Abstract
Background. Rapid maxillary expansion (RME) is a common treatment for maxillofacial skeletal abnormalities. Numerous studies have explored the impact of RME on skeletal, dental and nasal structures.
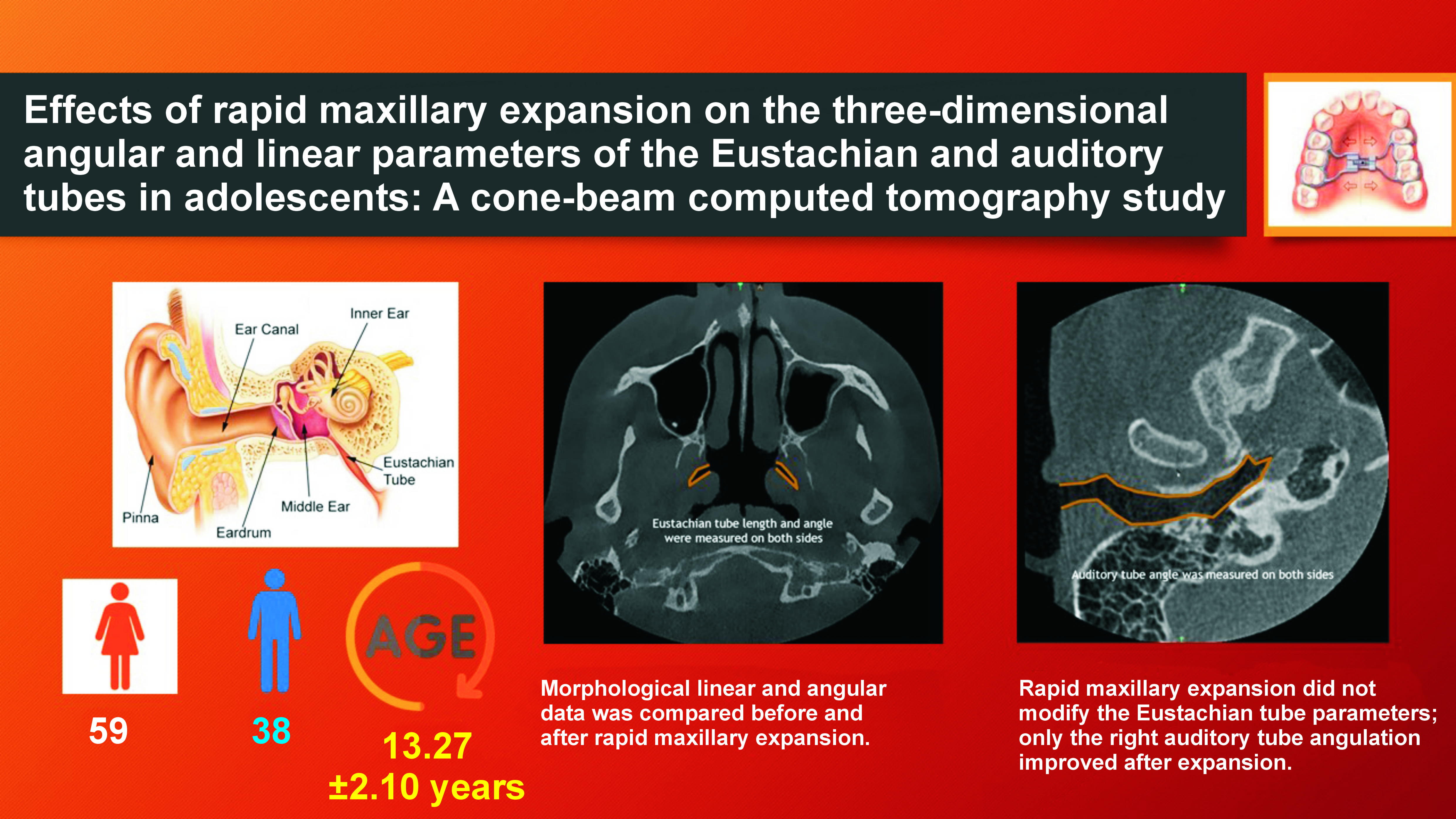
Objectives. The aim of the study was to evaluate the effects of RME on the three-dimensional (3D) Eustachian tube (ET) and auditory tube morphologies of adolescents using cone-beam computed tomography (CBCT).
Material and methods. A total of 97 patients (59 females and 38 males; age: 13.27 ±2.10 years) with maxillary transversal deficiencies who had undergone orthodontic RME were enrolled in the study. The treatment concluded when a cusp-to-cusp relationship was achieved between the palatal cusp of the maxillary first molar and the buccal cusp of the mandibular first molar. Cone-beam computed tomography was performed before maxillary expansion (T0) and after expansion (T1). The measurement of 2 linear and 4 angular, 3D, right and left ET parameters, as well as the ET and auditory tube angles, was conducted. The paired t-test was used to compare the data.
Results. There was no significant difference between T0 and T1 in any angular or linear ET parameters or the left auditory tube angle (p > 0.05). The T0 right auditory tube angle was significantly greater than the T1 angle (p < 0.05). Rapid maxillary expansion did not modify the 3D ET parameters; only the right auditory tube angulation improved after expansion.
Conclusions. Compared to conventional radiography, CBCT provides better morphological, angular and linear data regarding the ET and auditory structures. No significant differences were observed in linear or angular ET parameters based on the status of maxillary expansion treatment. The right auditory tube angle differed significantly between T0 and T1.
Keywords: rapid maxillary expansion, cone-beam computed tomography, Eustachian tube, auditory tube
Introduction
Rapid maxillary expansion (RME) is commonly used to treat skeletal transverse maxillary constriction, an upper-jaw skeletal discrepancy in the transverse plane associated with a posterior dentoalveolar crossbite, a narrow deep palate, nasal obstruction, and/or abnormal oral breathing. Numerous studies have explored the impact of RME on skeletal, dental and nasal structures.1, 2 The maxilla is linked to the cranial base and facial bones; therefore, RME may have an effect on these regions. Conductive hearing loss attributable to middle ear and Eustachian tube (ET) issues improved after RME.3, 4, 5, 6 The Eustachian tube is a rigid, epithelium-covered tube extending from the nasopharynx to the middle ear. The Eustachian tube, composed of bone and fibrocartilage, plays a crucial role in the proper functioning of the middle ear. The length and angle of the ET determine the nasopharyngeal content of the middle ear. Tubal disturbance has been observed to be more prevalent in individuals with very deep palatal vaults and malformations of the palate and nasopharynx.7, 8, 9 Studies on cleft palate have emphasized the relationship between the upper palate and the ET. In such subjects, the etiology of ET malfunction is attributable to the abnormal insertion of the tensor veli palatini and levator veli palatini muscles.7, 8, 9, 10, 11, 12 Bluestone et al. discovered a relationship between poor ET function and the incidence of chronic otitis media in patients with cleft lip and palate who had or had not received surgery.12 Maxillary and nasopharyngeal tissue expansion advances the pharyngeal ostium of the ET. Thus, RME may be useful in the treatment of hearing impairments associated with ET dysfunction.13, 14 The vast majority of angular and linear ET measurements have been derived with the aid of general computed tomography (CT). Cone-beam computed tomography (CBCT) is associated with a low radiation dosage, a short imaging period and better image quality. Additionally, CBCT produces multiplanar three-dimensional (3D) images and models, facilitating the analysis of the craniofacial skeleton.15 To the best of our knowledge, no prior study has used CBCT to investigate the effect of RME on 3D ET morphology. In this study, we measured angular and linear ET parameters in adolescents.
Material and methods
The clinical research protocol was reviewed and approved by the Clinical Research Ethics Board of Eskisehir Osmangazi University, Turkey (approval No. 2018-58). Informed consent was obtained from all subjects and/or their legal guardian(s). All patients were referred to the Orthodontic Clinic at the Faculty of Dentistry of Eskisehir Osmangazi University for treatment of transverse maxillary constriction between 2016 and 2019. In this retrospective study, a total of 97 patients (59 females and 38 males) with a mean age of 13.27 ±2.10 years were enrolled. Patients with unilateral or bilateral crossbites, maxillary transversal deficiencies and deep palatal vaults were included in the study and received orthopedic therapy using a hybrid RME appliance. No patient exhibited any maxillo- or craniofacial malformations, or a cleft lip or palate. None of the patients had previously received any orthodontic or orthognathic surgery. A hybrid RME device was used to treat all patients. After the induction of local anesthesia, 2 mini screws (Standard 2.0 mm × 7 mm LOMAS mini screws; Mondeal Medical Systems GmbH, Mühlheim an der Donau, Germany) were inserted 2 mm medial to the suture sites in the anterior palatal region. Anterior maxillary expander screws (Palatal-S Split Screws; FORESTADENT, Pforzheim, Germany) were connected to the mini screws using acrylic plates. The posterior arms of the expanders were laser-welded to the first maxillary molars via molar bands. The posterior parts of the hybrid RME appliances were cemented to the first molars using multi-cure glass ionomer cement (3M Unitek, Monrovia, USA). The acrylic anterior part of each RME device was bonded to the palatal mini screws using a flowable composite. Parents were instructed to rotate the RME appliance by 25% twice daily until a cusp-to-cusp relationship was established between the palatal cusp of the maxillary first molar and the buccal cusp of the mandibular first molar. Then, the expansion screw was secured with a flowable composite that is capable of light curing.16
Ultra-low-dose CBCT was performed prior to maxillary expansion (T0) and after expansion (T1). Clinical changes in the anatomy and morphology of the maxilla and the ET bony structures were evaluated.
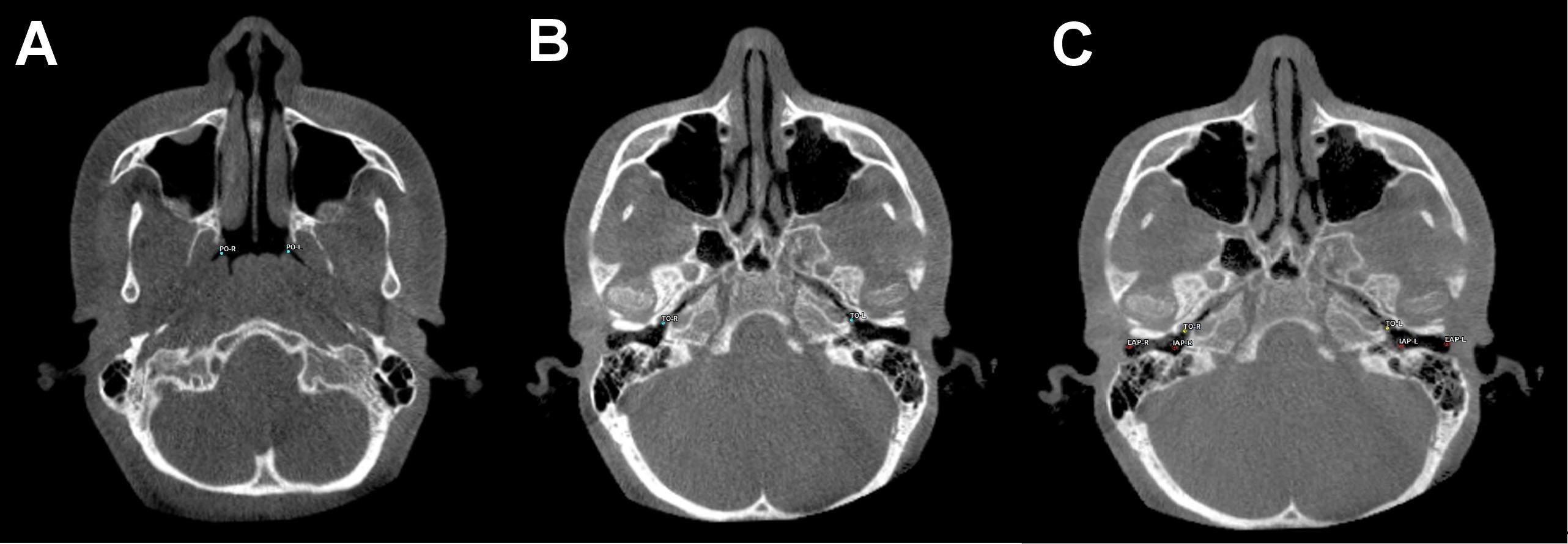
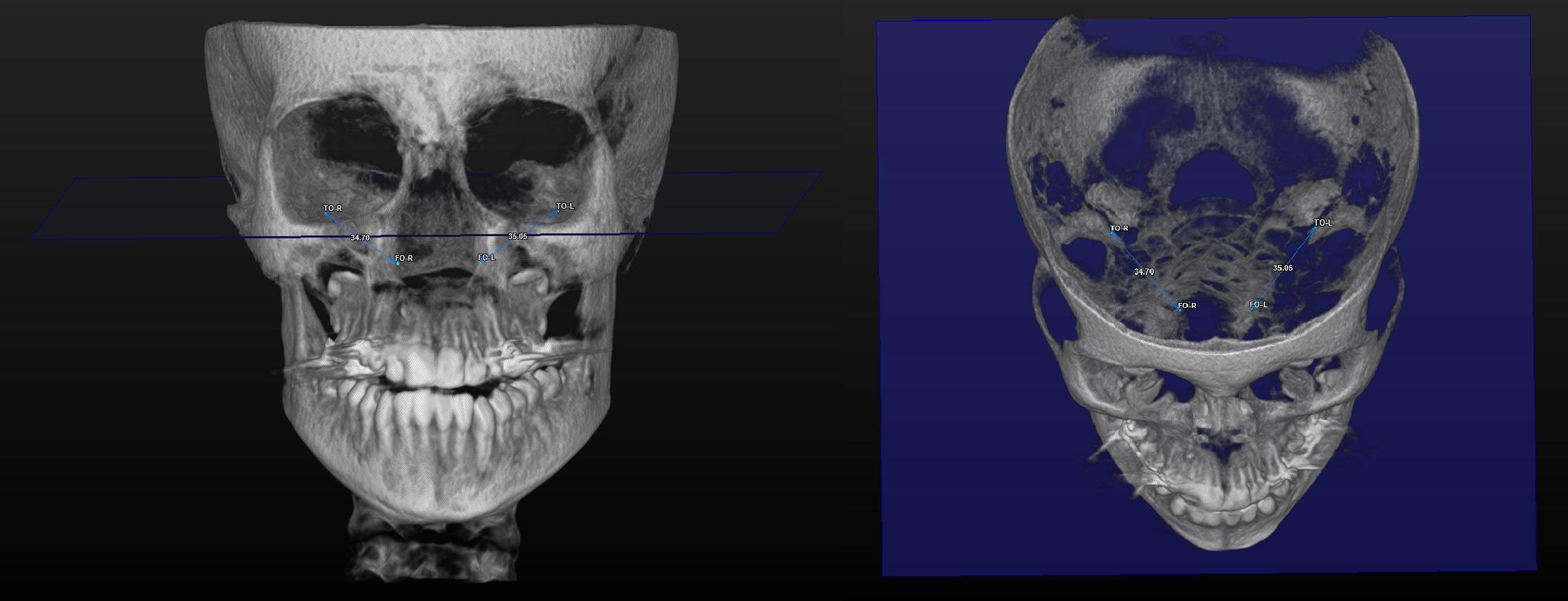
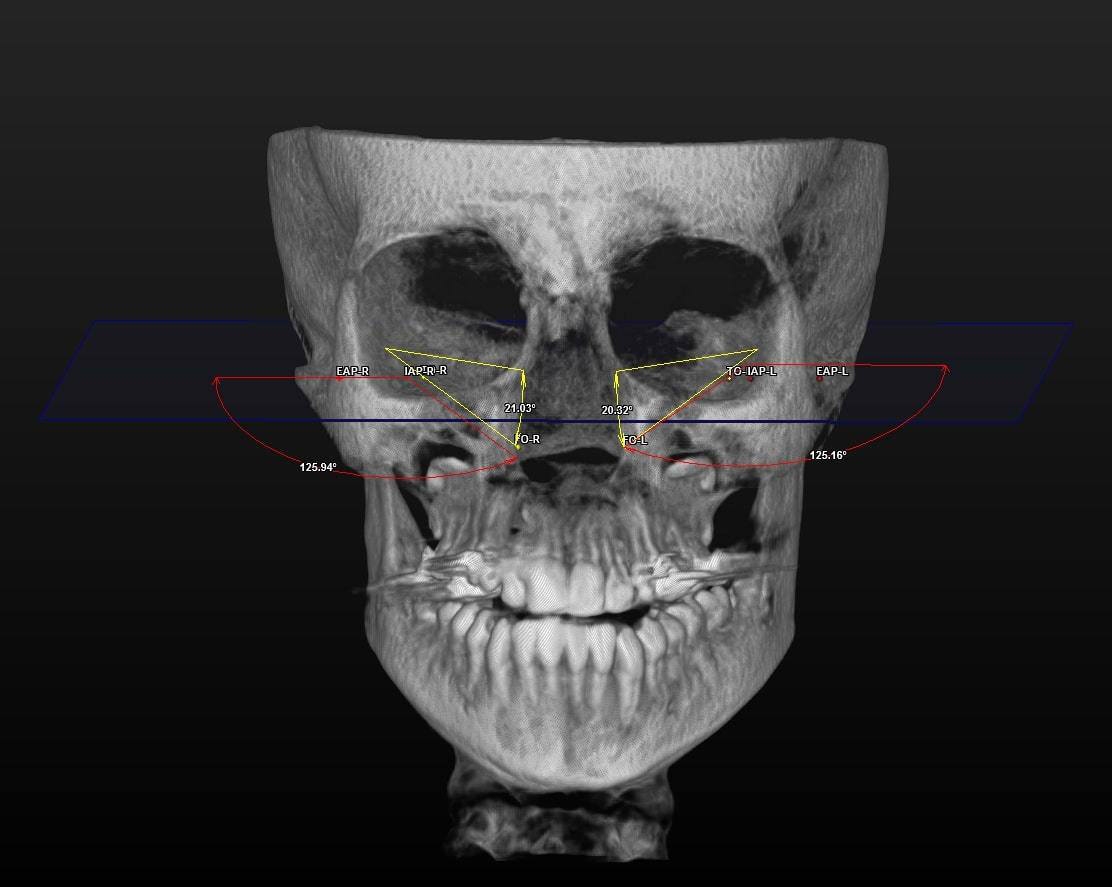
All 3D CBCT images were obtained with patients in a standing position using a CBCT device (ProMax® 3D Mid; Planmeca, Helsinki, Finland). The settings were as follows: 94 kVp; 14 mA; and 27 s. The images were consistent with the field of view (FOV) (20.0 cm × 20.0 cm × 10.2 cm) and voxel size (0.600 mm). The assessment of all CBCT images was conducted in 3D by a single clinician. The SimPlant® O&O image software (Materialise Dental N.V., Leuven, Belgium) was used for 3D image evaluation. The 3D morphological linear and angular parameters are listed in Table 1. The 3D morphological ET traces are displayed in Figure 1, Figure 2, Figure 3.
Statistical analysis
The descriptive statistics were compared using Microsoft Excel (Microsoft Corp., Redmond, USA) (Table 2). The statistical analyses were conducted using MedCalc software for Windows, v. 17.5 (MedCalc Software Ltd, Ostend, Belgium). The Kolmogorov–Smirnov test indicated that the data was non-normally distributed. The paired samples t-test was used to evaluate the statistical significance of the observed differences between the T0 and T1 measurements. The significance level was set at p < 0.05.
In order to ensure the reliability of the methodologies, each measurement was collected twice, separated by a designated time period. The intraclass correlation coefficient (ICC) was used to determine the accuracy of the radiographic measurements in terms of intraobserver reliability. The mean ICC was 0.91, indicating that the radiographic measurements were accurate (p > 0.05).
Results
The patients included in the study were referred to the orthodontic clinic for treatment of transverse maxillary constriction. The subjects included individuals with unilateral or bilateral crossbites, maxillary transversal deficiencies, and deep palatal vaults. These patients received orthopedic therapy using a hybrid RME appliance.
The comparison of the 3D linear and angular data is presented in Table 3. The mean right ET lengths were 36.26 ±3.10 mm at T0 and 36.13 ±3.08 mm at T1. Before and after RME, the mean left ET lengths were 36.82 ±2.98 mm and 36.82 ±3.12 mm, respectively. The right and left ET lengths did not differ significantly between T0 and T1 (p = 0.513 and p = 0.978, respectively). The mean right ET angle was 22.23 ±3.72° before RME and 22.82 ±4.06° after RME. At T0, the mean left ET angle was 22.33 ±4.22°. At T1, the mean left ET angle was 22.74 ±3.84°, indicating a non-significant difference (p = 0.077 and p = 0.184, respectively). The right auditory tube angle at T0 exhibited a significant increase compared to that at T1 (p = 0.000). The mean left auditory tube angles were 127.87 ±3.28° at T0 and 127.53 ±3.45° at T1 (p = 0.197).
Discussion
In the present study, no statistically significant difference was identified between T0 and T1 in left or right angular or linear ET parameters and the left auditory tube angle. The T0 right auditory tube angle was significantly greater than the T1 angle. Rapid maxillary expansion did not modify the 3D ET parameters; only the right auditory tube angulation improved after expansion. The dentoskeletal indications for RME include a bilateral or unilateral crossbite, a cleft palate, and a maxillary deficiency. Maxillary expansion has been demonstrated to enhance respiration and the use of the nasal passage. Nasal structure enlargement reduces dehydration of the pharyngeal surface, infections of the upper respiratory region, and otitis media.6 A meta-analysis revealed that an increase of 1,218.3 mm3 in the volumetric upper airway is associated with RME.17 Cheung et al. evaluated the effects of upper airway volume produced by Hyrax, Hybrid-Hyrax and Keles keyless expanders.18 Maxillary expansion caused enhancement in total airway volume in the Hybrid-Hyrax group (+5,902.1 mm3) and a smaller rise in the Hyrax group (+2,537.9 mm3) or the Keles group (+3,001.4 mm3). Small increases in total upper airway volume were observed after RME.18 Echarri-Nicolás et al. compared upper airway modifications in cases undergoing treatment with different methods of microimplant-assisted expansion.19 A significant increase in total area and minimal section at the level of nasopharynx and oropharynx was observed in cases receiving bone-anchored maxillary expansion. An umbrella review has presented important increases in the nasal and oropharyngeal space volumes of growing children and adolescents after RME at 3-, 6- and 12-month follow-ups.20 Shetty et al. reported notable differences in the soft tissue parameter after mini-implant assisted rapid palatal expansion.21 Aljawad et al. emphasized that RME causes an increase in upper airway volume.22
A study by Braun demonstrated that a narrow maxilla induced oral breathing and impaired nasal respiration, thus affecting the ET and middle ear.23 Several studies have revealed that maxillary expansion can modify the anatomical structures of the pharynx and palate, thereby allowing the ostium tuba auditiva to function more efficiently by equalizing the pressures on both regions of the tympanic membrane.4 The tensor veli palatini muscle extends from the entrance of the ET to the soft palate. After RME, the muscle may enlarge to expand the ET orifice.24 To the best of our knowledge, this is the first study to use ultra-low-dose CBCT to examine the effects of RME on the detailed angular and linear parameters of the right and left ETs.
Dinç et al. compared the ET angle and length in healthy subjects and those with otitis media. The ET angles in healthy individuals were 23.0° in females and 24.3° in males.25 The Frankfort horizontal plane was used when measuring ET angles. The angles in our study were slightly lower. In other studies, the mean ET angles with the horizontal palatal plane averaged 34–36° in adults.26, 27, 28 In adolescents, the ET angle with the Frankfort horizontal plane was approx. 22°. The difference may reflect age-related changes and the use of reference planes. The ET angle remained constant after RME on both sides. No prior study has measured the effect of RME on 3D ET angles. Therefore, there was no basis for comparison. We expected that any changes would be similar; symmetrical RME was applied to the mid-palatal suture. No differences in right and left ET length were observed between T0 and T1 (right: 36.26 ±3.10 mm at T0 and 36.13 ±3.08 mm at T1, left: 36.82 ±2.98 mm at T0 and 36.82 ±3.12 mm at T1; p = 0.513 and p = 0.978, respectively). Using two-dimensional images, Bluestone et al. found that the ET length increased as children grew, attaining a final size of 31–38 mm at approx. 7 years of age.12 Takasaki et al. used conventional CT to compare the ET length between children and adults; the ET length in children was 38 mm and 43 mm in adults.28 The CBCT data obtained in the current study was slightly different, presumably due to the imaging modalities. Ha et al. noted that the ET lengths revealed by conventional CT and CBCT differed due to subjects’ positioning, whether in a supine or seated posture.29 Ultra-low-dose CBCT has been demonstrated to optimally detect morphological structures and is associated with reduced radiation, sharper imaging and briefer viewing than CT. Many studies have shown that RME consistently reduces conductive hearing loss and improves ET function in adolescents with maxillary transversal constriction.30 However, the present study found no significant effect of maxillary expansion on the ET length. There are 2 possible explanations for this state of affairs. Other studies have collected audiometric or tympanometric data; however, these studies did not include 3D CBCT linear and angular measurements. Secondly, RME inhibits the infection of the nasal and pharyngeal airways, which may contribute to a reduction in the incidence of otitis. Maxillary expansion improves conductive hearing loss and reduces the incidence of otitis media.
Duman et al. used an identical CBCT protocol to determine the auditory angle, which was significantly larger in patients with cleft lip and palate than in normal individuals; such patients often exhibit a severe maxillary transversal deficiency.31 We also found that the right auditory tube angle was larger before RME in patients with maxillary constrictions. The effects of RME on Eustachian and auditory CBCT data require further research. Longitudinal studies would be instrumental in defining the effect of RME in patients without adenoidal or other nasopharyngeal disorders. The retrospective nature of the study constitutes a limitation, as it relied on a limited set of patient data. Additionally, the absence of auditory tests comparing measurements to patient data further restricts the study’s conclusions.
Conclusions
Cone-beam computed tomography can yield morphological, angular and linear data on the ET and auditory structures. No significant differences were observed in linear or angular ET parameters based on maxillary expansion treatment status. The right auditory tube angle differed significantly between T0 and T1. Future studies should be conducted on larger populations and designed to compare measurements.
Ethics approval and consent to participate
The clinical research protocol was reviewed and approved by the Clinical Research Ethics Board of Eskisehir Osmangazi University, Turkey (approval No. 2018-58). Informed consent was obtained from all subjects and/or their legal guardian(s).
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.