Abstract
Background. Pit and fissure sealants are the most commonly used preventive measure against caries in permanent molars. Advancements in dental materials have led to the development of hydrophilic sealants. However, their clinical efficacy must be evaluated and compared with that of conventional hydrophobic sealants.
Objectives. This study aimed to clinically evaluate and compare the retention, marginal adaptation and marginal discoloration of hydrophilic and hydrophobic pit and fissure sealants over a 12-month follow-up period.
Material and methods. The study was a split-mouth, double-blind, randomized controlled trial. A sample size calculation was performed, and 120 first permanent molars (60 in each group) were selected for inclusion in the study. According to the split-mouth design, the sample was randomly divided into 2 groups. Group A was treated with a hydrophilic sealant (UltraSeal® XT Hydro), while Group B was treated with a hydrophobic sealant (Conseal F). The sealants in both groups were applied in accordance with the manufacturer’s instructions by a single operator. The sealants were evaluated clinically using visual and tactile methods by 2 independent examiners who were blinded to the procedure in accordance with the modified United States Public Health Service (USPHS) clinical rating system at placement and at 1, 3, 6, and 12 months.
Results. After 12 months of follow-up, the Conseal F sealant showed significantly better retention (p = 0.001), marginal adaptation (p = 0.023) and reduced marginal discoloration (p = 0.004) in comparison to the UltraSeal XT Hydro sealant.
Conclusions. The Conseal F (hydrophobic) sealant demonstrated superior retention, marginal adaptation and marginal discoloration compared to the UltraSeal XT Hydro (hydrophilic) sealant.
Keywords: first permanent molars, Conseal F, resin-based sealant, UltraSeal XT Hydro
Introduction
The occlusal surfaces of posterior teeth are highly susceptible to caries due to bacterial accumulations being confined within the complex morphology of pits and fissures.1 The prevalence of caries on the occlusal surfaces of molars in children aged 5–17 years has been reported to range from 67% to 90%.2, 3
One of the most effective methods for preventing caries in pits and fissures is the application of pit and fissure sealants.4 These materials are introduced into the occlusal pits and fissures of caries-susceptible teeth, forming a micromechanically bonded protective layer that blocks the access of caries-producing bacteria and their source of nutrients.5 Pit and fissure sealants offer several advantages, including a lower cost compared to restorations and a nine-fold reduction in caries occurrence compared to unsealed teeth.6
Resin-based filled and unfilled fluoridated sealants, incorporating fluoride as a caries-preventive ingredient, have been introduced. Their effectiveness is attributed to their retention because they penetrate the micropores of etched enamel surfaces. Resin-based sealants are considered effective in the prevention of caries due to their higher retention rates and proven cariostatic effects. However, their application is technique-sensitive and depends on the practitioner’s skill, the patient’s cooperation and the prevention of salivary contamination. Additionally, their hydrophobic nature makes them highly susceptible to moisture contamination.7
The recent introduction of hydrophilic sealants has the potential to reduce microleakage and enhance retention.8, 9 UltraSeal® XT Hydro is a moisture-tolerant resin-based sealant that is capable of bonding to slightly moist tooth structures, thereby creating an impervious interface. The oral cavity is a 100% humid environment where moisture control is difficult to achieve. In such conditions, the use of a moisture-tolerant sealant may be advantageous.10
The caries-preventive effect of pit and fissure sealants depends on their retention and marginal adaptation. Therefore, this study aimed to clinically evaluate and compare the retention, marginal adaptation and marginal discoloration of UltraSeal XT Hydro and Conseal F pit and fissure sealants.
Material and methods
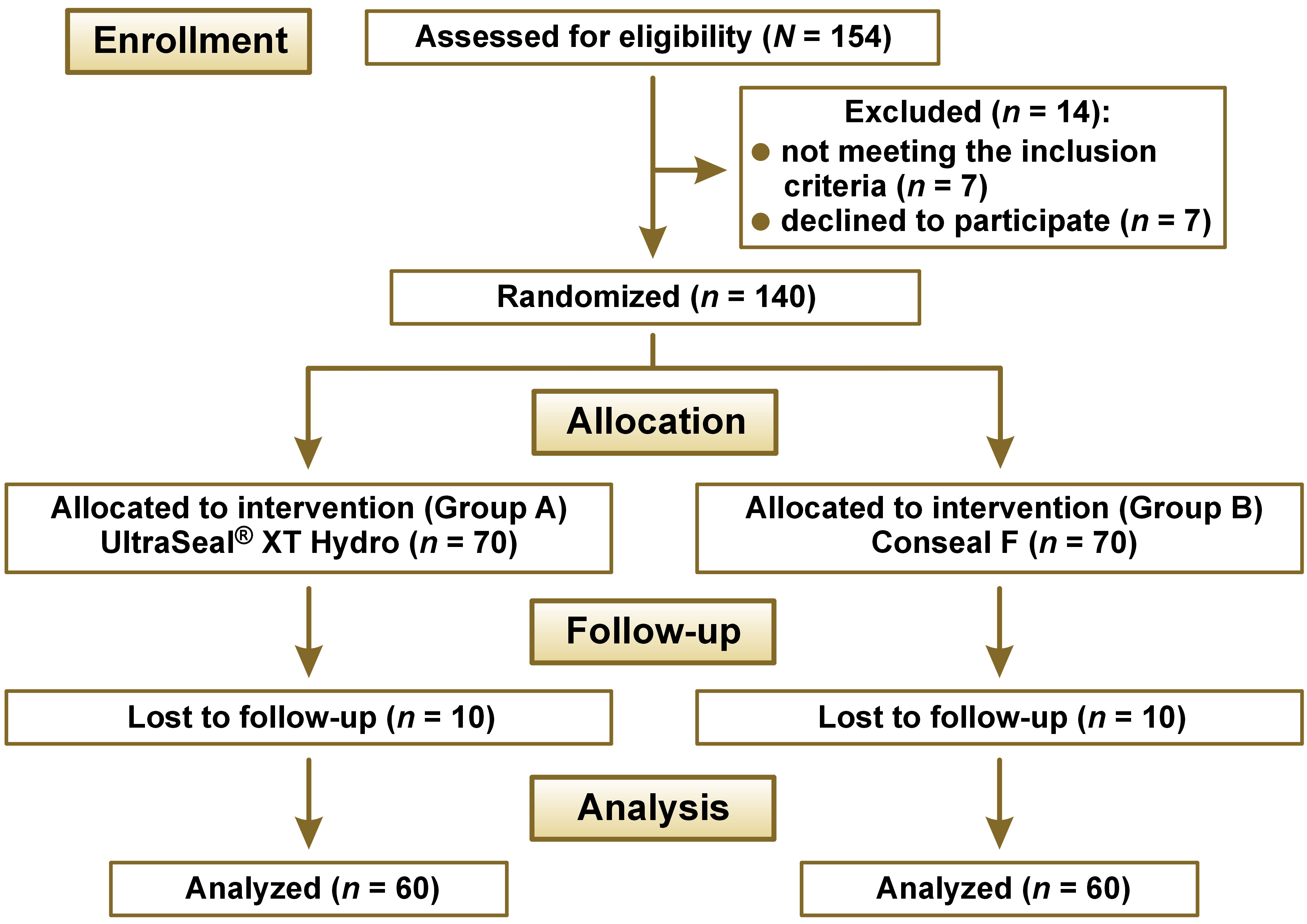
The study was conducted in the Department of Pediatric and Preventive Dentistry at Terna Dental College in Navi Mumbai, India. The ethical approval was obtained from the Institutional Review Board (reference No. TDC/IRB-EC/145/2017). The study was registered with the Clinical Trial Registry India under the code CTRI/2018/08/015206. The trial was conducted in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines (Figure 1).
Study design and sample size calculation
The study was designed as a split-mouth, double-blind, randomized controlled trial, ensuring that both patients and examiners were unaware of the sealants used. The sample size calculated per group was 60, with an alpha of 0.05 and a beta of less than 0.2 (power >80%). The assumed retention rate was 72% in Group A (hydrophilic sealant) and 50% in Group B (hydrophobic sealant). The proportion in Group A was assumed to be 0.5000 under the null hypothesis and 0.7200 under the alternative hypothesis.11 To account for potential dropouts, the sample size was increased by 15%, and the study was initiated with 140 sealants.
Patient selection and recruitment
Prior to the procedure, the parents provided written informed consent. Both children and parents received detailed verbal explanations regarding the procedure. The children were blinded to the type of sealant used.
A total of 64 children were initially assessed for eligibility. Of these, 55 children met the inclusion and exclusion criteria and were thus selected for the study.
Inclusion criteria
The study included children between the ages of 6 and 9 who exhibited a high risk of caries and Frankl’s behavior ratings of 3 or 4. Fully erupted, caries-free maxillary and mandibular first permanent molars with deep retentive pits and fissures were also included in the study. These criteria were evaluated through a clinical examination of the teeth using a mirror and a blunt probe, as well as the analysis of bitewing radiographs.
Exclusion criteria
Maxillary and mandibular molars with incipient caries, deep cavitated carious lesions, existing restorations, or previous sealants on occlusal surfaces, as well as hypomineralized molars and those with developmental disturbances were excluded from the study. Additionally, the participants included in the study were not using any removable or fixed dental appliances.11
Randomization
The selected teeth were randomly divided into 2 groups (Group A and Group B) using the computer-assisted randomization software (Rando 1.2 v. 2004; JIPMER, Puducherry, India). The allocation concealment was achieved with the use of sequentially labeled opaque envelopes. The allocation was performed by an independent individual. Each group (Group A and Group B) consisted of 70 first permanent molars (35 maxillary and 35 mandibular). In Group A, a hydrophilic sealant (UltraSeal XT Hydro) was applied, while Group B was treated with a hydrophobic sealant (Conseal F).
The sealants were applied in accordance with the manufacturer’s instructions by a single operator, who also calibrated the clinical protocol for the procedure.
In Group A, the tooth was isolated from the oral cavity with the use of a rubber dam. Prophylaxis was conducted using a slow-speed contra-angle micromotor handpiece with a bristle brush and polishing paste. The tooth was thoroughly rinsed with water for 30 s, after which it was dried with a three-way syringe. Acid etching was conducted for 20 s using 35% Ultra-Etch phosphoric acid gel (Ultradent Products, Inc., South Jordan, USA). Subsequently, the etched surface was rinsed with water for 30 s and slightly air-dried to remove any standing or pooled water. The tooth surface was treated with care to prevent desiccation. UltraSeal XT Hydro was applied with a brush tip and distributed evenly across all pits and fissures on the tooth surface. The sealant was light-cured for 20 s (Bluephase N MC; Ivoclar Vivadent, New York, USA). Then, the sealant was examined for marginal adaptation with an explorer, and the evaluation of the occlusion was conducted.12
In Group B, the tooth was isolated with a rubber dam, and prophylaxis was performed as described above. The tooth was rinsed thoroughly with water for 30 s and dried with a three-way syringe. Acid etching was performed for 20 s using 35% Ultra-Etch phosphoric acid gel (Ultradent Products, Inc.), followed by rinsing with water for 30 s. Then, the tooth was air-dried for 15 s using a three-way syringe, and checked for a frosted appearance. If a frosted appearance was not achieved, additional 10 s of etching were performed. Then, the stae total etch adhesive system (SDI Limited, Melbourne, Australia) was applied. The tooth surface was slightly air-dried to facilitate the even distribution of the bonding agent, which was then light-cured for 20 s. The Conseal F sealant was applied by placing the sealant tip on the mesial pit and spreading it over all pits and fissures of the maxillary molars. The same process was carried out on the mandibular molars, ensuring that no air bubbles were incorporated. The sealant was light-cured for 20 s and examined for marginal adaptation with an explorer.11
Clinical evaluation
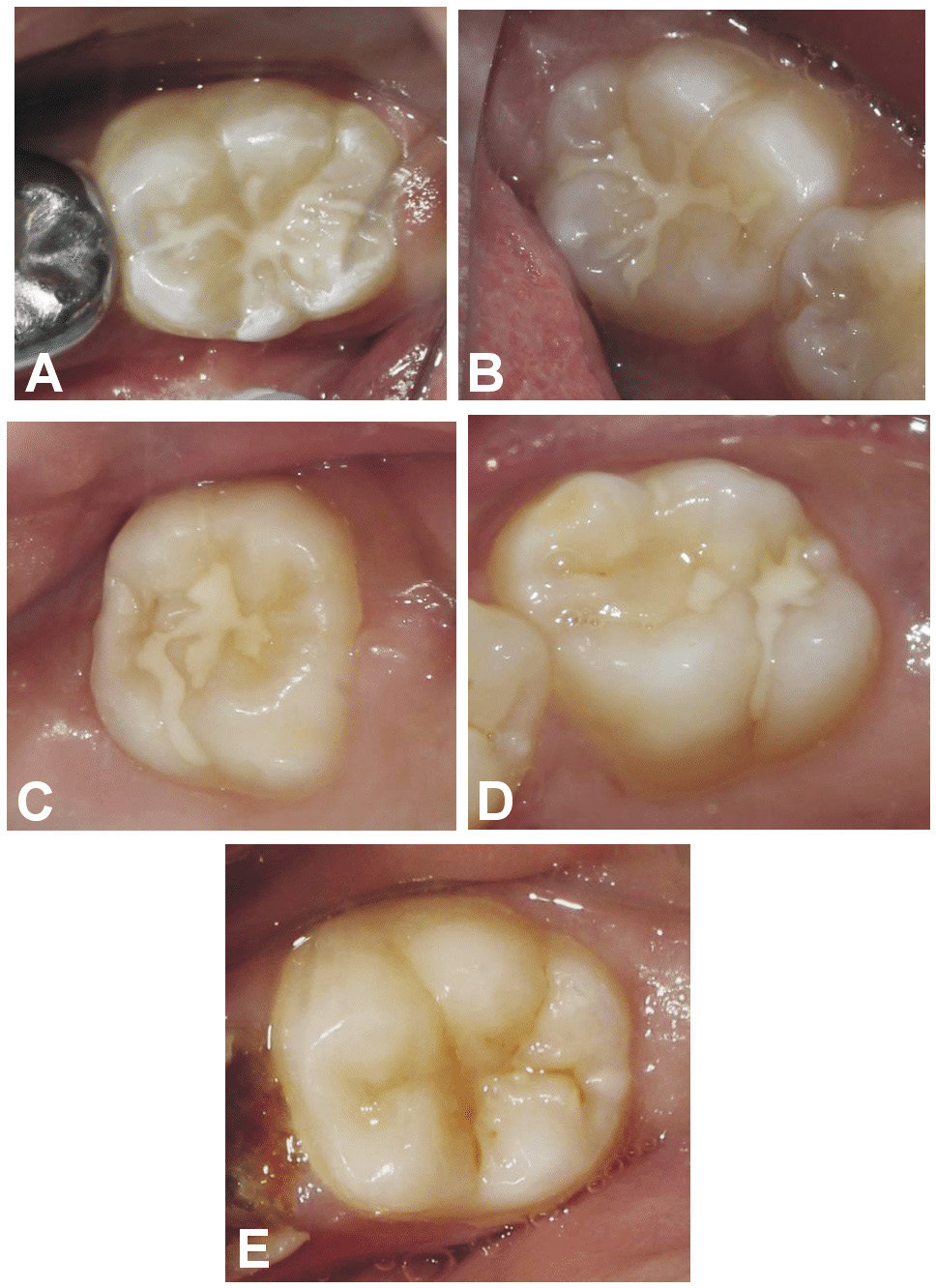
Clinical evaluations of the sealants were performed by 2 independent, calibrated examiners who were blinded to both study groups. All sealants were evaluated according to the modified United States Public Health Service (USPHS) clinical rating system at baseline and at 1, 3, 6, and 12 months (Table 1).13, 14 At each recall visit, any plaque and debris on the tooth were removed with a piece of gauze. The tooth was then air-dried, and the sealants were evaluated using a dental explorer for retention, marginal adaptation and marginal discoloration (Figure 2).
Statistical analysis
The data scores for retention, marginal adaptation and marginal discoloration were expressed as counts with percentages and analyzed using the Windows-based MedCalc Statistical Software v. 18.1.1 (MedCalc Software Ltd., Ostend, Belgium; https://www.medcalc.org).
The retention, marginal discoloration and adaptation scores within each group were analyzed using the Friedman test. The differences between the groups were analyzed using post hoc Mann–Whitney U tests. All tests were two-sided, with an alpha set at 0.05. The inter-examiner variability was evaluated using Cohen’s kappa test.
Results
The study was initiated with a total of 55 children, comprising 70 sealants in each of the 2 experimental groups (Group A and Group B). The mean age of the children was 7 years. Five subjects with 10 sealants in each group were lost to follow-up at 12 months. At 12 months, kappa agreement values for retention, marginal adaptation and marginal discoloration were 0.914, 0.918 and 0.936, respectively. These scores indicate almost perfect agreement between the examiners.
Within-group analysis
Statistically significant differences (p < 0.0001) were observed between the baseline and 12-month time points for retention, marginal adaptation and marginal discoloration in both groups (Table 2).
Between-group analysis
With regard to retention, no significant differences were found at baseline, 1 month and 3 months between hydrophilic and hydrophobic sealants. However, at the 6-month follow-up, the hydrophobic sealants showed significantly better retention compared to the hydrophilic sealants (p = 0.024). At the 12-month follow-up, the hydrophobic sealants continued to show significantly better retention compared to the hydrophilic sealants (p = 0.001). Notably, 10% of the sealants in the hydrophilic group and 1.7% in the hydrophobic group were completely lost and required replacement at the 12-month follow-up. This finding highlights the superior retention of hydrophobic sealants (Table 3).
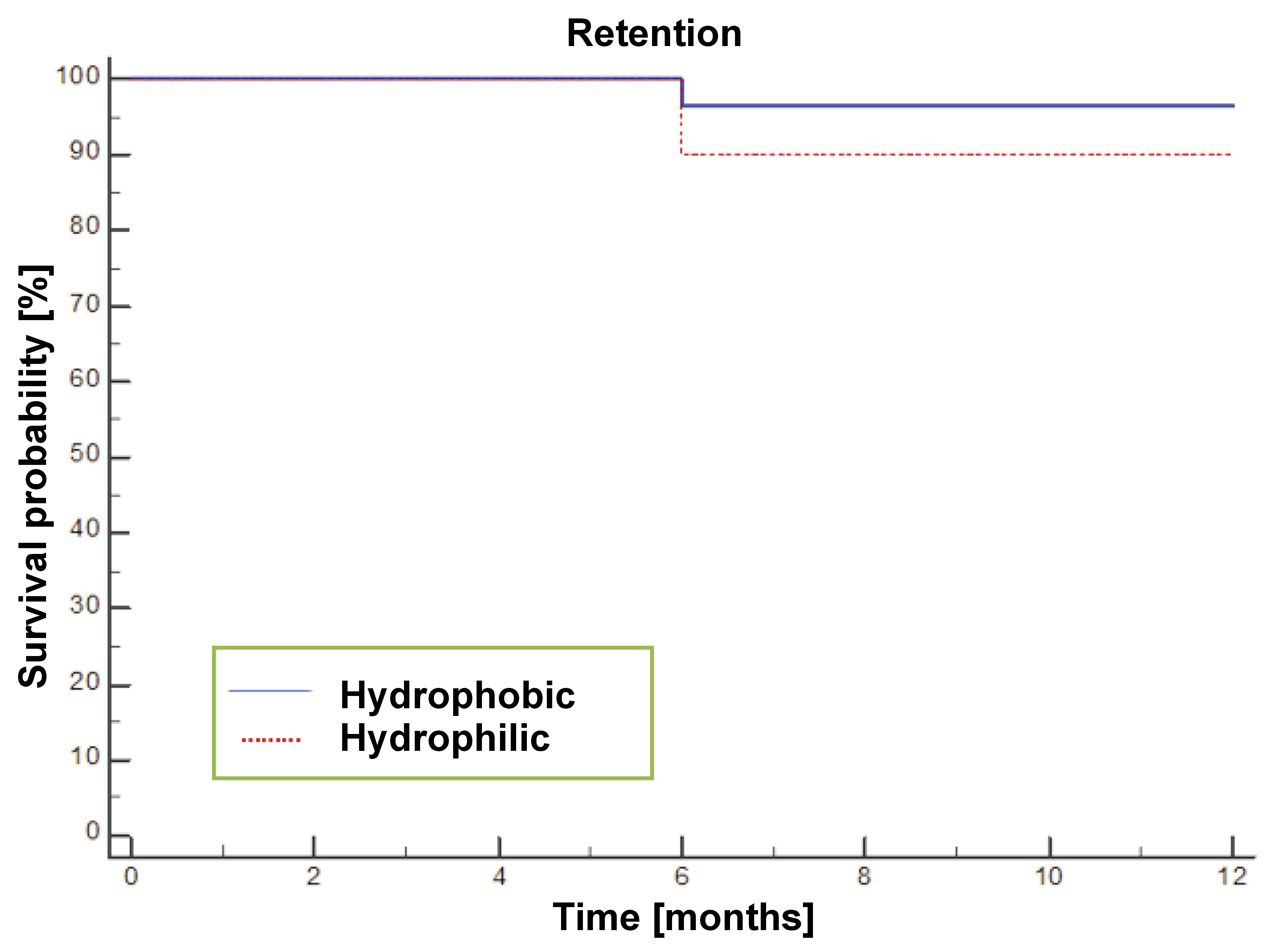
The survival rates of the sealants were assessed at baseline and at 1, 3, 6, and 12 months. All sealants showing retention scores of Oscar, Alpha and Bravo were classified as surviving, whereas retention scores of Charlie and Delta indicated loss. A total of 96.7% of sealants in the hydrophobic group and 90% in the hydrophilic group demonstrated survival over the 12-month period (Figure 3).
With regard to marginal adaptation, no significant difference was observed between the 2 groups up to the 3-month follow-up. However, at the 6-month (p = 0.015) and 12-month (p = 0.023) follow-ups, the hydrophobic sealants demonstrated significantly better marginal adaptation compared to the hydrophilic sealants (Table 4).
Regarding marginal discoloration, hydrophilic sealants showed significantly greater discoloration than hydrophobic sealants at the 1-, 3- and 6-month follow-ups. By the 12-month follow-up, 85.0% of sealants in the hydrophobic group were free of marginal discoloration, whereas only 61.7% of sealants in the hydrophilic group remained free of marginal discoloration. A statistically significant difference was observed in favor of hydrophobic sealants when marginal discoloration was compared between the 2 groups at the 12-month follow-up (p = 0.004) (Table 5).
Discussion
The efficacy of pit and fissure sealants in preventing caries is dependent upon their retention and marginal adaptation. Therefore, the objective of this study was to compare the effectiveness of hydrophilic (UltraSeal XT Hydro) and hydrophobic (Conseal F) sealants with respect to retention, marginal adaptation and marginal discoloration.
The results of this study demonstrate that Conseal F showed significantly better retention compared to UltraSeal XT Hydro at both the 6-month and 12-month follow-ups. By the end of the 12-month period, the failure rate of UltraSeal XT Hydro was found to be higher (10%) than that of Conseal F (3.3%). According to a review of published data on sealants, a loss rate of 5–10% per year is generally expected. The failure rate observed in this study is consistent with the expected range.15
The lower retention rate of UltraSeal XT Hydro can be attributed to a number of factors. One potential explanation could be its filler content, which is 53%, compared to only 7% in Conseal F.16, 10 Studies by Handelman et al. and Barrie et al. have shown that unfilled sealants tend to exhibit the improved retention compared to filled sealants.17, 18 Another factor could be the reduced penetration depth of the UltraSeal XT Hydro sealant. In a study by Gawali et al., UltraSeal XT Hydro showed significantly reduced penetration compared to the hydrophobic sealant (Fissurit).19 Additionally, Eliades et al. conducted a laboratory study which demonstrated that hydrophobic sealants exhibit superior sealing characteristics. Hydrophilic sealants, while offering improved setting properties, have lower flow, which affects their ability to penetrate fissures.20
The higher retention rates observed with Conseal F in this study may also be attributed to the application of a bonding agent prior to the pleacement of sealants. Studies by Hitt and Feigal and Asselin et al. have reported that the use of a bonding agent prior to the placement of sealants results in enhanced bond strength and a reduction in microleakage when compared to instances where a bonding agent is not used.21, 22
The results of this study are similar to those of Schlueter et al. and Mohapatra et al., who reported significantly better retention of hydrophobic sealants in comparison with hydrophilic sealants after 1 year.9, 23 In contrast, studies conducted by Khatri et al., Bhatia et al. and Bhat et al. reported a better retention rate of hydrophilic sealants compared to hydrophobic sealants.11, 24, 25 Prabakar et al. demonstrated that hydrophilic UltraSeal XT Hydro exhibited enhanced sealant coverage (retention) relative to the conventional Clinpro™ Sealant.26
Alongside retention, the marginal adaptation of the sealant is important for its clinical effectiveness. Sealants with poor adaptation can create plaque-retentive sites. Several factors contribute to poor marginal adaptation, including viscosity, polymerization shrinkage, which can result in tensions at the tooth/sealant interface, the formation of marginal microcracks, and ultimately, flaws in the adhesion of the material to the tooth structure.27
In the present study, Conseal F exhibited significantly better marginal adaptation compared to UltraSeal XT Hydro at the 6- and 12-month follow-ups. This difference in adaptation may be attributed to the higher viscosity of UltraSeal XT Hydro compared to Conseal F. A study by Mehrabkhani et al. concluded that low-viscosity sealants had significantly better marginal adaptation (p < 0.002) in comparison to high-viscosity sealants.28
Marginal discoloration of a sealant is often considered an early indicator of its loss of marginal integrity with the adjacent tooth structure. The discoloration is a consequence of marginal breakdown, resulting in a rough and irregular surface. This can create sites for the accumulation of plaque and food debris, as well as facilitate the penetration of oral fluids, which may lead to microleakage and secondary caries formation. If marginal discoloration extends into the margins of the sealant toward the pulp, it should be thoroughly examined with radiographs for potential secondary caries.29 The UltraSeal XT Hydro sealant showed a significantly higher incidence of marginal discoloration at 1, 3, 6, and 12 months. However, none of these discolorations extended toward the pulp, and they disappeared after polishing.
This study is one of the few to compare both hydrophilic (UltraSeal XT Hydro) and hydrophobic (Conseal F) sealants using a split-mouth study design over a period of 12 months. A randomized split-mouth design was selected to control factors such as patient behavior, diet and oral hygiene, which could influence sealant retention.30 Additionally, 120 first permanent molars were randomly assigned to the study groups, with 30 maxillary and 30 mandibular molars in each group. This approach helped to control retention variations resulting from the observed anatomical differences in these teeth.
When sealants are applied in children with a high risk of caries, a review of sealant retention should be part of the recall visits. It is recommended that the recall interval for these children does not exceed 12 months.31 In this study, which included children with a high risk of caries, recalls were conducted at 1, 3, 6, and 12 months to assess the effectiveness and retention of pit and fissure sealants.
Visual and tactile examinations were employed in this study to evaluate the retention, marginal adaptation and discoloration. This approach may introduce subjective variability in the evaluation, which could be a limitation of the current study. The use of additional methods of evaluation, such as standardized photographs or computer-based software programs, could provide a more objective assessment of these variables.
Accordingly, further studies with extended follow-up periods and more objective assessment methods are required to assess the effectiveness of these sealants.
Conclusions
The findings of this study indicate that the retention and marginal adaptation of Conseal F (hydrophobic sealant) were significantly better compared to those of UltraSeal XT Hydro (hydrophilic sealant) over a follow-up period of 1 year. Thus, both the null and alternative hypotheses were rejected. The marginal discoloration of Conseal F was significantly higher than that of UltraSeal XT Hydro. However, in both groups, the discoloration could be removed by polishing. Therefore, Conseal F demonstrated superior properties compared to UltraSeal XT Hydro in this study.
Ethics approval and consent to participate
The study was approved by the Institutional Review Board (Terna Dental College, Navi Mumbai, India; reference No. TDC/IRB-EC/145/2017). Written informed consent was obtained from parents before the procedure.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.