Abstract
Background. The ability to predict the extent and direction of horizontal growth of the patient’s face at an early age allows clinicians to timely identify cases that require treatment during the growth period and to ensure that appropriate treatment can be administered.
Objectives. The aim of this study was to investigate the role of the antegonial angle, gonial angle, antegonial notch depth, and the type of the antegonial notch on predicting horizontal facial growth in individuals with normal facial height.
Material and methods. In this descriptive analytic study, lateral and panoramic radiographs of 180 patients aged 17–30 years with normal facial height who were referred to the School of Dentistry of Qazvin University of Medical Sciences and private dental clinics were investigated. The indices of the gonial angle, antegonial angle, type of antegonial notch, and antegonial notch depth were plotted bilaterally on tracing paper and subsequently measured using panoramic radiographs. Additionally, the relationship between the desired radiomorphometric indices and the occlusion class in the samples was investigated.
Results. There was a statistically significant relationship between the occlusion class and the antegonial notch depth (analysis of variance (ANOVA), p = 0.048), as well as the antegonial angle (Kruskal–Wallis test, p = 0.002).
Conclusions. The results of this study indicate that the antegonial notch depth and angle indices can be clinically valuable in predicting the process of mandibular growth and developing appropriate treatment plans.
Keywords: mandible, radiomorphometric index, skeletal relationship
Introduction
The variability of occlusion, which can range from a desired state to a severe malocclusion in different individuals, is attributed to the interplay of bone growth, dental development and neuromuscular maturation. A better understanding of the relationship between occlusion, dental development and skeletal structure will facilitate the orthodontic diagnosis.1 Orthodontists must be able to discern the relationship between the major functional facial parts, namely the cranial base, jaw and teeth.2 The correlation between occlusion and craniofacial skeletal structure is well established within the field of orthodontics.1, 3
A thorough diagnosis and treatment plan for malocclusions require a clear understanding of both the dentoalveolar and skeletal components in anterior–posterior and vertical directions.4
The capacity to predict a patient’s growth pattern is valuable for orthodontists, as it enables the implementation of corrective measures at critical time periods to address skeletal discrepancies and avoid or decrease the necessity for surgical or orthodontic treatment. The direction of the growth of the mandible can significantly affect a person’s occlusion, which in turn has an influence on their function and aesthetics. The type of facial growth is primarily determined based on radiographic imaging.5
Mandibular stimuli are present from the developmental stage to adulthood and can change the growth of the mandible and its bone remodeling.6 Some of the most notable changes that have been suggested include alterations in the antegonial, gonial, condylar, and ramus regions.7 Panoramic radiography is the preferred method in the assessment of mandibular morphology, including vertical and angular measurements.6
Panoramic radiography is a valuable tool for evaluating mandibular indices.8 Dental panoramic radiography is a reliable method for diagnosing and evaluating the mandibular position from the dentist’s perspective.9 The majority of authors who have conducted research into mandibular remodeling have performed morphometric evaluations using panoramic radiographs.7 The morphological changes of the mandible have been investigated mainly through the analysis of radiomorphometric measurements.6
Skieller et al. used multivariate statistical methods to identify 4 morphological variables that, when evaluated in lateral cephalograms, may predict future mandibular rotation. However, their sample included individuals with highly abnormal morphological patterns.10 Further research using this method conducted by Lee et al. and Leslie et al. did not yield promising results.11, 12 Halazonetis et al. discovered that the overall rotation of the mandible during growth was not related to the mandibular shape.13 However, the authors observed a correlation between the Fourier coefficient, which explained most of the variability in the ramus slope, and gonial and antegonial angles.13 Two studies examined the possibility that the mandibular antegonial notch morphology may predict the mandibular growth.14, 15
Given the paucity of studies in this field that have considered sample matching and the ongoing debate surrounding the study of gonial angle and antegonial notch area changes in mandibular growth, this study aimed to investigate the crucial role of the antegonial angle, gonial angle, antegonial notch depth, and the type of the antegonial notch in predicting horizontal facial growth in individuals with normal facial height.
Material and methods
This descriptive analytic study evaluated 180 individuals between the ages of 17 and 30 who were candidates for orthodontic treatment and referred to the School of Dentistry of Qazvin University of Medical Sciences and Qazvin private dental clinics between 2011 and 2016. The participants were divided into 3 groups of 60 individuals each, according to the occlusion class (Angle’s Class I, Class II and Class III occlusion).
The samples were selected from patients who had been referred to orthodontic clinics using simple random sampling and following the conclusion of a clinical study, based on established inclusion and exclusion criteria. The study included patients with normal facial height.
One of the criteria for evaluating and detecting the vertical facial growth pattern is the Jaraback index, which was calculated with the help of natural head position (NHP) cephalometric imaging using the following formula (Equation 1)16:
where:
S–Go – linear distance between Sella (S) and Gonion (Go) (posterior facial height) [mm];
N–Me – linear distance between Nasion (N) and Menton (Me) (anterior facial height) [mm].
The Jaraback index falls within the normal range of 62–65%.17
The exclusion criteria were as follows: a mismatch between the ANB and Wits indices in the patient; a discrepancy between the occlusion of the both sides of the patient; patients with mixed dentition; individuals with long or short faces; and individuals with retrusion or severe maxillary protrusion based on the cephalometric index.
All certified digital panoramic radiographs were attached to the parchment paper of the Ortho Organizer type. Tracing was performed by a trained senior-year student, while radiomorphometric indices were determined by a maxillofacial radiologist on digital panoramic radiographs.
The radiomorphologic and radiomorphometric indices evaluated in this study are as follows:
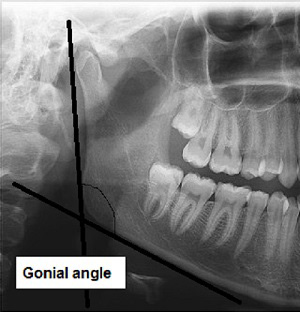
– gonial angle: a line is drawn tangent to the inferior border of the mandibular body, and another line is drawn tangent to the posterior border of the ramus and condyle. The intersection of these 2 lines forms the gonial angle (Figure 1)18;
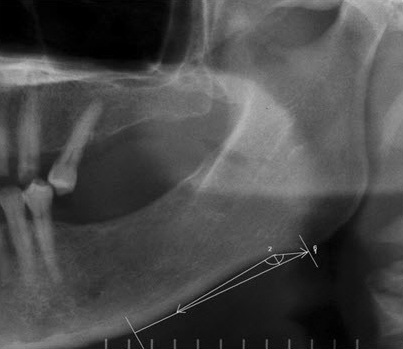
– antegonial angle: 2 lines are drawn tangent to the edge of the inferior border of the mandible that intersect each other at the deepest part of the antegonial notch. The angle between these 2 intersecting lines is referred to as the antegonial angle (Figure 2)19;
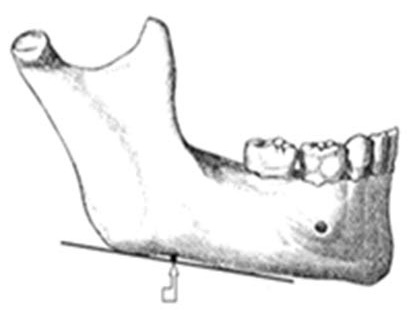
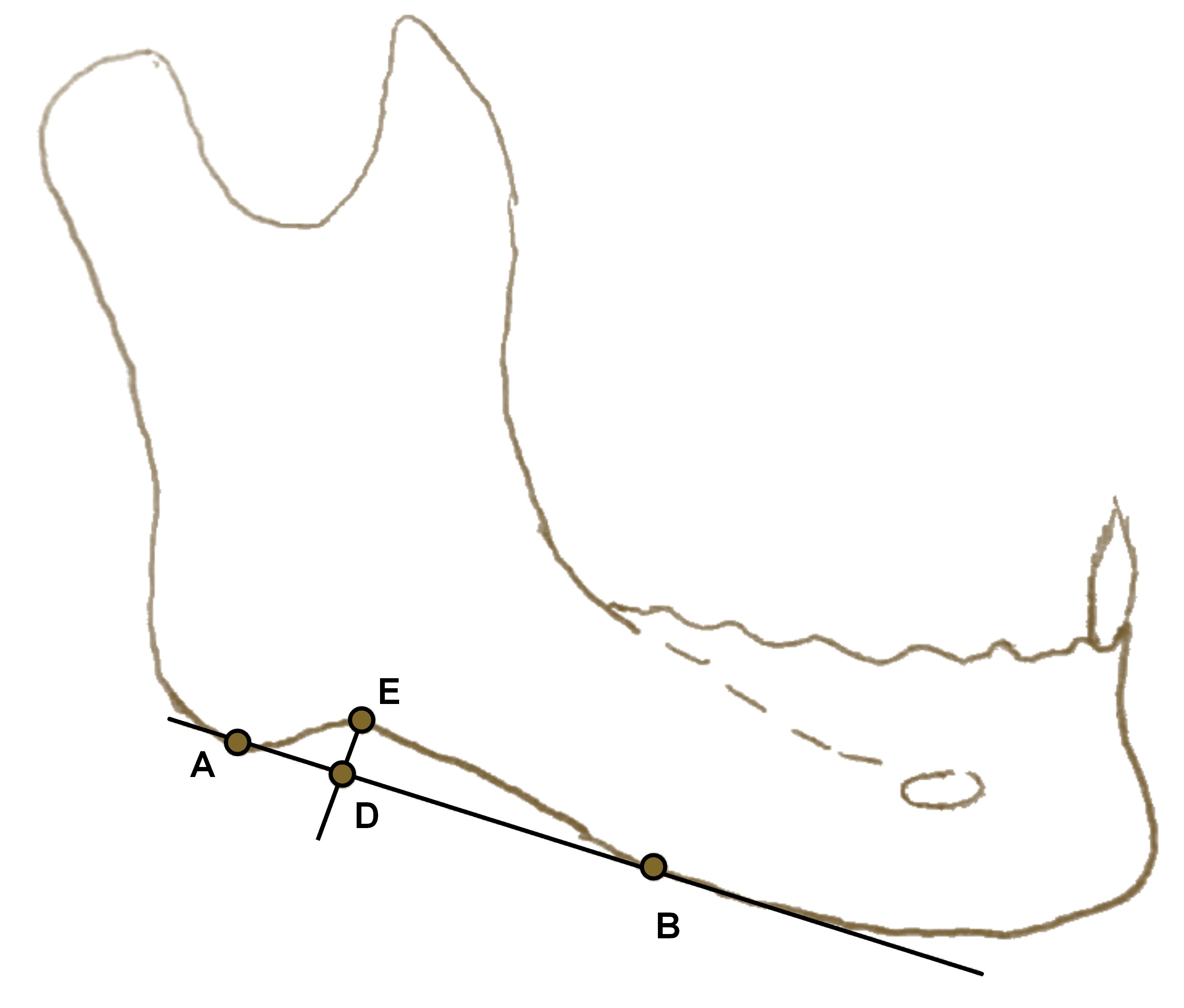
– antegonial notch depth: the distance of a perpendicular line from the deepest point of the antegonial notch concavity to a line tangent to the inferior border of the mandible (Figure 2, Figure 3, Figure 4)19;
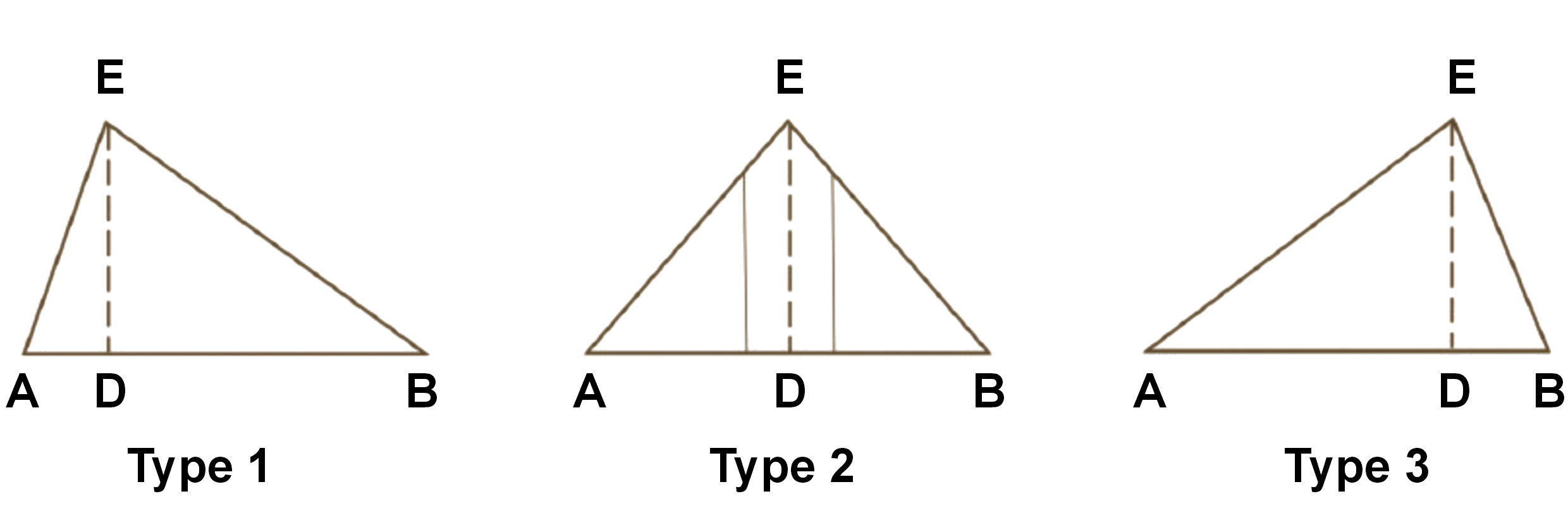
– type of antegonial notch: the triangular shape of the antegonial notch is drawn by connecting 3 points (A, B and E) (Figure 4); antegonial notch is classified into 3 types, including asymmetrical posterior notch (type 1), symmetrical notch (type 2), and asymmetrical anterior notch (type 3) (Figure 4,Figure 5).15
The antegonial notch depth was measured with the use of a digital caliper (Guanglu Instruments Co., Ltd., Guilin, China). The measurements included the gonial angle and the antegonial angle. The obtained data was recorded in the patient form. In instances where the indices were bilaterally visible, two-way measurements were performed and the mean values were recorded. In cases where the index was not visible on one side, only the index of the side that was clearly visible was used in the measurements.
Statistical analysis
The data was analyzed using analysis of variance (ANOVA), and Tukey’s post hoc test was employed to facilitate the comparison between the 3 groups. The χ2 test was utilized to investigate the relationship between qualitative traits. A paired t-test was employed to compare the left and right indices, while Wilcoxon test and the Kruskal–Wallis test were utilized to compare indices with a non-normal distribution. The data was analyzed using the IBM SPSS Statistics for Windows software, v. 20.0 (IBM Corp., Armonk, USA). In this study, a p-value of less than 0.05 was considered statistically significant.
Results
The present study was conducted on a total of 180 subjects aged 17–30 years, who were candidates for orthodontic treatment at the School of Dentistry of Qazvin University of Medical Sciences and Qazvin private dental clinics between 2011 and 2016. Of the total number of subjects, 47 (26.1%) were male and 133 (73.9%) were female. The results demonstrated no statistically significant relationship between sex and the occlusion class.
The mean and standard deviation of the right and left gonial angles were 123.0 ±6.7° and 123.1 ±7.9° for Class I, 124.1 ±5.8° and 122.9 ±6.5° for Class II, and 123.3 ±7.1° and 122.9 ±6.3° for Class III of occlusion. The statistical analysis revealed no statistically significant differences between the mean values of the gonial angle on both sides across the 3 occlusion classes (Table 1).
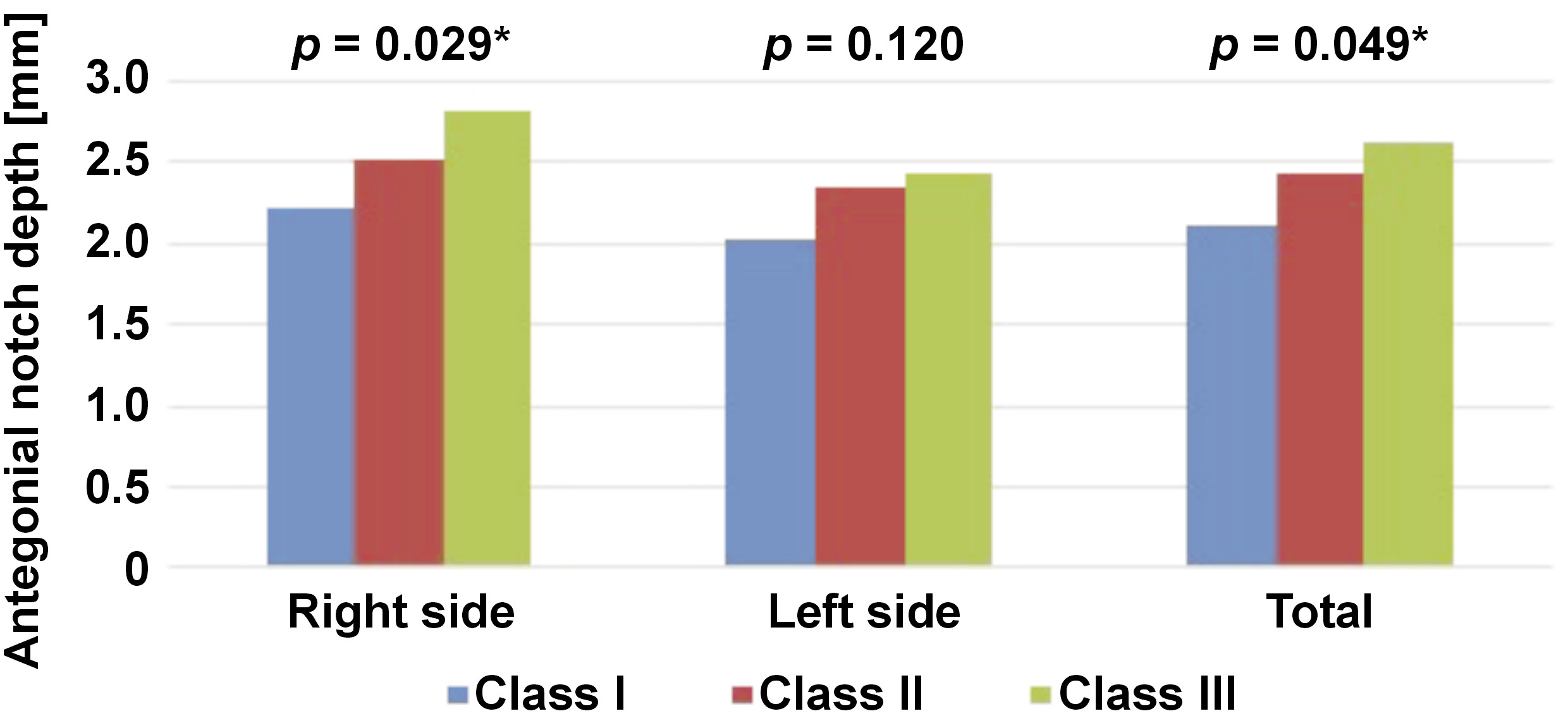
The results of the statistical analysis indicated a statistically significant difference in the mean value of the antegonial notch depth between the 3 occlusion classes on the right side and in the total sample (Figure 6).
The data revealed that in Class I, 1.7% of the antegonial notches were tangible, 28.3% were type 1, 45.0% were type 2, and 25.0% were type 3. In Class II, 2.5% of the antegonial notches were tangible, 29.2% were type 1, 50.8% were type 2, and 17.5% were type 3. In Class III, 0.8% of the antegonial notches were tangible, 26.7% were type 1, 42.5% were type 2, and 30.0% were type 3 (Table 2).
The statistical analysis demonstrated statistically significant differences between the right and left sides of the antegonial notch in 3 occlusion classes (p < 0.001) (Table 3).
The results of the statistical analysis revealed no statistically significant difference between the occlusion groups on the right side of the antegonial notch and in total. However, a statistically significant difference was observed between the 3 groups on the left side (p = 0.007) (Table 4).
In evaluating the antegonial angle across 3 occlusion groups, the median value of the left antegonial angle was observed to be greater than that of the right angle. However, no statistically significant difference was identified between the 2 sides (p > 0.001) (Table 5).
The statistical analysis revealed a statistically significant difference in the antegonial angle values between the 3 occlusion classes on the right (p = 0.002) and left sides (p = 0.040) of the body, as well as in the total sample (p = 0.002) (Table 6).
Discussion
The study investigated the relationship between 4 radiomorphometric indices, including the gonial angle, the antegonial angle, antegonial notch depth, and the type of antegonial notch. A statistically significant relationship was identified between the antegonial angle, antegonial notch depth and the occlusion class. There was no significant relationship between the gonial angle and the type of antegonial notch in relation to the occlusion class.
Dental panoramic radiography is a reliable method for diagnosing and evaluating the mandibular position from the dentist’s perspective.9 Since panoramic radiography is a routine procedure, it can be used effectively to evaluate mandibular indices.8
Some studies have reported a significant difference between individuals with very deep and those with very shallow antegonial notches with regard to mandibular growth indices.14, 20 Singer et al. performed a 4-year longitudinal study on 25 patients undergoing orthodontic treatment with a deep antegonial notch, along with a similar group with a shallow antegonial notch.14 They used lateral cephalometric radiographs and found that cases with a deep antegonial notch exhibited greater retrusion of the mandible, a shorter body length, a shorter ramus, and greater gonial angles than those with a shallow antegonial notch.14 During the study period, patients with a deeper antegonial notch demonstrated a smaller increase in the mandibular body length and less chin displacement in the horizontal direction (resulting in greater retrusion of the mandible) than subjects with a shallow antegonial notch. The results of this study indicate that the presence of a deep antegonial notch is associated with reduced mandibular growth potential and a distinct vertical growth pattern.14 Although the present study and the study by Singer et al.14 are consistent in terms of the orientation of the antegonial notch and its impact on mandibular growth, the pattern of mandibular growth differs. Based on the present study, cases with a higher antegonial angle and a deep antegonial notch are prone to mandibular protrusion. Moreover, no statistically significant difference was identified between the gonial angle and the occlusion class, in contrast to the findings of the study by Singer et al.14
The differences between the results of the present study and those of the study by Singer et al. include different sampling methods, different implementation methods, a low sample size, a lack of attention to maxillary horizontal growth, sample mismatch in terms of maxillary horizontal growth, and racial differences.14 The study sample employed by Singer et al. consisted of patients who had undergone orthodontic treatment, which represents a confounding factor in the study. Additionally, the subjects of the study were individuals with deep and shallow antegonial notches.
Lambrechts et al. investigated the craniofacial features in lateral cephalometric radiography of 40 patients with a shallow antegonial notch and 40 patients with a deep antegonial notch in order to evaluate different dimensions in craniofacial morphology between the 2 groups.20 Their findings indicated that, on average, subjects with a deep mandibular antegonial notch had a larger gonial angle, a deeper posterior ramus notch, and a steeper occlusal plane in examination than those with a shallow antegonial notch, whose mandible exhibited a more anterior position than subjects with a deep antegonial notch. The anterior face height of individuals with a shallow antegonial notch was significantly lower than the anterior face height of those with a deep antegonial notch. Also, the maxillary position in relation to the cranial base was more protruding in patients with a deep antegonial notch than in those with a shallow antegonial notch.20 While the present study and the study by Lambrechts et al. are consistent in terms of the efficacy of the antegonial notch in mandibular growth, the growth pattern of the mandible presented in the study by Lambrechts et al.20 is inconsistent with the results of our study. Also, in contrast to the findings of Lambrechts et al.,20 the present study did not identify a statistically significant relationship between the gonial angle and the occlusion class. This discrepancy can be attributed to different sampling methods, racial differences, different implementation techniques, a small sample size, a lack of attention to maxillary horizontal growth, and sample mismatch in terms of maxillary horizontal growth. Moreover, the study by Lambrechts et al.included individuals with deep and shallow antegonial notches, which is indicative of non-random sampling.20 Furthermore, previous studies14, 20 have not addressed the issue of vertical growth matching, which may be a confounding factor in the study.
The study by Ghosh et al. revealed no significant relationship between mean angles and the depth of the antegonial notch in relation to age.21 However, antegonial angles decreased with age, while the antegonial notch depth demonstrated an increase with age.21 The findings of our study are consistent with those of Dutra et al., who found no significant correlations between age and the antegonial angle and depth change.19 The results indicate that the 17–30 age range is not considered as a confounding factor in the study.
In the study by Ghosh et al., a comparison of the absolute values of the right and left antegonial angles revealed that the values on the left side were significantly higher than those on the right side in each group.21 This result is consistent with the findings of our study. It supports the theory that even in the absence of malformations and skull base asymmetry, the mandible may be physiologically asymmetric.
In the study by Ghosh et al., a significant decrease in the values of the antegonial angle and a significant increase in the values of the antegonial notch depth were observed as the dentition status changed from completely dentulous to partially dentulous and from partially dentulous to completely edentulous on both the right and left sides and in both sexes.21 Therefore, the dental position can be considered a confounding factor in the evaluation of the antegonial area. In the present study, all samples had at least 1 interdental position in each side of the jaw, thereby eliminating the confounding role of dental position as a variable.
In a longitudinal study conducted by Kolodziej et al., 40 subjects were examined in 3 age groups (8.5, 12 and >17 years) with no history of treatment.22 The study concluded that the antegonial notch depth was not a reliable indicator for investigating the potential of facial growth.22 This result is inconsistent with the findings of our study. The discrepancy between the 2 studies may be attributed to the long-term nature of the study conducted by Kolodziej et al., a small sample size, the use of different implementation methods, racial differences, inadequate consideration of maxillary horizontal growth, and sample mismatch in terms of maxillary horizontal growth.22
Conclusions
In evaluating the indices, it was observed that changes based on the occlusion class, the antegonial angle and the type of antegonial notch were affected by the growth pattern in patients with normal facial height. Individuals with a deep antegonial notch and a greater antegonial angle were more prone to mandibular protrusion. Therefore, it is recommended that timely therapeutic measures be taken prior to the growth spurt in patients with a deeper antegonial notch and a wider angle in order to control the growth of the mandible. However, further research is required to determine a suitable cut-off point for these indices.
Ethics approval and consent to participate
The study protocol was approved by the Ethics Committee of Qazvin University of Medical Sciences (approval No. IR.QUMS.REC.1395.292).
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.