Abstract
One of the most important factors that determine the success of pulpectomy in primary teeth is the root canal filling material used. This systematic review is an update on the success rates of various materials used for obturation in primary teeth. An electronic search was carried out in the PubMed, Scopus, Web of Science, and Cochrane Library databases with the preset inclusion and exclusion criteria. Only randomized or quasi-randomized clinical and controlled trials with a minimum follow-up of 12 months were included for analysis. Nine articles were considered potentially eligible for inclusion in this review. All the included trials had zinc oxide–eugenol (ZOE) cement as a control group. The time span of the included trials extended from 12 to 30 months. Only 2 trials were at low risk of bias. Evidence to support the success rates of obturating materials used in primary teeth is scarce, which necessitates further high-quality randomized controlled clinical trials with regard to this issue.
Keywords: systematic review, deciduous tooth, obturating materials, primary tooth, meta-analysis
Introduction
Dental caries in primary teeth is the most pervasive chronic disease, with a prevalence of approx. 60–90% among children. If untreated, this disease may cause irreversible pulpitis requiring root canal treatment. This, in turn, affects the general health of children and disrupts their quality of life.1, 2, 3 The management of dental caries in primary teeth is extremely challenging for pediatric dentists, and endodontic treatment is the only option to treat and preserve primary teeth with chronic irreversible pulpitis in a symptomless state until they are replaced by permanent teeth. This treatment is achieved via a procedure called pulpectomy, which includes the chemo-mechanical preparation of the root canals of primary teeth. The prepared root canals are filled with a material that should have maximal antibacterial effects and the ability to resorb at the same rate as primary teeth.4 The complexity of the root canal morphology, along with the process of physiological resorption in primary teeth, is an inherent hindrance to effective instrumentation, and therefore, an ideal obturating material is needed to ascertain the success of root canal treatment.5, 6
There are abundant obturating materials for primary teeth available on the market, but none of these materials meets the requirements completely.7 Until 2008, zinc oxide–eugenol (ZOE) cement was the only root canal filling material for endodontically treated primary teeth.8 However, ZOE cement has limited antimicrobial action and a slow resorption rate, and if it is extruded beyond the apex, it can cause irritation to the periapical tissues, lead to the necrosis of the bone and cementum, and reorient the path of eruption among permanent teeth.9, 10, 11
Therefore, it was necessary to find an appropriate replacement for ZOE cement among root canal filling materials for primary teeth, one of them being iodoform paste.12 Iodoform was introduced for obturation in primary teeth; despite having good clinical and radiographic success rates, it accelerates the root resorption of primary teeth.13 Additionally, it produces yellowish discoloration of the tooth, which, in turn, has a negative esthetic effect.14 The major drawback of using calcium hydroxide (Ca(OH)2) as an obturating material is that it provokes inflammatory root resorption in primary teeth when in proximity to any vital pulp tissue.15 Currently, the combination of Ca(OH)2 and iodoform paste is used in practice, given its potent antimicrobial properties and an easy resorption rate when extruded without any foreign body reactions. However, the material resorbs faster than the tooth, resulting in a hollow tube effect that leads to uncertainty regarding the prognosis of the pulpectomized tooth.10, 16 Recently, Endoflas was introduced, comprising ZOE cement, Ca(OH)2 and iodoform; this material was proposed to have all the desirable properties of an ideal obturating material in primary teeth.17 As none of the abovementioned materials can be considered the optimal obturating material in deciduous teeth, the search for better materials continues via the modification of the existing materials with new components.7, 18, 19, 20, 21, 22
Owing to the complex, varied morphology of primary root canals, the complete removal of the pulp tissue is not always possible, and therefore, the obturating material used largely contributes to the prognosis and success of pulpectomy-treated primary teeth. Although there are numerous options available for one to choose as the close-to-ideal root canal filling material in primary teeth, there is no consensus among pediatric practitioners regarding the best available material for obturation in primary teeth. Hence, the present systematic review aimed to critically assess the available dental literature on the clinical and radiographic success rates of various obturating materials used for pulpectomy in primary teeth.
Material and methods
Search methodology for trial identification
The systematic review was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (CRD42021286974), and was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 statement.23 The PubMed, Scopus, Web of Science, and Cochrane Library electronic databases were searched without any date and language restrictions. The preset inclusion and exclusion criteria were used during the search. The authors manually searched for additional eligible trials. Other review articles were also examined to retrieve relevant references. The search terms used were: ‘primary teeth’; ‘deciduous tooth’; ‘deciduous dentition’; ‘primary dentition’; ‘children’; ‘obturating materials’; ‘zinc oxide eugenol’; ‘calcium hydroxide’; ‘iodoform’; ‘endoflas’; ‘root canal filling material’; ‘clinical success rate’; ‘radiographic success rate’; and ‘quality of obturation’.
Criteria for the inclusion of trials
Only randomized or quasi-randomized clinical and controlled trials with a minimum follow-up of 12 months were included for analysis. Trials with less than 1 year of follow-up were excluded. Additionally, observational studies and pilot studies were excluded from this review.
Included participants: children between 4 and 9 years of age.
Intervention: any form of obturating material for primary teeth, including both conventional and newly experimented materials.
Type of outcome measures: the primary outcome measure in this review was the clinical and radiographic success rates; the quality of obturation was considered a secondary outcome.
Collection and analysis of data
The screening for eligibility for the trials was performed independently by 2 review authors. Duplicate studies and studies that did not meet the inclusion criteria were excluded. Data regarding the general characteristics and outcome variables of the included studies were extracted. The criteria used for assessing the clinical and radiological success rates were the same for each study. The quality of the included studies was assessed using the Consolidated Standards of Reporting Trials (CONSORT) guidelines.24
Assessment of the risk of bias
of the included trials
The risk of bias was appraised by 2 authors independently, and any difference in opinion between them was sorted out by discussion or by involving another pediatric dentist. The assessment of the risk of bias was carried out using a refined and adapted tool of the Cochrane Collaboration. Five domains were assessed, namely, sample size determination, random sequence generation, allocation concealment, blinding of the participants/personnel, and blinding of the outcome assessment. Each domain was recorded as either low or high risk based on the information reported in the study. A judgment of ‘unclear risk of bias’ was marked when the trial methods were unclear and until any further information from the authors involved in the trial was available. The overall risk of bias in the included trials was then assessed as follows25:
– low risk of bias – when all 5 domains were assessed as low risk of bias;
– high risk of bias – when at least one domain was assessed as high risk of bias; and
– unclear risk of bias – when at least one domain was assessed as unclear risk of bias, but none of the domains were assessed as high risk of bias.
Results
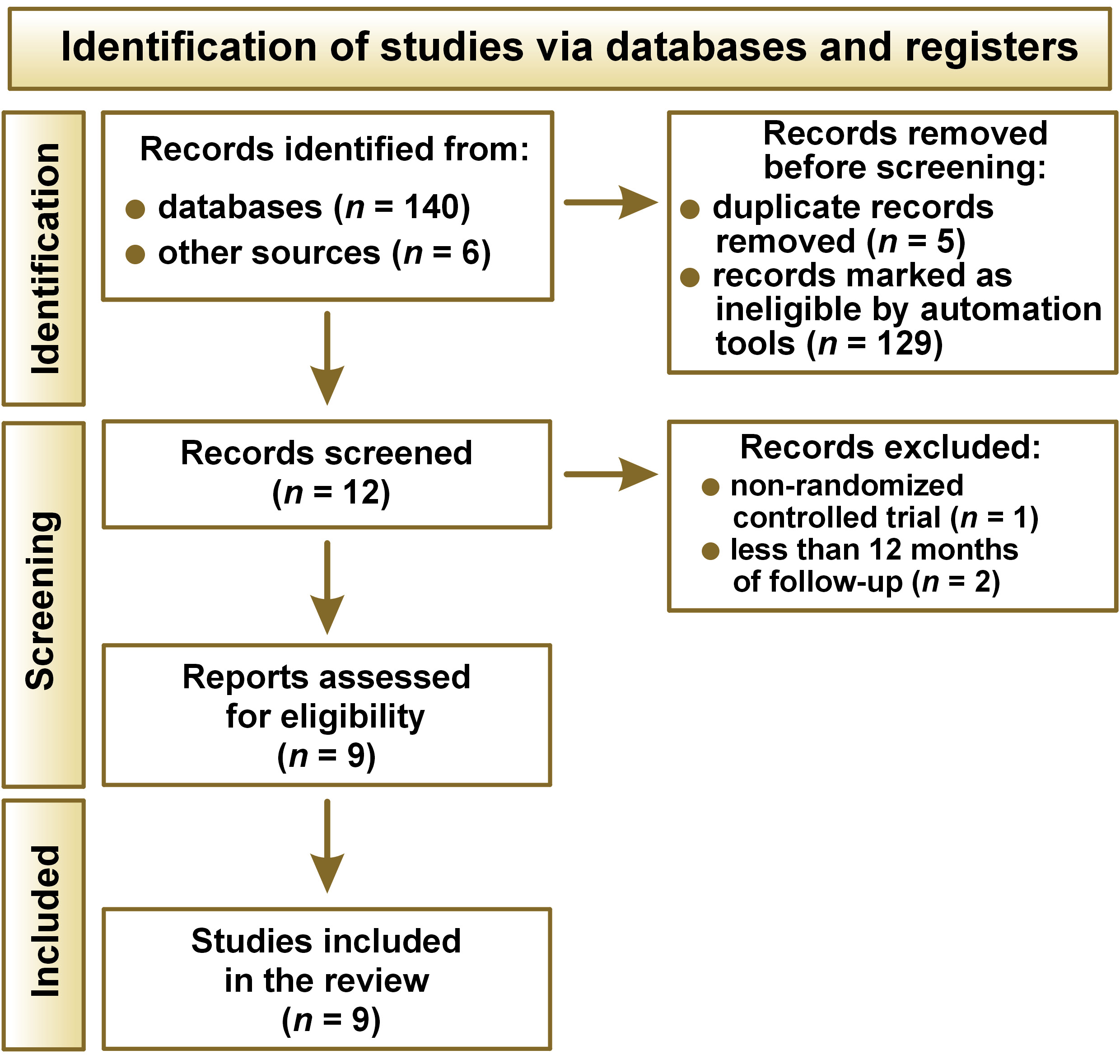
After thoroughly searching the electronic databases and other sources, 146 articles were identified. Of these, 129 articles were excluded after reading the title, as the records were irrelevant. After removing duplicates, 12 articles were screened, and 3 articles were further excluded, as one of them was not a randomized controlled trial, and the other 2 had a follow-up period shorter than 12 months.22, 26, 27 Nine articles were considered potentially eligible for this review.7, 10, 17, 28, 29, 30, 31, 32, 33 The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) flowchart is shown in Fig. 1.
Characteristics of the included studies
We included 9 trials in this review, all of which were published between 2004 and 2020. One trial was self-funded,30 1 trial received a grant from the Program for New Clinical Techniques and Therapies of Peking University School and Hospital of Stomatology, China,7 2 trials mentioned that they did not receive any financial support,32, 33 and the remaining 5 studies provided no information relating to the funding sources.10, 17, 28, 29, 31 The characteristics of the included studies are depicted in Table 1.
Design and methods
Four studies were randomized clinical trials (RCTs),10, 28, 30, 31 2 studies were quasi-randomized trials,17, 29 and the other 3 studies were randomized controlled trials.7, 32, 33 All the included trials used ZOE cement in one group, and 4 studies had multiple-treatment groups that were compared with ZOE cement.7, 17, 30, 31 The study duration of the included trials (the follow-up period) ranged from 12 to 30 months.
Participants
The trials included participants aged 4–9 years, with a total of 726 teeth treated with pulpectomy.
Interventions
All the included trials used ZOE cement in one group. Vitapex was tested in 4 trials,7, 10, 28, 30 Metapex in 1,17 RC Fill in 1,30 Endoflas was included as one of the test groups in 3 trials,17, 31, 32 mixed primary root canal filling (MPRCF) was tested in 1 trial,7 zinc oxide (ZnO)–ozonated sesame oil was tested in 1 trial,29 another tested ZnO with the Aloe vera extract and ZnO with 10% sodium fluoride (NaF),31 and the other trial the ZnO–propolis mixture.33
Outcome measures
All the trials reported the clinical and radiographic success rates of the obturating materials tested. Two trials also reported on the quality of obturation.10, 17
Risk of bias of the included trials
Table 2 depicts the summary of the risk of bias assessment for the 9 trials included in the review. Two trials were found to have a low risk of bias,7, 33 and the remaining 7 studies were considered to have a high risk of bias.10, 17, 28, 29, 30, 31, 32 Six included trials showed selection bias, as sample size determination or random sequence generation or allocation concealment were not achieved.10, 17, 28, 29, 31, 32 We considered 6 studies to have a high risk of performance bias, as the blinding of the participants was either not completed or not mentioned.10, 17, 28, 29, 30, 31 Five trials had a high risk of detection bias, as the outcome assessor was not blinded.10, 17, 28, 29, 31
Discussion
This systematic review was intended to evaluate the clinical and radiographic success rates of various obturating materials used in primary teeth. Eleven different obturating materials were used in the 9 trials included for review. For all of the trials included, ZOE cement was used as one of the obturating materials or control groups. Other materials evaluated included Vitapex, Metapex and Endoflas, all of which are conventionally used materials. New materials included ZnO with iodoform, MPRCF, ZnO–ozonated sesame oil, ZnO with the Aloe vera extract, ZnO with 10% NaF, and the ZnO–propolis mixture.
The secondary intent of this review was to determine the quality of obturation with these root canal materials in primary teeth. There were only 2 trials that evaluated the quality of obturation10, 17; however, statistical significance was not mentioned to detect a clear relationship between the obturating material and the quality of obturation. This indicates that there are no studies in the literature determining the relationship between the obturating material used and the quality of obturation.
In terms of methodological limitations of the included trials, only 2 trials were found to have a low risk of bias,7, 33 whereas others were found to have a high risk of bias. The domain most commonly found to be at high risk of bias was allocation concealment and blinding of the participants, followed by blinding of the outcome assessor and sample size determination.
This review found, in the head-to-head comparisons, that each of the examined obturating materials was more effective than ZOE cement. However, most of the included trials had a high risk of bias, and hence, we could not draw any definite conclusions. Taking studies with a low risk of bias into consideration, MPRCF and the ZnO–propolis mixture were better alternatives to ZOE cement.
The MPRCF contains 0.28 g of ZnO, 0.18 g of iodoform, and 0.01 g of Ca(OH)2. Notably, the composition of MPRCF is similar to that of Endoflas, which is considered close to the ideal root canal filling material in primary teeth. The trials that tested Endoflas also showed a high success rate despite having a high risk of bias.17, 31, 32 Hence, more research should be focused on developing an ideal root canal filling material incorporating these components.
The other alternative is the ZnO–propolis mixture that replaces eugenol with propolis. Propolis is proven to have antimicrobial and anti-inflammatory properties.34, 35 However, the preparation of the mixture and the concentrations of the ingredients were not mentioned in the included trial.33 Another important fact that should not be neglected is that any new alternative to ZOE cement, including both MPRCF and the ZnO–propolis mixture, still contains ZnO as one of its key components. Studies have shown that ZOE cement shows good resistance to bacterial leakage and inhibits most organisms,36, 37 indicating that ZnO is an inevitable component of any new alternative.
Unfortunately, the trials included in this review were all heterogeneous, and hence, we were not able to perform a meta-analysis. Evidence from the trials included in this review cannot be applied to clinical practice due to a major void in the methodological constraints. With pulpectomy being the major procedure in pediatric dental practice, it is surprising to know that no qualitative studies are assessing the quality of obturation and the success rates of the obturating materials used in primary teeth. Future trials must be well-designed RCTs in accordance with the CONSORT statement, and all possible measures should be taken to prevent any sort of bias.
Conclusions
Based on the scientific information available, there seems to be a low level of evidence to support the success rates of a new ideal root canal filling material for primary teeth. High-quality randomized controlled clinical trials with a minimum of 12 months of follow-up are needed to decide upon the best obturating material for primary teeth, as at present, there is no consensus among pediatric dentists with regard to this issue.
Ethics approval and consent to participate
Not applicable.
Data availability
All data generated and/or analyzed during this study is included in this published article.
Consent for publication
Not applicable.