Abstract
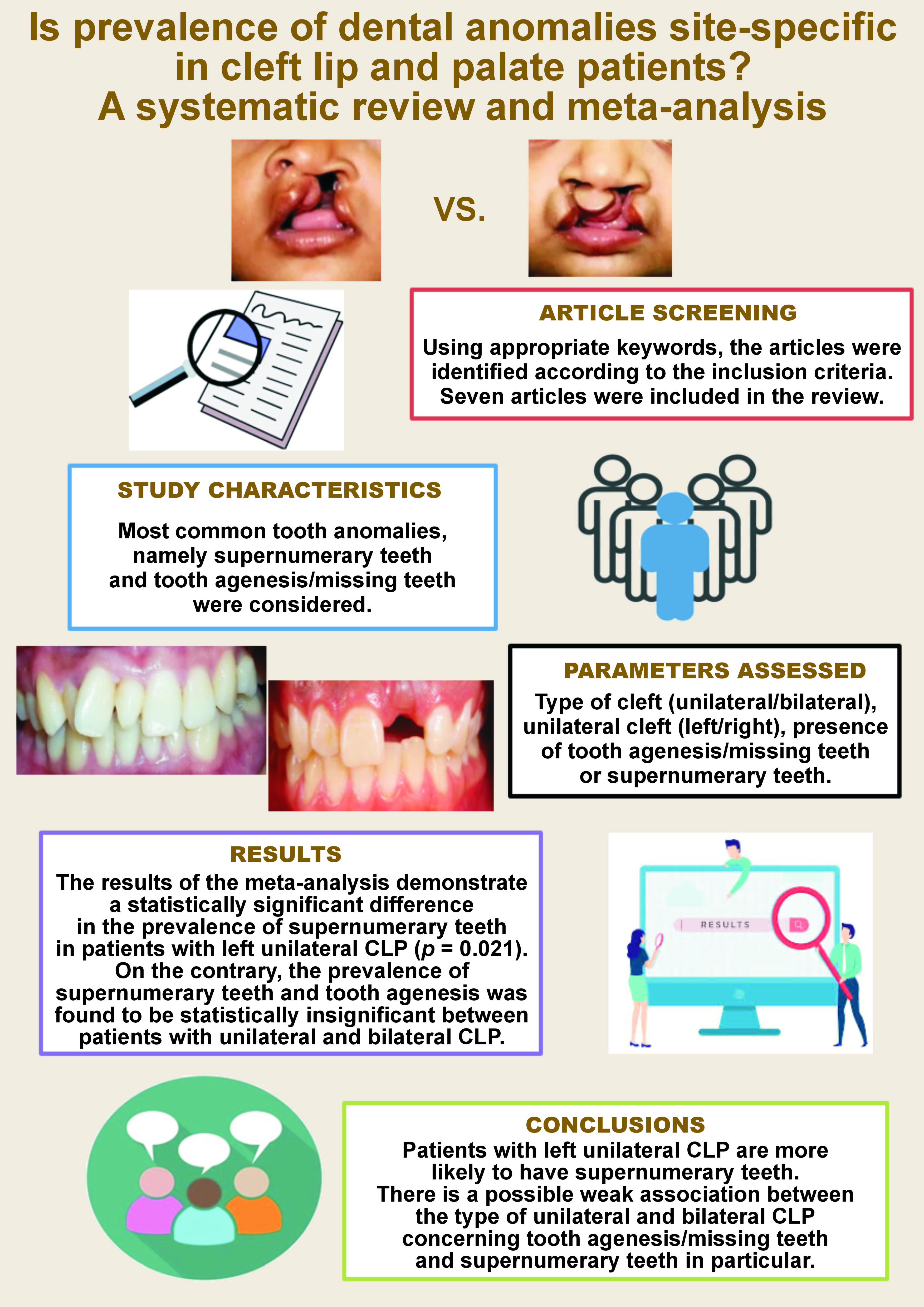
The prevalence of cleft lip in conjunction with cleft palate is twice that of cleft lip or palate alone. Dental abnormalities are more frequent in patients with cleft lip and palate (CLP) than in non-cleft individuals. The present systematic review aimed to identify studies that examined the prevalence of dental anomalies in unilateral and bilateral clefts. Relevant articles that met the specified inclusion criteria were identified with the use of MEDLINE/PubMed®, Scopus and EBSCOhost databases. The systematic review protocol was formulated using the established PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist. The results of the meta-analysis demonstrated a statistically significant difference in the prevalence of supernumerary teeth (ST) in patients with left unilateral CLP (p = 0.021). The difference was statistically insignificant for ST between unilateral and bilateral CLP (p = 0.542). The present analysis demonstrated that the difference between unilateral and bilateral CLP, as well as between right and left unilateral CLP regarding tooth agenesis/missing teeth (A/MT) was statistically insignificant (p = 0.301 and p = 0.130, respectively). However, the black diamond presented in the forest plot indicates that the unilateral CLP and left unilateral CLP groups are in favor, respectively. Consequently, patients with left unilateral CLP exhibited a higher frequency of ST. The analysis suggests a potential association between the type of unilateral CLP and bilateral CLP concerning A/MT and ST in particular.
Keywords: supernumerary teeth, cleft lip, cleft palate, congenital abnormalities
Introduction
A common congenital abnormality that manifests in approx. 1 in 700 live births is cleft lip and palate (CLP).1 The prevalence of cleft lip in conjunction with cleft palate is twice that of cleft lip or palate alone. These malformations involve the alteration of the middle third of the face, with varying degrees of severity. They may occur in isolation, particularly in non-syndromic patients, or they can be part of a group of abnormalities seen in syndromic cases.2
Developmental factors such as chromosomal abnormalities and gene mutations, as well as environmental factors, including maternal drug use, folic acid deficiency and radiation are concomitant to the etiology of cleft development.3, 4, 5, 6 However, the prevalence of CLP varies according to the type of population, race and geographical area.7, 8, 9
Dental abnormalities are more prevalent in patients with CLP than in non-cleft individuals, which may be a consequence of the cleft itself or any surgical intervention.10 Additionally, the relationship between dental abnormalities and CLP is influenced by proximal anatomy, cleft formation time and dental development.9, 11 Dental anomalies in CLP patients are predominantly observed in the anterior maxilla, suggesting a potential correlation with surgical interventions performed in this region during tooth bud formation. It is believed that both the embryological cleft formation and surgical procedures may cause dental anomalies in the structure and position of the teeth.12, 13
From an anatomical location and in terms of timing, the development of tooth germs and the formation of the oral clefts are associated embryologically with the construction of the teeth, lips and palate.14, 15 In comparison to the general population, individuals with oral clefts are more susceptible to dental variations.8, 16, 17 The disruptions and alterations during the development of teeth at various stages, including morphodifferentiation and histodifferentiation, may result in the formation of supernumerary teeth (ST), which may emerge from the dental lamina as a discrete entity or from the dichotomy of a tooth bud.18, 19 The most common dental defect in the cleft region is agenesis of maxillary lateral incisors, which is presumably due to the local impact of the cleft.14, 20, 21 The frequent absence of lateral incisors or their distal or mesial location concerning the cleft, as well as the presence of ST in the same region, may be attributed to the presence of CLP.22 The second most frequent dental defect is the presence of ST.22, 23
This systematic review aimed to identify studies that assess the prevalence of dental anomalies in unilateral and bilateral clefts. The review focuses on the prevalence of the most common anomalies, such as tooth agenesis/missing teeth (A/MT) and ST, in patients with unilateral and bilateral CLP, as well as between right and left unilateral CLP. This investigation also examines the existence of any quantitative differences among these groups.
Material and methods
The protocol of this systematic review was formulated using the established PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) checklist.24 The review question was designed utilizing the PICO framework, as follows:
– Population: non-syndromic unilateral and bilateral CLP patients with A/MT or ST;
– Intervention: presence of A/MT or ST;
– Comparison: dental anomalies between unilateral and bilateral CLP patients and between right and left unilateral CLP patients;
– Outcome: prevalence of dental anomalies between unilateral and bilateral CLP patients and between right and left unilateral CLP patients.
The formulated research question sought to ascertain whether dental anomalies are more prevalent in patients with bilateral CLP or unilateral CLP. The review protocol was registered in PROSPERO (registration No. CRD42022346399).
Eligibility criteria
Strict inclusion criteria were established to identify relevant articles from the database. The identification and filtration of articles was performed by 2 examiners (JW and SS). The full texts of relevant articles were obtained and independently screened by both reviewers. Only studies that considered and segregated data for unilateral as well as bilateral CLP were taken into consideration. This was done to compare the prevalence of anomalies strictly between unilateral and bilateral CLP. The inclusion criteria encompassed studies that described different types of clefts, with cross-sectional or prevalence-based study design, and non-syndromic unilateral and bilateral CLP study sample with A/MT or ST. The anomaly data was to be given individually for right and left unilateral CLP patients. Additionally, data for unilateral and bilateral CLP patients must have been presented in the form of total anomalies for specific cleft categories (discrete data). The selection of articles was constrained to those written in English, and the scope included any dentition (permanent/primary). The focus was exclusively on dental anomalies, and the specific types of anomalies must have been clearly specified. The exclusion criteria encompassed studies that did not describe the type of cleft, those that involved syndromic unilateral and bilateral CLP patients, and studies that did not categorize data and present it as cleft and non-cleft groups. Additionally, data that was not provided individually for right and left unilateral CLP patients, or for unilateral and bilateral CLP patients, was excluded. Studies that considered more than 1 anomaly in an individual but included them as a single entity, studies in which the number of events (anomalies) exceeded the total population, as well as case reports, letters, short communications, case series, and views, were excluded. Articles in any language other than English were not considered for inclusion.
Outcome assessed
The prevalence of dental anomalies was assessed between unilateral and bilateral CLP patients and between right and left unilateral CLP subjects.
Information sources and search
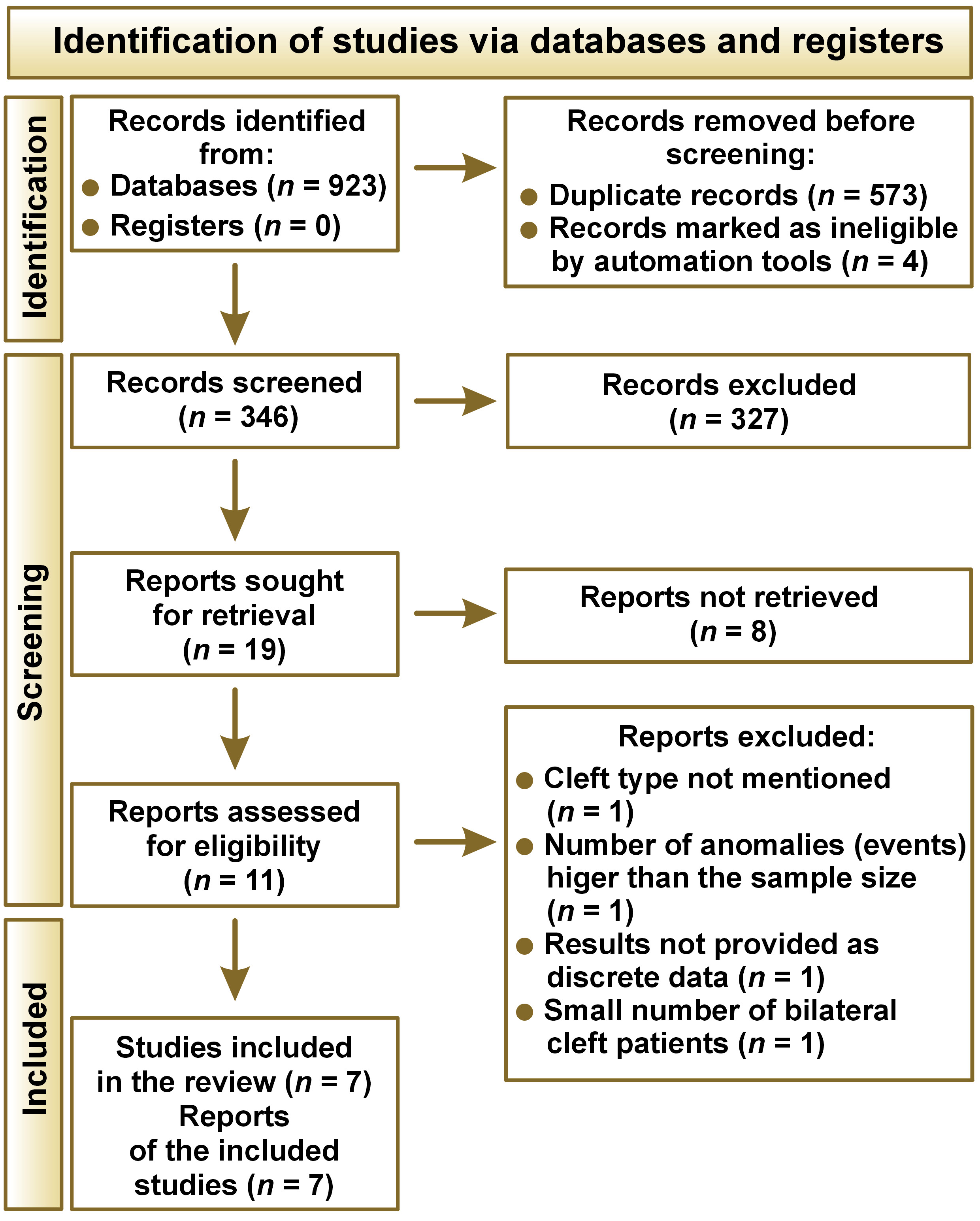
A comprehensive search was conducted using MEDLINE/PubMed®, Scopus and EBSCOhost databases to identify relevant articles that met the specified inclusion criteria. Additionally, a manual search was carried out to identify relevant articles from the gray literature. The search was implemented by 2 examiners (JW and SS) in October 2022. The medical subject headings (MeSH) were paired with “AND” and “OR” to establish a search strategy. The search strategies and the databases are delineated in Table 1. Titles and abstracts were initially screened against the inclusion and exclusion criteria, and the full texts were independently obtained and evaluated during a second screening by 2 researchers (JW and SS). Any discrepancies were resolved by the third researcher (AG). Figure 1 depicts a flowchart of the process of selecting studies for inclusion.
Data collection
The data was extracted from the included studies by 2 reviewers independently (JW and SS) under the following headings: author and publication year; types of anomalies; age group; types of clefts; results; and conclusions (Table 2). A modified version of the Newcastle–Ottawa Scale (NOS) was applied to evaluate the risk of bias.25
Quality assessment
The modified version of NOS was applied to assess the quality of cross-sectional studies for the systematic review, specifically cohort studies (Table 3).25, 26 Each study that met the established criteria was classified as very good, good, satisfactory, or unsatisfactory, based on the number of stars received. In the present analysis, 3 studies were qualified as satisfactory, and the remaining 4 were rated as good.
Synthesis of findings
The results of the studies were tabulated, and a meta-analysis was performed using RevMan 5.3 software (https://test-training.cochrane.org/online-learning/core-software-cochrane-reviews/review-manager-revman/download-revman-5), which synthesized the mean (M) and standard deviation (SD) values and depicted the results in the form of a forest plot. Statistics from 7 studies were analyzed, and the data was obtained, depending on the characteristic of effect size. For each study, discrete data was utilized to calculate the random risk ratio with the Mantel–Haenszel method. The heterogeneity of the included studies was investigated by inspecting study characteristics and using the I2 statistic in cases where sufficiently similar studies were analyzed. As the measuring scale in all the included studies was different, the meta-analysis utilized the mean difference as the effect size. The calculations involved the division of the mean difference in each study by that study’s SD to create an index (standardized mean difference). This index was found to be constant among studies. A funnel plot of studies with continuous data was plotted to assess publication bias for both dental anomalies (agenesis and ST between unilateral and bilateral CLP and for right and left unilateral CLP).
A meta-analysis was also performed to ascertain the prevalence of dental anomalies in patients with unilateral and bilateral clefts. The forest plot illustrated that the standard mean difference obtained for the prevalence of dental anomalies with unilateral and bilateral clefts as a whole was 1.23 (95% CI: 1.04–1.46). Patients with unilateral clefts demonstrated a higher prevalence of dental anomalies compared to those with bilateral clefts, with a p-value of 0.021 and low statistical heterogeneity (I2 = 0%), which may be attributed to the fact that the included studies were conducted in a similar manner, with minimal variation in study design.
Results
The search database yielded a total of 923 articles (Figure 1). Duplicate studies and studies marked as ineligible by automation tools were removed and abstracts of the remaining 346 articles were screened. Of these, the full texts of 11 articles underwent screening. Seven articles fulfilled the inclusion criteria and were included in the present analysis. Four studies were excluded from the analysis due to the following reasons: the cleft type was not mentioned in the data; the number of anomalies (events) was higher than the sample size27; the results were not given as discrete data28; and there was a small number of bilateral cleft patients, which may have introduced bias.17
A random-effects meta-analysis was conducted to generate an overview of the difference between dental anomalies among patients with unilateral or bilateral CLP. Since the studies involved different populations across the globe, the random-effects meta-analysis was employed to account for the variance in the prevalence of caries. For a study to be included in the meta-analysis, it was required to provide information regarding sample size and discrete data for each group, along with either SD, standard error (SE), standard error of difference, or p-value. The meta-analysis was conducted using RevMan 5.3 software. The analysis involved studies that compared patients with unilateral and bilateral CLP in terms of commonly associated dental anomalies, namely A/MT and ST.
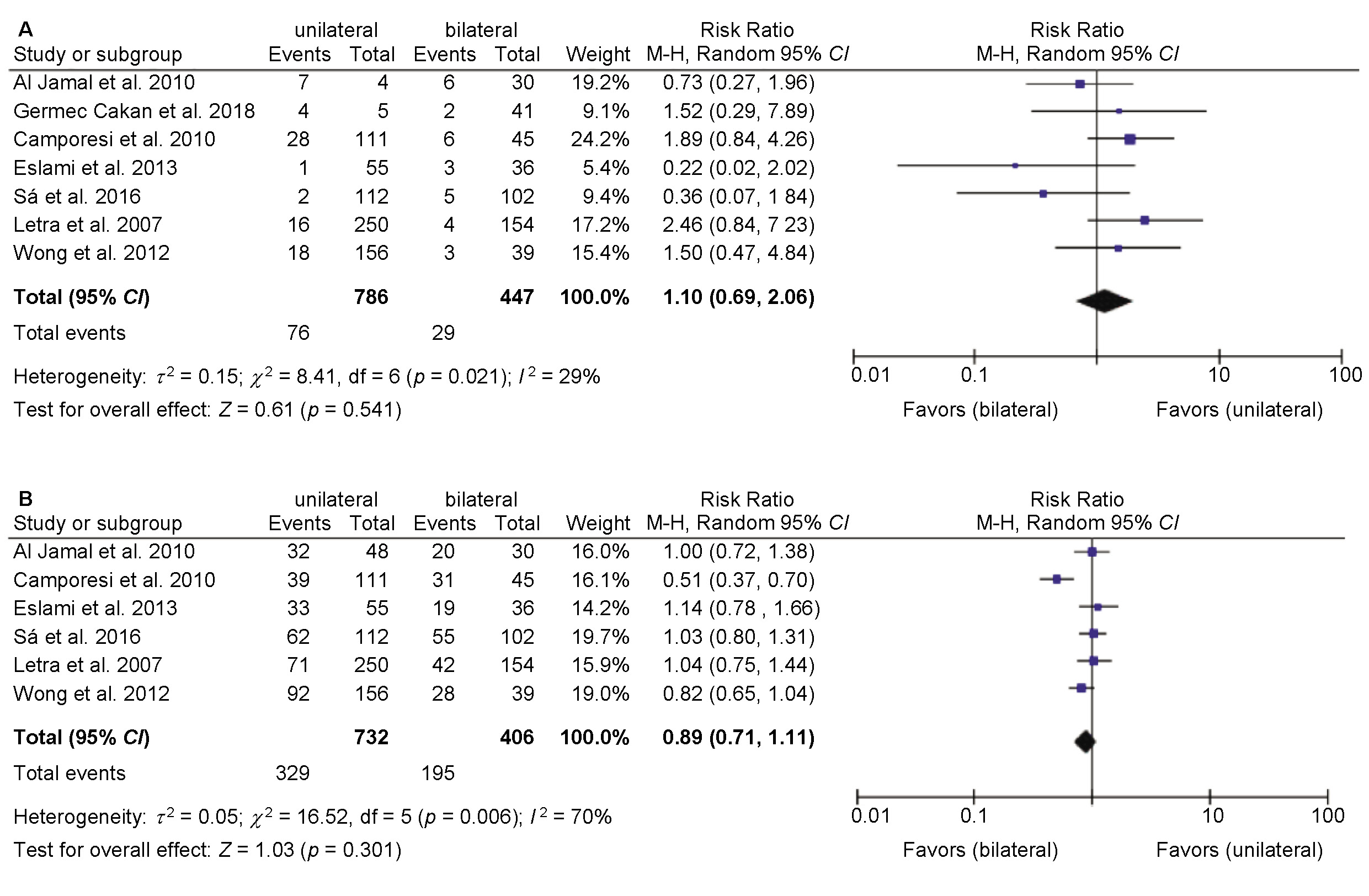
The sample size of individuals with ST in unilateral CLP was 786, and in bilateral CLP, it was 447. For agenesis, the sample size for unilateral CLP was 732 and 406 for bilateral CLP. The number of patients with ST and agenesis in left and right unilateral CLP was 39 and 196, respectively. The forest plot illustration of the random-effects meta-analysis of the included studies for ST and A/MT in patients with unilateral and bilateral CLP is presented in Figure 2. The current analysis revealed the standard mean difference of 1.10 (95% confidence interval (CI): 0.69–2.06) for ST in patients with unilateral and bilateral CLP, and 0.89 (95% CI: 0.71–1.11) for A/MT in unilateral and bilateral CLP. The variation was statistically insignificant for the prevalence of ST in unilateral and bilateral CLP, as indicated by a p-value of 0.541, and there was low statistical heterogeneity among the included studies (I2 = 29%, p > 0.05). The difference was also statistically insignificant in unilateral and bilateral CLP patients with A/MT, with a p-value of 0.301 and high statistical heterogeneity among the included studies (I2 = 70%, p = 0.006).
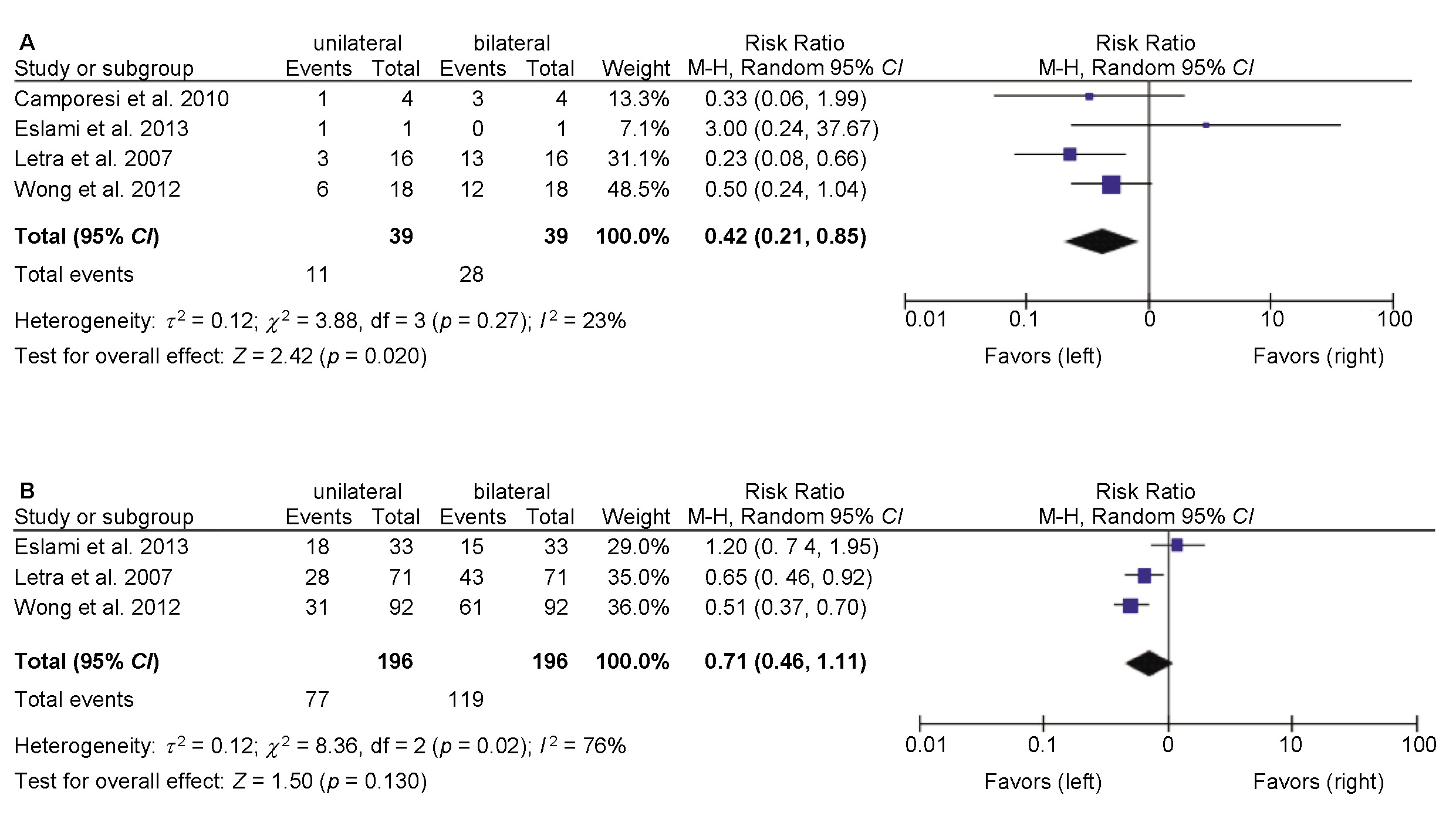
The forest plot illustration of the random-effects meta-analysis of the included studies for ST and A/MT in patients with left and right unilateral CLP is presented in Figure 3. In the current analysis, the standard mean difference obtained for ST in patients with left and right unilateral CLP was 0.42 (95% CI: 0.21–0.85), and for A/MT in patients with left and right unilateral CLP, it was 0.71 (95% CI: 0.46–1.11). The variation was statistically significant for the prevalence of ST in patients with left or right unilateral CLP, with a p-value of 0.020, favoring left unilateral CLP. Low statistical heterogeneity was reported among the included studies, with I2 = 23% (p > 0.05). On the other hand, the difference was statistically insignificant for the prevalence of A/MT in patients with left and right unilateral CLP, with a p-value of 0.130 and high statistical heterogeneity among the included studies (I2 = 76%, p < 0.05).
The results of the meta-analysis indicate that patients with left unilateral CLP have a higher prevalence of ST. On the contrary, the prevalence of A/MT was found to be statistically insignificant between patients with right and left unilateral CLP (p > 0.05). The quantitative analysis for A/MT and ST in unilateral and bilateral CLP patients yielded statistically insignificant results (p > 0.05).
Discussion
The current review quantitatively analyzed the available literature to ascertain whether the prevalence of dental anomalies (A/MT and ST) is higher in patients with CLP. To the best of our knowledge, no review has explored the relationship between the occurrence of dental anomalies in unilateral and bilateral CLP patients and also between patients with right and left unilateral CLP. The results of the current meta-analysis demonstrate a statistically significant difference in the prevalence of ST in patients with left unilateral CLP (p = 0.020). These outcomes are similar to the results of previous studies.9, 29 On the other hand, the difference was statistically insignificant for ST in unilateral and bilateral CLP (p = 0.541). To date, the literature has proposed 2 types of hypotheses regarding the occurrence of ST in cleft patients. The first suggests that the odontogenic region of the lateral incisor originates from the medial nasal and maxillary processes, and that the non-fusion of these 2 processes results in 2 separate lateral incisors.15, 22 The other hypothesis suggests that ST arise from post-fusion rupture of the cleft in the lateral incisor area, and the tooth germ of the lateral incisor is separated into 2 teeth.15, 30
The analysis of A/MT between unilateral and bilateral CLP patients, as well as between right and left unilateral CLP individuals, yielded statistically insignificant values (p = 0.301 and p = 0.130, respectively). However, the black diamond in the forest plot indicates that the bilateral CLP and left unilateral CLP groups are in favor, respectively. A high level of heterogeneity was observed in studies involving agenesis, indicating potential differences in study design, population type, age group, and surgical interventions across the included studies, with I2 of 70% for unilateral and bilateral CLP, and 76% for right and left unilateral CLP. The studies that examined the prevalence of ST were similar in respect to the abovementioned attributes and reported a low level of heterogeneity, with I2 values of 29% for unilateral and bilateral CLP and 23% for left and right unilateral CLP. Further clinical trials are necessary to reach a conclusive result.
Several theories have been advanced to explain the presence of dental agenesis in the vicinity of the affected region. These theories include low blood supply due to congenital conditions or surgery, low ectomesenchymal supply, and the osseous deficiency resulting from the cleft.10, 20, 22 Sá et al. reported that lateral incisors are the most affected teeth and are more prevalent in individuals with unilateral complete CLP.15 However, these findings differ from the results of the conducted meta-analysis. In the 12th month following birth, the permanent maxillary lateral incisors begin to calcify. Thus, the presence or absence of ST, microdontia, or malformation of lateral incisors may be attributed to the presence of a cleft, the intraoral environment generated by the cleft, and a lack of mesenchymal tissue. Letra et al. stated that the absence of the left or right lateral incisor was significantly associated with unilateral right or left clefts, respectively.16 Research has indicated that genetic factors may contribute to the development of CLP and dental anomalies.8, 31, 32 Furthermore, human studies revealed an association between genetic variations in MSX1 and PAX9 genes and tooth agenesis within and outside the cleft area.31, 33
Marzouk et al. conducted a systematic review to determine whether individuals with non-syndromic orofacial clefts (OFCs) demonstrated an increased prevalence of dental abnormalities in comparison to those without OFCs.34 The results indicated that individuals with OFCs are more likely to present with a range of dental abnormalities compared to their unaffected peers. Statistically significant associations were observed between OFCs and ST, developmental enamel defects, malposition and/or transposition, rotation, and impaction.34
Dental abnormalities manifest at a higher frequency among individuals with cleft palates compared to the general population. The observed differences in the prevalence of these abnormalities across studies can be attributed to ethnic variations, the diversity of the sample, or the severity of the cleft phenotype. However, a definitive conclusion has not been reached. In this analysis, the relationship between gender, cleft type and dental anomalies was not considered, as previous studies demonstrated no correlation between these variables.23, 29, 31, 34, 35 Local factors, such as the cleft itself, and primary surgical procedures have been proposed as contributors in the development of dental anomalies. However, a conclusive statement regarding the involvement of surgical procedures in influencing the development of anomalies in cleft patients could not be discussed at length, as the same factor was not considered in the included studies.36, 37 Additionally, although bilateral CLP is less common in the general population, the condition should be considered when conducting clinical studies in the future.
Limitations
The study was subject to several limitations. Firstly, the population group and the type of dentition were heterogeneous, which may have affected the outcome, as the occurrence of dental anomalies may be more pronounced in a particular type of population. Secondly, the results of the review were not categorized by age or gender. Additionally, the oral hygiene practices adopted by patients with clefts are unclear. There is a need for randomized controlled trials based on patients with unilateral and bilateral CLP. Lastly, it was not specified whether the anomalies had been counted before or after the surgical intervention for the correction of CLP.
Conclusions
The present analysis demonstrated that patients with left unilateral CLP are more susceptible to being associated with the presence of ST. There is a possible weak association between the type of unilateral and bilateral CLP concerning A/MT and ST in particular. However, in vivo studies with a similar study design and overall minimal heterogeneity are necessary to reach a definitive conclusion.
Trial registration
The review protocol was registered with PROSPERO (identification No. CRD42022346399).
Ethics approval and consent to participate
Not applicable.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.
Use of AI and AI-assisted technologies
Not applicable.