Abstract
Background. Erbium family lasers have been used as an alternative method for the treatment of dental caries in deciduous teeth, in comparison to traditional methods.
Objectives. The study aimed to determine the most optimal erbium-doped yttrium-aluminum-garnet (Er:YAG) laser settings for carious lesions in deciduous teeth on different surfaces with the evaluation of treatment time and pain level on a visual analog scale (VAS).
Material and methods. The randomized clinical trial involved 66 teeth with deep caries in 33 children aged 3–8 years, divided into 2 study groups: Er:YAG laser (test group); and conventional treatment with a dental turbine (control group). The time required for caries removal and cavity preparation using both methods was recorded. The inclusion criteria encompassed generally healthy pediatric patients, pain-free subjects, first-time dental appointment, and unicuspid primary teeth with caries. Dental caries treatment was performed without the administration of local anesthesia.
Results. The cavity preparation time was on average 2.5 times longer when the Er:YAG laser was used compared to the conventional method. The study demonstrated the effectiveness of the Er:YAG laser in hard tissue preparation of deciduous teeth with a pulse energy of 230 mJ for enamel preparation, mainly on occlusal and proximal surfaces, and with a pulse energy of 120 mJ and 150 mJ for dentin preparation. Optimum operating frequencies were 10 Hz and 20 Hz with corresponding water consumption. The level of discomfort among the laser-treated patients indicated 0 based on VAS, meaning no pain. Among patients treated with the traditional method, the pain level averaged 5.27.
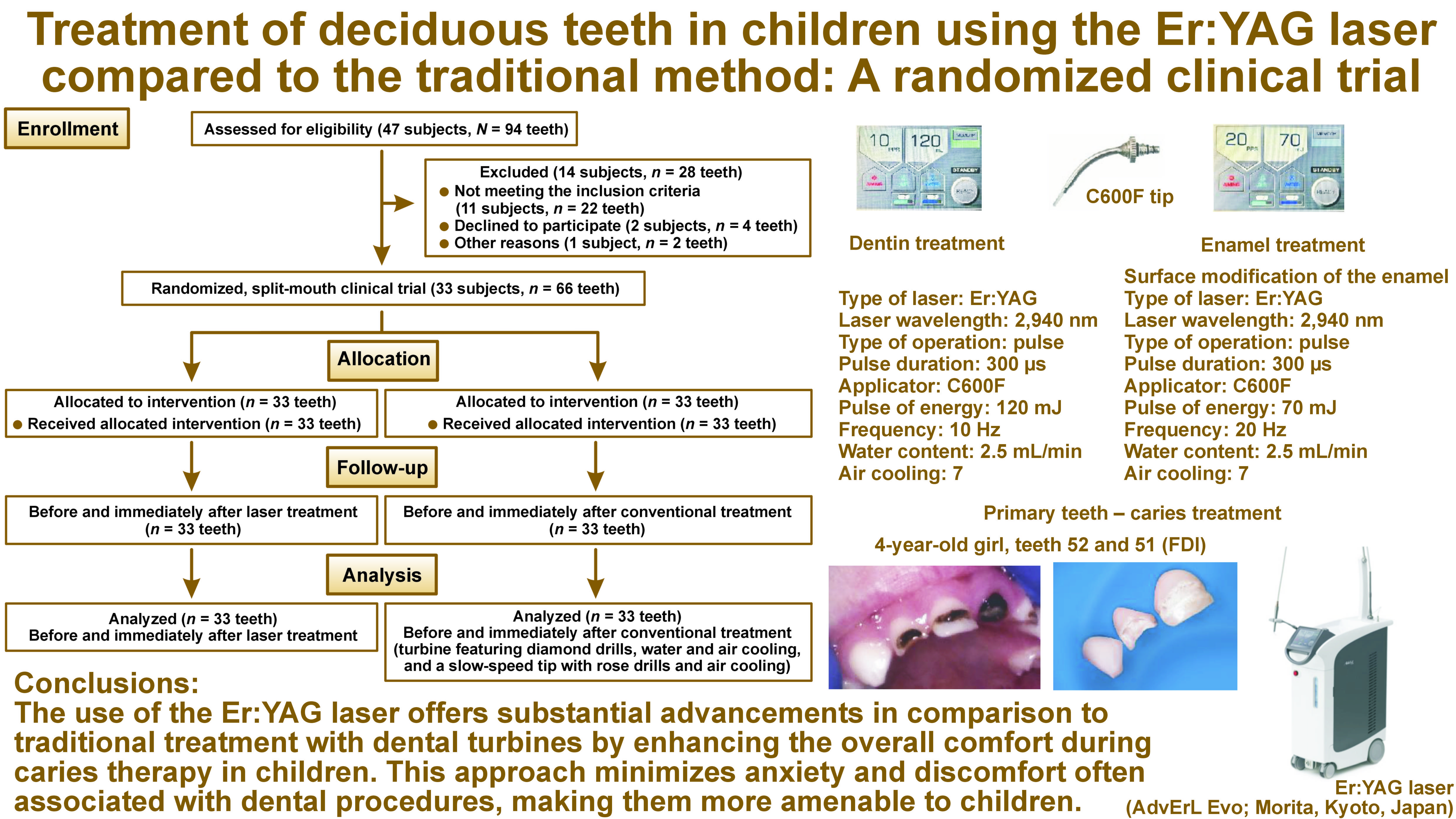
Conclusions. The use of the Er:YAG laser offers substantial advancements in comparison to traditional treatment with dental turbines by enhancing the overall comfort during caries therapy in children. It fosters better patient cooperation and reduces the need for intraoperative anesthetics due to its minimally invasive nature and the fact that it is a relatively quiet operation. This approach minimizes anxiety and discomfort often associated with dental procedures, making them more amenable to children.
Keywords: pain, dental caries, laser, primary teeth, Er:YAG
Introduction
Maintaining primary dentition until its natural replacement by permanent teeth is extremely important. Unfortunately, the treatment of primary teeth is still underappreciated by parents and dental practitioners. This phenomenon is also reflected in the limited number of scientific publications addressing this subject. If dental caries in primary teeth progresses to apical periodontitis, it can impact the tooth germ of the developing permanent teeth, increasing the risk of caries in newly erupted permanent teeth. The contemporary field of restorative dentistry for primary teeth places a significant emphasis on the utilization of minimally invasive techniques for the preparation and filling of carious lesions. Traditionally, turbine drills and micromotors were used. However, the loud sound and intense vibrations from rotary instruments often diminish children’s cooperation during treatment and contribute to the development of dental anxiety in children. Therefore, with the advancement of technology, there is an increasing demand for contemporary methods of caries treatment that do not provoke negative experiences in children. One such method involves the use of the erbium-doped yttrium-aluminum-garnet (Er:YAG) laser.1, 2, 3, 4 High-power laser light is known due to its bactericidal effect.5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18 This property of laser can reduce the risk of secondary infections and recurrent caries, contributing to long-lasting restorations. Erbium family lasers operate through a process known as thermo-mechanical ablation, as they are highly absorbed by the water chromophore within dental carious tissue. This interaction leads to the precise and minimally invasive removal of decayed tissue. The water content present in primary dental tissue is higher than in permanent teeth due to its lower degree of mineralization, which results in higher energy absorption. Lasers efficiently remove decayed and infected tissue without affecting the healthy parts of the tooth. Thus, lasers require different parameters for caries ablation in primary teeth compared to permanent teeth. However, current research has yet to establish definitive guidelines for the optimal physical parameters of the Er:YAG laser in the minimally invasive treatment of carious lesions in primary teeth. These teeth have a different structure from permanent teeth and thus require different physical parameters for proper cavity preparation.19, 20, 21
The null hypothesis of this study posits that the use of the Er:YAG laser for the preparation of carious lesions in primary teeth requires the application of a radiation beam perpendicular to the direction of enamel prisms and dentinal tubules, with appropriate low voltage delivered through a small-diameter optical fiber, along with significant water cooling. This approach is predicted to have no effect on pulp vitality and should not reduce pain sensations during the procedure.
The aim of the study was to determine the optimal settings for the Er:YAG laser in treating advanced lesions in the enamel and dentin of primary teeth on occlusal, interproximal and smooth surfaces. This investigation was conducted through the implementation of randomized clinical trials. The settings were compared to conventional methods for treating caries in primary teeth. The time required to prepare the cavity using the laser and conventional methods was examined. A pulp tester (Digitest® Pulp Vitality Tester; Parkell Inc., Edgewood, USA) was used to assess the impact of both methods on the pulp of the treated primary teeth before and immediately after cavity preparation. Additionally, the pain perception of young patients in both the laser and conventional groups was evaluated.22, 23, 24, 25
Material and methods
Ethics approval
The study was designed as a randomized controlled trial. The Ethics Committee of Wroclaw Medical University, Poland approved the study (approval No. KB-547/2021), and informed consent was obtained from all participating subjects, as stipulated in the Declaration of Helsinki. This study was registered with the ISRCTN (International Standard Randomised Controlled Trial Number) Registry under the reference No. 45696-OH7CP3.
Study sample
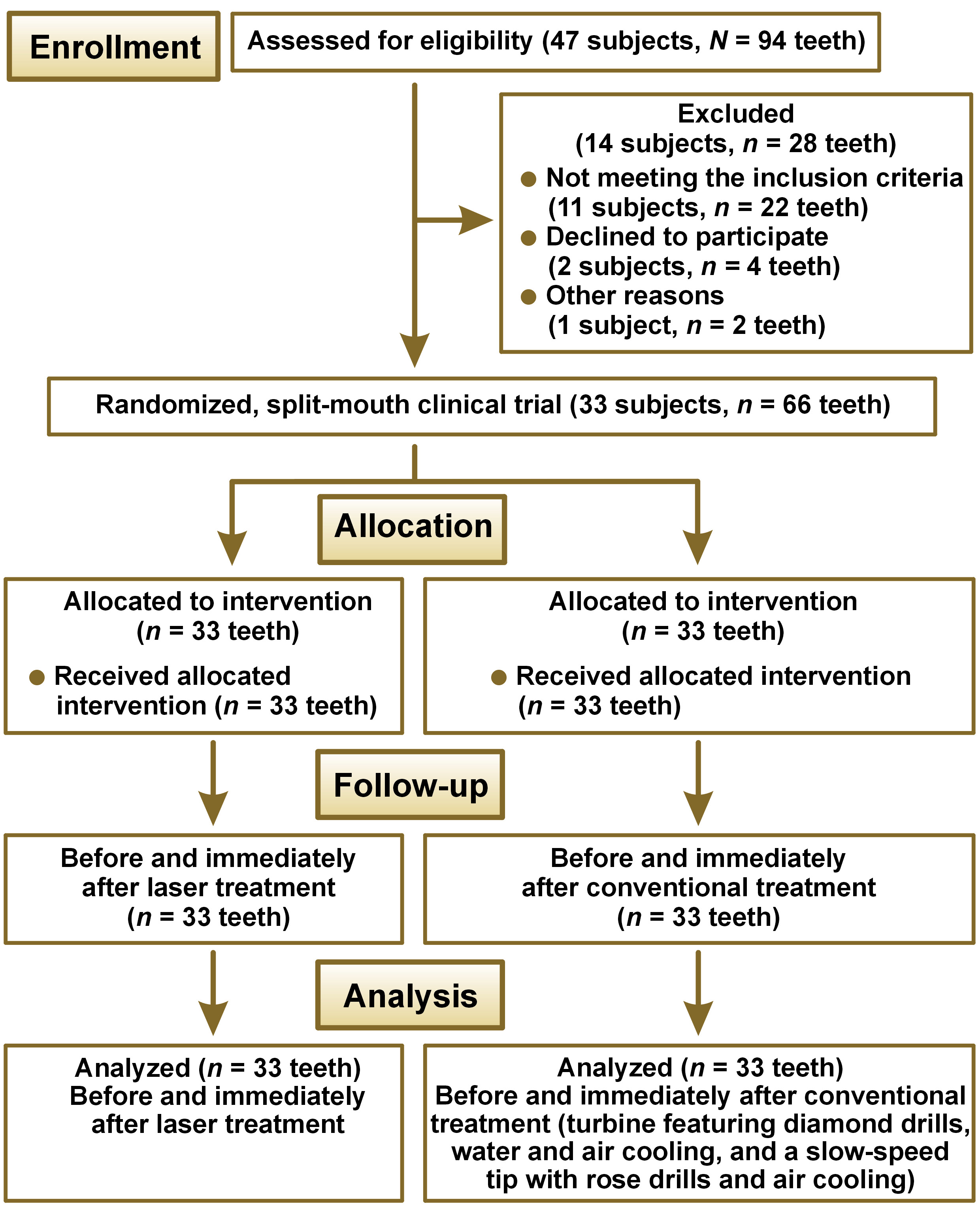
Initially, a total of 47 subjects (94 teeth) were evaluated for eligibility. Of these, 14 patients (28 teeth with caries) were excluded from the study. This group included 11 children (22 teeth) who did not participate due to previous dental office visits, 2 individuals (4 teeth) who refused to participate, and 1 patient (2 teeth) who dropped out of the study due to an existing systemic disease. This randomized, split-mouth clinical trial involved 66 teeth affected by deep caries (33 subjects of both sexes; age: 3–8 years). The sample size was calculated to be 33 in each group using the G*Power v. 3.1 (Kiel University, Kiel, Germany) software, assuming 80% power, 95% confidence intervals, a level of significance of 0.05, and d = 0.62, based on preliminary studies conducted on a smaller number of subjects. Each tooth on the test side (n = 33) of the maxilla or mandible was treated with the Er:YAG laser, while the teeth on the opposite side (n = 33) served as a control group and received conventional treatment (Figure 1).
The inclusion criteria encompassed children who had visited a dental office for the first time in their lives for a dental examination and possible conservative treatment, healthy children who were not taking any medication, subjects who did not report any pain when coming to the office, subjects aged 3–8 years, and patients with unicuspidal deciduous teeth with deep caries. The same dentist treated all patients.
The initial visit did not include caries treatment. Instead, the children underwent a series of adaptive visits, tailored to their age and individual needs. This was followed by a comprehensive dental examination that included oral hygiene instruction, dietary guidelines, and a procedure to clean plaque from all teeth. The dental examination was conducted using the DIAGNOcam™ Vision Full HD diagnostic device (KaVo, Biberach, Germany) to identify occlusal and proximal caries in primary teeth. Patients presenting with carious lesions of similar severity in unicuspidal teeth were eligible for inclusion in the study. The decision as to which tooth would be treated with the conventional method and which with the laser method, as well as the method of the initial cavity preparation were selected through computerized randomization (blinding). The computer program determined whether the initial preparation would be conducted using conventional methods or the Er:YAG laser.
The conventional treatment was initiated in 12 patients, and the laser was employed as the initial treatment modality in 21 patients. The conservative management of deciduous teeth was conducted without the use of anesthetics (Figure 1).
Treatment procedures
This study evaluated the efficacy of different treatment modalities for the removal of dental caries. One group of patients received treatment with the Er:YAG laser (AdvErL Evo; Morita, Kyoto, Japan), while the other group was treated with a turbine featuring diamond drills, water and air cooling, and a slow-speed tip with rose drills and air cooling.
Characteristics of the conventional method
In the traditional method, a turbine with blue-coated diamond drills (19 mm long, sizes 012–018), as well as water and air cooling were employed to create the cavities and work on enamel. For dentin preparation, a slow-speed carbide tip (22 mm long, sizes 018–021) with air cooling was used. The restorative material was glass ionomer.
Laser settings
A summary of the laser settings utilized for each group of cavities is presented in Table 1, Table 2, Table 3. The following Er:YAG laser parameters were employed in the enamel on all surfaces: a frequency of 10 Hz for cavity opening and 20 Hz for enamel modification; a pulse energy of 160 mJ with a 400-μm diameter applicator and 230 mJ. The 600-μm diameter applicator was used to develop cavities on the proximal and occlusal surfaces. On smooth surfaces (palatal and labial) of anterior teeth, a pulse energy of 150 mJ with a 600-μm diameter and a pulse energy of 180 mJ with a 800-μm diameter were applied.
In the surface modification procedure, the pulse energy was set at 50 mJ and 70 mJ for 400-μm and 600-μm diameter applicators, respectively. The water content values oscillated between 2.5–3.0 mL/min, and the air cooling was set to 7 on a scale from 1 to 10.
The parameters employed in dentin across all cavity classes were as follows: a frequency of 10 Hz, a pulse energy of 120 mJ with a 600-μm diameter applicator, and 150 mJ with an 800-μm diameter applicator, respectively. The water content was used at a rate of 2.0–2.5 mL/min, and the air cooling was set to 7 on a scale from 1 to 10. The pulse duration was maintained at 300 μs throughout the enamel and dentin treatment (Table 1).
Laser applicators, type of primary teeth and working surfaces
The procedure was conducted in a non-contact mode, with the applicator positioned 1 mm from the target area in both enamel and dentin. The occlusal and proximal surfaces of the enamel in deciduous molars were treated with applicators that had a diameter of 400 μm and 600 μm. The smooth palatal and labial surfaces of the enamel in incisor and canine teeth were treated with a 800-μm diameter applicator. Regardless of the cavity class, dentin was treated with applicators having diameters of 600 μm and 800 μm.
During the operation, the applicator was positioned at a 90° angle to the tooth surface. This angle was selected as the ideal impact angle for laser ablation of enamel, as it is perpendicular to the orientation of the prisms. The procedure was performed with slow, overlapping movements, following the recommendations outlined in Table 2.
Pulp vitality
The Digitest® Pulp Vitality Tester was employed to assess the vitality of the dental pulp. The device quantifies pulp vitality on a scale ranging from 0 to 80 (0–40 – vital pulp; 40–80 – pulpitis; <80 – necrotic pulp). The pulp responses of deciduous teeth were studied using both traditional and laser methods.
Working time
In the preparation of carious cavities in deciduous teeth, the working lengths were measured using conventional methods and the Er:YAG laser with the aid of a stopwatch.
VAS scale
Following the conventional and laser treatment visits, patients were asked to rate their pain sensations using emoticons according to the visual analog scale (VAS).23, 24 The results were collected and documented separately for the laser method and separately for the conventional method.
Statistical analysis
In order to answer the research questions and test the hypotheses, the statistical analysis was performed using the IBM SPSS Statistics for Windows software, v. 26.0 (IBM Corp., Armonk, USA). The Student’s t-test was employed for both dependent samples, with p < 0.05 indicating the level of statistical significance.
Results
The study’s participants included 33 subjects who underwent treatment with laser and conventional methods. The distributions for the treatment characteristics in both methods were examined sequentially. The laser method was divided into 3 stages, namely enamel treatment, dentin treatment and enamel modification. For each method, the teeth most frequently treated were molars (69.7%). A mere 18.2% of the treated teeth were incisors, while the remaining 12.1% comprised canines.
Characteristics of treatment methods
Further characterization was related solely to the laser method. The most frequently selected applicator type in the laser method for enamel work was the C600F applicator (54.5%). Over one-third (36.4%) of the enamel work settings were allocated to the C400F applicator. The remaining parameters (9.1%) pertained to the C800F applicator. In the context of dentin or enamel modification, the majority of settings (60.6%) were associated with the C600F applicator. In the remaining cases (39.4%), the applicator type was identified as C800F.
For enamel work, the pulse energy was predominantly 160 mJ (48.5%) and 230 mJ (33.3%). The remaining cavity preparations were based on pulse energies of 150 mJ (9.1%) and 180 mJ (9.1%). In the case of dentin, the pulse energy was lower. In the majority of cases, the energy level was set at 120 mJ (60.6%). The remaining studies on dentin employed a pulse energy of 150 mJ (39.4%), while enamel modification was treated with a weaker energy of 50 mJ (60.6%) and 70 mJ (39.4%).
The frequency for cavity preparation on enamel and dentin was 100.0% at 10 Hz, while for enamel modification, the frequency was 20 Hz (100.0%). During the process of cavity preparation in the enamel area or its modification, the water content was maintained at a level of 2.5–3.0 mL/min. In the dentin area, this value was lower (2.0–2.5 mL/min). The area setting for all laser preparations was set to 7, and in each case, the pulse duration was 300 μs. Table 3 presents the discussed data on the characteristics of both methods.
Subsequently, basic descriptive statistics were calculated for the variables of patient age, time to complete cavity treatment, pain as measured by the VAS, and pulp vitality before and after treatment. The calculations are presented separately for subjects treated with the laser method and separately for those treated with the conventional method (Table 4).
The analysis revealed that the average age of the children was 5.27 ±1.42 years. The youngest child was 3 years old, while the oldest was 8. The mean time to complete cavity preparation was 195.94 ±30.13 s among patients treated with the laser method. The shortest total cavity preparation time was recorded at 147 s, while the longest was 254 s. The mean time to complete cavity repair using the conventional method was 77.67 ±11.09 s. The shortest amount of time to complete cavity repair was 50 s, while the longest amount of time to complete cavity repair was 97 s. The level of discomfort measured by the VAS among the laser-treated patients was 0, indicating no pain. Among the subjects treated with the traditional method, pain levels exhibited a mean of 5.27 ±2.34, with the lowest recorded level at 2 and the highest indicating maximum pain intensity. In the group that received laser treatment, pulp vitality remained at the same level before and after the intervention (25.82 ±0.85). The lowest recorded value for pulp content in this group was 25, while the highest was 27. Among the children treated with the traditional method, differences were observed between the pre-operative and post-operative measurements. The pre-treatment mean pulp content was found to be analogous to that observed in the laser group, with a value of 25.88 ±0.82. The lowest recoded value for pulp compactness was 25, while the highest was 27. Following treatment, the value increased to 32.30 ±2.01. The lowest recorded value for pulp compactness was 29, while the highest was 35.
Descriptive statistics of the measured quantitative variables
In the subsequent phase of the analysis, the distribution of the quantitative variables was evaluated. This objective was achieved by calculating basic descriptive statistics and applying the Shapiro–Wilk test to determine the normality of the distribution. The results of this analysis are presented in Table 5.
The Shapiro–Wilk test results were found to be statistically insignificant for the time of complete cavity preparation, irrespective of whether a laser or traditional methods were employed. This finding suggests that, when categorized into 2 groups, this variable approached a normal distribution. In contrast, the results of the normality of distribution test suggest a distribution that does not align with the Gaussian curve for the other variables. Nevertheless, the absolute value of the skewness for each variable did not exceed 2, indicating a slight asymmetry in these distributions. Therefore, the analyses were based on parametric tests, provided that the remaining assumptions of these tests were met.
Differences in total cavity preparation time according to the method
In the subsequent stage of the statistical analysis, the total preparation time for 2 methods of cavity preparation, namely the laser method and the traditional method, was compared using the Student’s t-test for dependent samples (Table 6).
The test results were found to be statistically significant, indicating the presence of a substantial observed effect. This finding suggests that there are differences between the methods in terms of the time required to complete the cavity, with the laser method requiring more time than the conventional method.
Pulp vitality before and after conventional treatment
Subsequently, the vitality of the pulp was evaluated before and after treatment using the Student’s t-test for independent samples. This analysis was conducted exclusively in the conventional treatment group. In the group that underwent laser treatment, the pulp vitality values remained consistent before and after the procedure.
The results of the test were found to be statistically significant, indicating the presence of notable differences between the measurements of pulp vitality (Table 7). The observed effect was of high power. In the cohort of subjects who received the conventional treatment modality, the values for pulp vitality were found to be significantly higher after treatment in comparison to the pre-treatment values. This finding suggests that the procedure may have had an adverse effect on the vitality of the pulp.
Discussion
The utilization of laser technology in restorative dentistry remains a novel concept, not only in how it changes traditional treatment approaches but also in the manner in which it is perceived by dental professionals and their patients. The utilization of the Er:YAG laser for the treatment of carious enamel and dentin defects provides a more comfortable and safer experience for young patients when compared to conventional methods. The paucity of literature on the laser treatment of deciduous teeth underscores the importance of further research in this area, with the aim of developing a protocol for the appropriate use of the Er:YAG laser on the hard tissue of deciduous teeth. The objective of this study was to identify the most optimal physical settings of the Er:YAG laser for the treatment of carious lesions in the enamel and dentin of deciduous teeth on occlusal, tangential and smooth surfaces. A randomized clinical trial was conducted to compare the parameters of the Er:YAG laser settings for the conservative treatment of deciduous teeth in children with those of the conventional method.
The present study examines the reaction of children to the applied treatment, with a focus on the assessment of pain according to the VAS. The results demonstrated that pediatric patients who underwent laser treatment did not report any pain, despite the absence of local anesthesia. Conversely, the findings indicated that the patients participating in the study perceived the conventional method to be less favorable. The children reported pain, as evidenced by the VAS findings. Other researchers have evaluated the pain experienced during the use of the erbium, chromium:yttrium-scandium-gallium-garnet (Er,Cr:YSGG) laser on permanent teeth in children24 and during Er:YAG laser treatment on deciduous teeth.1, 25, 26, 27, 28, 29
The study also evaluated the time duration required for the laser treatment and the conventional treatment. The results indicated that operating the laser required approx. 2.5 more time than the conventional method. Nevertheless, the children aged 3–8 years who participated in the study found the laser method more acceptable.
In conclusion, in accordance with the results of preceding studies, the preparation time for laser treatment is approximately twice as long as that for rotary instruments. However, for pediatric patients, the duration of treatment is not the primary concern; rather, pain is the most important factor contributing to uncooperative behavior. Other studies have demonstrated that 70% of children felt more comfortable during laser cavity preparation. In comparison, a mere 30% of children expressed a similar level of comfort during conventional cavity preparation. The study demonstrated that the utilization of laser during tooth preparation requires more time compared to conventional methods. Nevertheless, children exhibit greater cooperation and calmness during laser treatment, leading to their preference for this method in subsequent visits.27, 30, 31 The aforementioned advantages of lasers in pediatric dentistry result in a less traumatic experience for young patients, thereby enhancing their acceptance of the procedure.
Eren et al. evaluated the duration of laser cavity preparation and compared it to conventional methods in sixth molars in patients aged 7–10 years.26 The laser preparation took an average of 7.4 min, while mechanical preparation took an average of 3.7 min. Liu et al. also investigated the duration of laser cavity preparation and compared it to conventional methods for deciduous teeth preparation.29 The working time with the Er:YAG laser was approx. 2.35 times longer than that required for cavity preparation using conventional methods.
Laser tooth preparation entails the minimally invasive and selective removal of infected carious tissue from cavities. The utilization of laser techniques in hard tissues yields a minimal thermal effect or a complete lack of thermal effect in the pulp of teeth undergoing preparation.31, 32, 33, 34 This topic was also addressed in our work, wherein we employed the pulp tester to examine the pulp of the teeth under consideration. The results established that the laser technique does not have an influence on the condition of the pulp. In contrast, the utilization of rotary instruments has been demonstrated to enhance pulp viability following mechanical pulp treatment.
In the present study, a frequency of 10 Hz was employed for both enamel and dentin preparation, while 20 Hz was used exclusively for enamel modification. Upon analysis of other research papers and the frequency values cited therein, a significant discrepancy was observed, ranging from 2 Hz35 to 20 Hz8, 36 and 25 Hz.37 The researchers did not differentiate between the values of the applied frequency according to the work in enamel and dentin. In the context of laser applications, the frequency values of the Er,Cr:YSGG laser ranged from 20 Hz to 25 Hz,22, 30, 36 while those of the Er:YAG laser ranged from 2 Hz to 10 Hz.29, 35, 38 A review of the literature failed to reveal any rationale behind the significantly higher frequencies employed when using the Er,Cr:YSGG laser compared to the Er:YAG laser. Furthermore, none of the other studies analyzed such a relationship.
The frequency value appears to be important in the context of hard dental tissues. The operational speed of the Er:YAG laser is influenced not only by the laser beam parameters and the operator’s expertise but also by the chemical composition of the hard dental substance to be treated (enamel, dentin). Enamel is composed of 95% hydroxyapatite, 4% water and 1% collagen fibers, while dentin is composed of 70% hydroxyapatite, 20% collagen fibers and 10% water.39 The hard tissue of the tooth affected by caries contains more water than healthy tissue, which means that the speed of laser treatment in dentin is higher than that in enamel. This allows the caries tissue to be removed more easily and quickly than healthy tissue. It is essential to control the parameters during laser cavity treatment in accordance with the principles of minimally invasive dentistry. When working in enamel, the frequency parameters may exceed those employed in dentin, particularly within the region of the intraosseous wall.37, 40
Another parameter that was assessed was the diameter of the applicator used. The diameter of 600 μm (C600F) was identified as the most frequently used applicator. The diameter of 400 μm (C400F) was primarily employed for cavity opening and enamel working, whereas the diameter of 800 μm (C800F) was utilized for dentin treatment in cavities with a larger surface area. The present study delineated the area and type of tooth on which the applicator was utilized in detail. In each case, it was stated whether the contact or non-contact treatment was used, the movements executed during the treatment, the angle at which the applicator was positioned in relation to the tissue being treated, and the type of cavity and tooth treated. Observations revealed that the pulse energy was higher when working in enamel and lower when working in dentin.
A review of the available research papers21, 29, 30, 35, 36, 38, 40, 41, 42, 43 revealed that it is not possible to ascertain which parameters were employed to treat a specific tooth surface or to remove caries in enamel and dentin. A single paper provided this information, stating the fluence, the applicator type, the diameter, the non-contact mode 1 mm from the target area, the type of teeth (canines), and the surface to be treated (class V cavity).36 The study did not specify the angle of the applicator in relation to the working surface and the type of movement performed by the operator. The study by Rossi et al. appears to be one of the most accurate among the works evaluated, containing the data necessary for determining the optimal physical settings of the Er,Cr:YSGG laser for working in the enamel and dentin of deciduous teeth in a class V cavity.36
The study by Valério et al. employed a 900-μm diameter applicator in a non-contact mode with a focal distance of 7 mm, utilizing a non-contact head.38 In contrast, Johar et al. used a 600-μm diameter applicator in a non-contact mode, yet the distance from the surface to be treated and the type of applicator were not specified.30 None of the papers provided information on the specific tissues that the given parameters were used for, nor did they indicate whether the parameters were applied to enamel or dentin of deciduous teeth.
Following the analysis and evaluation of the laser settings in the presented studies, it is evident that despite specifying the diameter of the applicator used,21, 29, 30, 35, 36, 38 only 3 publications31, 42, 43 described the type of applicator. Furthermore, none of the reviewed studies specified the angle of the applicator in relation to the treated tissue or the type of movement performed during the procedure. All of the evaluated studies used the non-contact mode, with the distance from the target area varying between 1 mm,21, 29, 36 7 mm37 and 17 mm,35 with no specification of the length from the working surface.30 However, the values provided do not elucidate the reason behind the selected distances, such as the rationale behind the choice of 1 mm in one instance and 7 mm or 17 mm in another.
In many studies, the data concerning the applicator type and diameter were described in general terms, without linking them to the specific tissue or tooth type. Several publications, including those by Rossi et al.,36 Valério et al.,38 and Johar et al.30 have explicitly examined primary dentition. However, most of the reviewed studies failed to specify the movements performed while operating in the hard tissue, nor did they indicate the angle of incidence of the laser beam, which are crucial parameters for standardizing laser-based protocols in pediatric restorative dentistry.
The studies on the treatment of permanent teeth (with regard to the type of tissue to be treated) revealed a more detailed treatment algorithm, which was not included in the studies on deciduous teeth. In their description of laser treatment of cavities in permanent and deciduous teeth in children with the Er:YAG laser, Kato et al. provided detailed information on the pulse duration, type, and diameter of the applicator used, as well as the physical parameters of the laser applied to enamel and dentin.28 However, the authors did not specify the movement of the applicator when working in hard tissue and did not distinguish between working in deciduous and permanent teeth. Consequently, the paper is not suitable for determining the baseline parameters of the physical settings of the laser for any type of tooth.28
The analysis by Eren et al. describes the specific head and applicator used and is the only study to specify the movements of the applicator.26
Based on the published studies, it can be claimed that the use of erbium lasers is beneficial due to the lack of contact with tooth tissues and the absence of vibration.26, 29, 31, 34, 35, 44, 45, 46 A significant proportion of children (90%) accept laser tooth treatment, whereas patients aged 10 years and older show no preference between laser and conventional treatment methods.1, 46 The reduction of turbine noise is of particular significance for children, given the importance of comfort during operation.26, 29, 31, 34, 35, 44, 45, 47 In the majority of cases, laser treatment indicates the absence of local anesthesia,20, 24, 29, 30, 31, 34, 35, 36, 38, 41, 42 as observed in the present study. In our study, the difficulty of removing carious lesions from the lateral walls of the cavity was not evaluated, as previously described by Valério et al.38 The removal of carious lesions from the lateral cavity walls is more challenging than conventional methods, as the laser applicator does not function in the same manner as a bur. Future studies should aim to investigate the preparation of infected dentin from the lateral cavity wall.
Upon analysis of data from our study and other research papers, it can be concluded that there is a pressing need for further laboratory and clinical studies. It is imperative that the data included in a research publication adheres to the following protocol: firstly, the laser wavelength employed in the study should be specified; then, the type of the head used, the type of the applicator, the diameter of the applicator, the mode of operation (contact or non-contact), the distance of the applicator from the tissue being treated, and the angle of the applicator’s movement should be outlined. Additionally, the position of the applicator in relation to the tissue being treated, the type of movement performed, the type of tissue being treated (enamel or dentin), the type of tooth to be treated (deciduous, immature or mature permanent tooth), the surface of the tooth to be treated, and finally, the physical parameters of the laser (pulse duration, frequency, pulse energy, power, as well as water spray and air cooling) must be specified.
Conclusions
Er:YAG lasers offer a promising alternative to traditional rotary instruments for treating caries in primary teeth. The best results were achieved for enamel preparation using the 600-μm diameter applicator with a pulse energy of 230 mJ, mainly on occlusal and proximal surfaces. For dentin preparation, the optimal outcomes were obtained when using the applicator with the 600-μm diameter, and a pulse energy of 120 mJ, or the 800-μm diameter with a pulse energy of 150 mJ. In the context of the enamel modification procedure, positive results were obtained using the 400-μm applicator at a pulse energy of 50 mJ and the 600-μm applicator at a pulse energy of 70 mJ. The optimal operating frequencies of 10 Hz (enamel and dentin caries) and 20 Hz (enamel modification) were identified, with a water spray volume of 2.5–3.0 mL/min (enamel) and 2.0–2.5 mL/min (dentin). Despite the extended treatment duration, the reduction in pain and the preservation of pulp vitality make laser treatment a favorable option for pediatric patients. Further research is necessary to refine laser settings and improve the efficiency of this technique.
Trial registration
The trial was registered with the ISRCTN (International Standard Randomised Controlled Trial Number) Registry under the reference No. 45696-OH7CP3.
Ethics approval and consent to participate
The Ethics Committee of Wroclaw Medical University, Poland, approved the study (approval No. KB-547/2021), and informed consent was obtained from all participants, as stipulated in the Declaration of Helsinki.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.