Abstract
The correlation between magnetic resonance imaging (MRI) signs and clinical findings has been highlighted in multiple studies. However, very little information is available on the correlation between the bilateral temporomandibular joints (TMJs) of the same individual. The majority of efforts in the clinical research setting have focused on the correlation between ipsilateral imaging and clinical findings, while less attention has been paid to the contralateral imaging findings of the anatomical structures.
The objective of this paper was to review the existing literature that compares temporomandibular joint (TMJ) magnetic resonance imaging (MRI) findings from both sides of the same individual.
In January 2024, a systematic search of the literature from major search engines (MEDLINE (PubMed), Scopus) was conducted to identify all peer-reviewed English-language studies that presented an MRI comparison of left and right TMJ data in the same patients. The articles were analyzed using a Population/Intervention/Comparison/Outcome (PICO) format.
The search terms “temporomandibular joint” AND “magnetic” AND “resonance” yielded 2,561 results. Only 2 papers met the established inclusion criteria. The results of the papers included in the systematic review were not comparable due to differences in the evaluation of the TMJs, which prevented a meta-analysis. Manfredini et al. identified a statistical correlation between disc displacement, osseous changes (OC) and joint effusion (JE) between the joints of the contralateral sides. Koca et al. observed a significant difference in TMJ MRI findings between the painful and non-painful sides of each individual in a bruxism group and a control group (p = 0.001, p < 0.001 and p = 0.004, p < 0.001, respectively).
The studies on the correlation between the right and left TMJs remain scarce. A comparative analysis of the 2 sides of the TMJ in individual patients is rarely reported.The review did not identify a common result for the findings of the contralateral TMJs in the 2 articles included.
Keywords: magnetic resonance, temporomandibular joint disorder, bilateral evaluation
Introduction
The temporomandibular joint (TMJ) is a fundamental structure of the stomatognathic system and is composed of several components, including the articular fossa, articular eminence, disc, and mandibular condyle. When there is an issue with the TMJ and/or the masticatory muscles, the resulting musculoskeletal symptoms are known as temporomandibular disorders (TMD).1, 2 Temporomandibular disorders are the most common non-odontogenic cause of orofacial pain and include cardinal symptoms such as pain, limited jaw movement and joint noises, which may have a negative impact on an individual’s quality of life.3
The use of medical imaging is important for the differential diagnosis of TMD. Consequently, studies on the correlation between imaging and clinical findings are of paramount importance in order to gain a better insight into an effective prescription. Although conventional radiography can provide images of the TMJ bony components, it offers a bidimensional evaluation that is often obstructed by other parts of the cranium. Currently, cone beam computed tomography (CBCT) and magnetic resonance imaging (MRI) have emerged as the reference imaging techniques.4, 5, 6 In particular, MRI is the gold standard for visualizing soft tissues of the TMJ and the presence of joint effusion (JE).7 With recent advancements in MRI hardware and techniques, dynamic imaging is now possible for MRI of TMD with significantly improved image quality.8, 9
The correlation of MRI signs with clinical findings has been highlighted in multiple studies.10, 11, 12, 13, 14 However, very little information is available on the correlation between the bilateral TMJs of the same individual.13 The majority of efforts in the clinical research setting have been directed towards investigating the correlation between ipsilateral imaging and clinical findings, while less focus has been put on the contralateral imaging findings of the anatomical structures. The ability to identify imaging signs associated with specific findings in the joints on the opposite sides of the body is potentially important from a clinical-pathological perspective, as it contributes to understanding the clinical relevance of specific imaging signs with respect to the presence of symptoms.15, 16 This is especially interesting when considering that the TMJs are a unique example of connected units.17 Based on these premises, the intent of this manuscript was to systematically review all of the publications correlating right and left TMJs in the same individual. The primary objective of the review was to assess the relationship between TMJ disorders diagnosed using MRI of the joints of both sides of the same individual.
Material and methods
Search strategy
A systematic search of the literature was conducted to identify all peer-reviewed English-language articles that were crucial for the topic of the review: the investigation of right and left TMJs in an individual patient by means of MRI. As a starting point, we conducted a search using Medical Subjects Headings (MeSH) terms in the National Library of Medicine, MEDLINE (PubMed) database. The following terms were adopted and inserted in the search bar: “temporomandibular joint” AND “magnetic” AND “resonance” (“temporomandibular joint” [MeSH terms] OR (“temporomandibular” [all fields] AND “joint” [all fields]) OR “temporomandibular joint” [all fields]) AND (“magnetic resonance spectroscopy” [MeSH terms] OR (“magnetic” [all fields] AND “resonance” [all fields] AND “spectroscopy” [all fields]) OR “magnetic resonance spectroscopy” [all fields] OR (“magnetic” [all fields] AND “resonance” [all fields]) OR “magnetic resonance” [all fields]). The results were sorted using the Best Match research engine filter. Next, an article screening strategy was implemented by excluding all the articles whose titles were not relevant to the search query. Subsequently, additional publications were excluded based on their abstracts, while the remaining articles were ultimately excluded following a full-text review. Finally, the search was expanded through the use of the “PubMed related articles” section and a manual search of the Scopus database.
Inclusion criteria
The following inclusion criteria were applied: articles written in English; articles presenting the investigation of TMJs through the use of MRI; articles correlating findings or specifically reporting findings from the 2 contralateral sides at the individual level.
Exclusion criteria
The following publications were excluded from the analysis: systematic reviews or meta-analyses; non-systematic reviews; case reports; studies reporting data from previous publications; opinion papers; letters to the editor; and articles published before the year 2000.
Selection of participants
The participants of the included studies were adults of both genders diagnosed with any type of TMJ disorder. The individuals underwent an MRI examination of both TMJs.
Structured reading
A Population/Intervention/Comparison/Outcome (PICO) strategy was employed to read and investigate the selected articles. The study population (“P”) was described in every article according to the inclusion criteria, the demographic features of the sample and the sample size. The study intervention data (“I”) was collected based on all procedural characteristics of the study, including the type of intervention/experiment, assessment instruments and statistical analysis. The presence of a comparison group (“C”), such as a control group or another comparison subset among the patient population, was documented within the comparison criterion. The study outcome (“O”) was evaluated in light of the need to assess a potential relationship between the TMJs of the left and right sides within the same patient. Given the extensive temporal range of the articles selected for the review, it was not feasible to structure the review according to the PICOT framework, where “T” represents the time frame.
Two of the authors participated in the stepwise search process (NGS and FS), independently reviewing titles and abstracts of all articles and then conducting a full-text screening. Two authors (MV and AC) supervised the activity and intervened in cases of uncertainty regarding the potential inclusion of an article or data interpretation. Once the review team had reached a consensus on the articles to be included in the review, the main reviewer (NGS) proceeded to perform data extraction based on the abovementioned PICO strategy. The initial plan was to conduct a meta-analysis of the data in the event that sufficient and homogeneous material was retrieved.
Estimation of the quality of studies
Grading of the level of evidence was based on the work of David Sackett and his team, as described by Richardson.18 The classification made by Sackett et al.19 is presented in Table 1.
Results
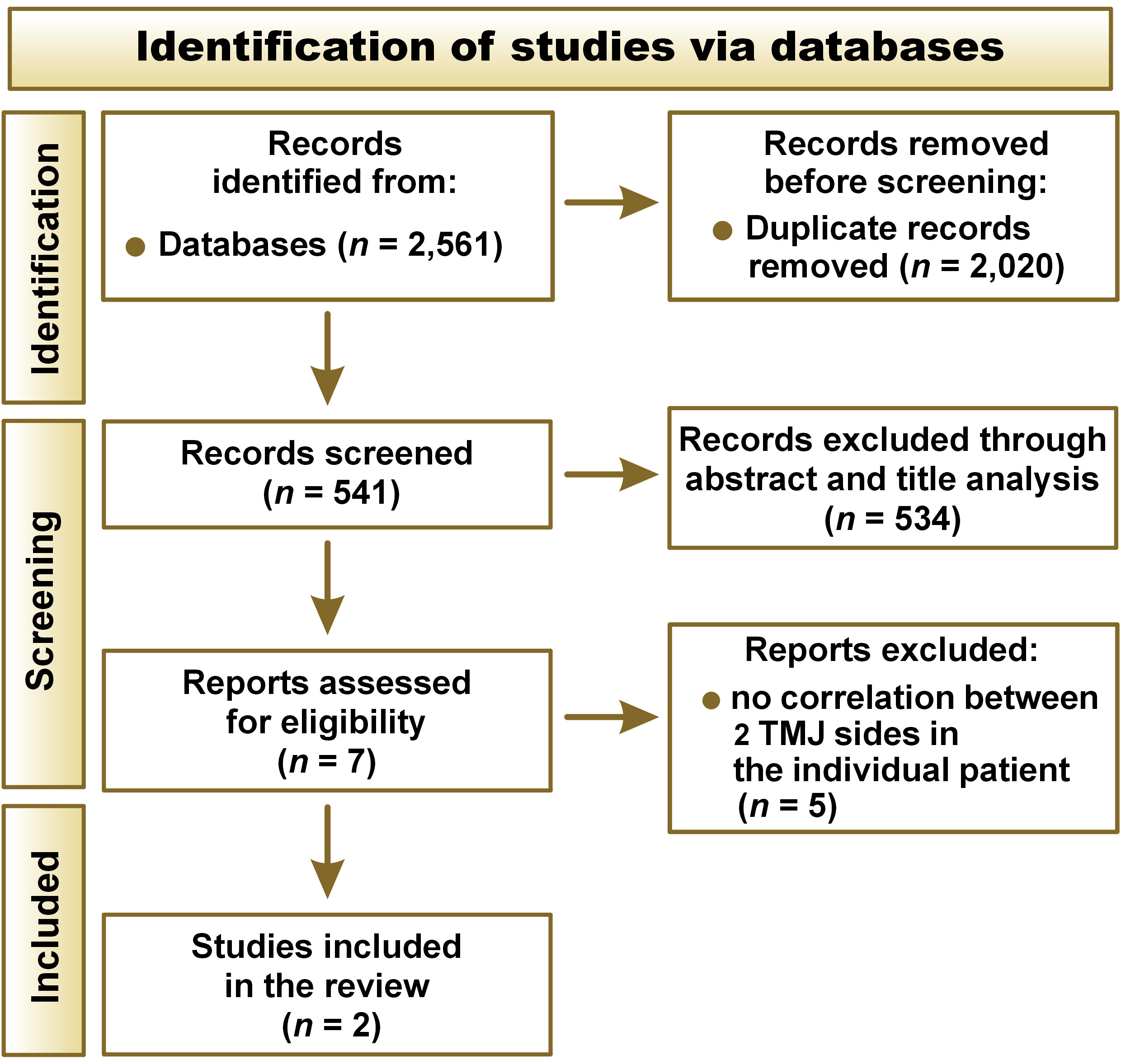
The literature search yielded 2,561 results, of which 2,020 were excluded due to duplication. Of the 541 remaining articles, only 7 were deemed potentially suitable for inclusion based on the assessment of abstracts. All 7 articles were read in full, and two13, 20 matched the eligibility criteria and were included in the study (Figure 1).
The main characteristics of the included articles are reported in Table 2.
Diagnostic equipment and MRI type
In both studies,13, 20 1.5 Tesla MRI scanners from 2 different manufacturers (GE Medical Systems, Buc, France; Siemens Healthcare GmbH, Erlangen, Germany) were involved in the diagnostic process. Both publications employed T1- and T2-weighted sequences for the evaluation of patients. In both studies,13, 20 participants underwent MRI analysis with open and closed mouth positions.
Study population
A total of 478 patients (300 female) were included in the 2 studies. The patients exhibited a range of TMD, and in both investigations, the following findings were evaluated: disc position; disc morphology; and osseous changes (OC).13, 20 Additionally, both Manfredini et al.13 and Koca et al.20 investigated the presence of effusion and fluid accumulation.
Quality of studies
Table 3Table presents the level of evidence for the 2 selected studies. The level of evidence was considered medium-low (III), given that both papers were cohort studies with a control group.13, 20
Comparison of right and left TMJs
Koca et al. compared TMJ MRI findings between painful and non-painful sides in TMD patients, distinguishing between bruxers and non-bruxers.20 Significant differences in the disc/condyle structure and effusion were present between the painful and non-painful sides of each patient (p < 0.05). The study demonstrated an increased prevalence of anterior disc with reduction, anterior disc without reduction, and effusion in patients exhibiting an abnormal disc/condyle relationship on the painful side, regardless of the group they belonged to (bruxism or no bruxism group). Manfredini et al. compared MRI signs on the left and right sides of the TMJ.13 The study found that if a specific diagnosis was present on one side, it was likely to be present on the opposite side as well. However, the study did not report on patient symptoms. The correlation level was moderate for disc displacement with reduction (DDR) (R = 0.47) and OC (R = 0.50). Additionally, the study found negative correlations between OC and JE, as well as between DDR and disc displacement without reduction (DDNR) in the opposite joint. The results of the global multivariate permutation test with Tippett’s combination method indicated that the null hypothesis of independence between the diagnoses of the 2 sides was rejected in favor of the hypothesis of positive global association at the α significance level of 0.001. The adjusted p-values exceeded the significance level, with the exception of the tests where a specific symptom on one side was compared with the same symptom on the other side.
Statistical analysis
Due to the limited number of available studies, it was not feasible to perform a meta-analysis for the purposes of this systematic review. Instead, a descriptive analysis of the studies was conducted.
Discussion
The distinctive characteristics of the TMJs have posed significant challenges to their study, necessitating the development of tailored approaches. In fact, the coordinated action of the right and left joints ensures the forward movement of the entire anatomical structure. Given that the 2 TMJs are non-disjointed structures, an interesting issue arises regarding the potential for pathologies in one joint to also affect the contralateral joint.2, 13, 21, 22 To date, there has been a paucity of studies addressing the concurrent contralateral findings.23, 24 Indeed, the majority of literature on TMD describes individual cases and focuses on the correlation between clinical and imaging results rather than on the bilateral joint findings.25
This paper presents a review of the articles that best address the topic of contralateral findings. In analyzed studies,13, 20 the participants were selected based on their TMD symptoms, even if some differences in the recruitment strategies prevented the findings from being combined. Indeed, Koca et al. included patients with unilateral preauricular pain and divided them into those with and without bruxism.20 Manfredini et al. did not provide any information on the concurrent presence of pain symptoms, which was beyond the scope of that paper.13 Both investigations employed similar 1.5 Tesla MRI machines for the evaluation of the TMJs. Images were acquired with the patient in the position of maximum mouth opening and with the mouth closed.
A previous study conducted by Takahara et al. revealed significant associations between pain, disc displacement, effusion, and degenerative changes.26 In the research carried out by Koca et al., the frequencies of intraarticular degenerative changes, effusion, DDR, and DDNR were significantly higher on the painful side of each patient compared to the non-painful side in both the control and bruxism groups.20 In accordance with previous studies,27, 28 the findings of Koca et al.20 revealed that the frequencies of abnormal disc/condyle relationships were significantly higher on the painful side of each patient in both the control and bruxism groups in comparison to normal disc/condyle relationships (p < 0.05). Additionally, significant differences were observed in the disc/condyle structure and effusion between the painful and non-painful sides of each patient in both groups (p < 0.05).20 In a study by Manfredini et al., it was found that diagnoses on one side of the TMJ were usually associated with the same diagnoses on the other side, pointing to a mutual interaction between the joints on opposite sides of the body.13 This is consistent with the theory that an imbalance between the loads exerted on the joint (such as prolonged jaw clenching) and the joint resistance (structural anatomy) can affect the TMJs bilaterally.17 This finding is a novel addition to the literature on the need to report the results of clinical assessments of the bilateral joints.23, 24 A study conducted by Görürgöz et al. on the TMJs of 258 patients using CBCT revealed that 209 out of 258 cases had bilateral condylar bone changes.29 The same study found no statistically significant difference between the types of degenerative changes on the right and left TMJs, as determined by McNemar’s test (p = 0.668). This supports the findings of Manfredini et al., which demonstrated an association between the diagnoses assigned to both TMJ sides.13
In addition, both studies13, 20 identified a correlation between DDNR and degenerative disease within the same joints. This supports the idea that the TMJ disc plays a protective role in preventing remodeling or damage to the articular bone structures. According to several papers,32 long-lasting displacement of the disc is associated with degenerative changes in the bone. As both studies are observational in nature, it is not possible to determine the causative factor responsible for joint degeneration originating from DDNR. However, the presence of DDNR may increase the risk of osteoarthrosis in the TMJs.33
This review focused on radiological signs observed on MRI scans of both sides of the TMJ. However, the conflicting results between the 2 included studies make it difficult to reach consistent conclusions. This may be due to the different criteria adopted for patient recruitment. The discrepancies in the selection of the study group, especially in the study by Koca et al., where 40.1% of the patients did not have bruxism or other systemic pathologies that could have led to joint degeneration, may have contributed to the partial inconsistency of the findings.20 On the other hand, Manfredini et al. did not provide any details regarding bruxism behaviors in the study group.13 Therefore, further investigation is needed to determine whether and how prolonged bruxism activities may influence the contralateral findings. From a clinical perspective, it is important to consider the presence of symptoms on one or both sides when interpreting the results of these studies. The prevalence of unilateral and bilateral clinical TMD symptoms and their frequency in patient populations have not yet been determined.23 It is plausible to suggest that certain patients may exhibit identical MRI findings on both sides despite experiencing symptoms on only one side, or the opposite may be true. This hypothesis is consistent with prior research indicating that the level of agreement between clinical and imaging diagnoses is not always flawless. Future research is required to ascertain the significance of imaging signs in the absence of clinical symptoms.
Conclusions
The limited number of papers and partially conflicting results precluded any definitive observation about the correlation between the 2 sides of the TMJ. It is a common practice in the international literature to consider only 1 TMJ for clinical research studies, as evidenced by the majority of publications. In light of these considerations, further research on the topic of contralateral findings is necessary in order to expand knowledge on the clinical relevance of MRI data.
Ethics approval and consent to participate
Not applicable.
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.