as a pivotal component of dental education. This would ensure the uniformity of educational standards and enhance its quality. Additionally, the quality of dental education can be improved by the adoption of innovative teaching methods such as simulation-based training, formative assessments and other interactive techniques, as well as by the establishment of robust feedback systems to provide students with regular and constructive critiques of their work. There is a clear need for longitudinal studies assessing the long-term impact of educational interventions on clinical competency.
The strengths of the present study include comprehensive assessment, combining both quantitative and qualitative data. Moreover, a diverse sample provided a broad perspective on educational quality. The study also offers practical recommendations based on empirical evidence for conducting preclinical dental preparation courses.
Limitations
The present research was subject to certain limitations. It was conducted in a single educational center and only by 2 examiners. In the future, it would be beneficial to expand the research to include other university dental schools and increase the number of examiners. The criteria adopted for the study were not assessed by any independent external institution. Another limitation is the possibility of bias in the self-reported qualitative data, as well as the cross-sectional nature of the study, which lacks long-term outcome assessment. The present research was limited to the domain of tooth preparation and may not be generalized to other aspects of dental education.
Conclusions
A combination of theoretical and practical exercises allowed students to acquire basic knowledge and skills in the preparation of teeth for prosthetic crowns. In order to improve their performance during the more difficult stages of preparations, students need practical exercises and well-targeted feedback from instructors. Dentists who supervise students should pay particular attention to the parameters in which students achieved their lowest scores in terms of precision, namely the degree of wall convergence and the reduction in the height of both functional and non-functional cusps.
The traditional analytical approach to assessing the tooth preparation procedure is a reproducible method that examiners can use to effectively evaluate students’ work. Targeted calibration of the evaluators is essential to ensure more accurate results. Parameters that are not easily quantifiable are more challenging to evaluate.
Ethics approval and consent to participate
The study protocol followed the ethical guidelines established by the 1975 Declaration of Helsinki and was approved by the Institutional Ethics Committee at Jagiellonian University Medical College, Krakow, Poland (approval No. 118.6120.109.2023). Prior to their involvement in the study, each student provided informed consent.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.