Abstract
Background. In Mexico and around the world, water in dental units, including triple syringes, comes from municipal chlorinated water mains. The microbial contamination of dental unit water systems constitutes a risk factor for opportunistic infections.
Objectives. The present work aimed to identify the bacteria present in the triple-syringe water lines of dental units at a dental school of a public university in Mexico, with a hypothesis that opportunistic bacteria of importance to human health would be found.
Material and methods. A cross-sectional study was carried-out. A total of 100 samples of triple-syringe tubing from dental units operated by a dental school of a public university in Mexico were analyzed before and after their use in dental practice. Bacterial biofilm was cultured and isolated from the tubing, using standard microbiological methods, and then the species present were identified through 16S rRNA gene sequencing. The characterization of the biofilm was performed by means of scanning electron microscopy (SEM).
Results. Bacterial growth was observed in 20% of the non-disinfected and 10% of the disinfected samples, with 11 strains isolated. Six genera and 11 bacterial species were genetically identified. Coagulase-negative staphylococci (CoNS), considered opportunistic human pathogens, were among the most critical microorganisms. Scanning electron microscopy revealed a thick polymeric matrix with multiple bacterial aggregates.
Conclusions. Opportunistic bacteria from human skin and mucous membranes were detected. Under normal conditions, these bacteria are incapable of causing disease, but are potentially harmful to immunosuppressed patients.
Keywords: genotype, microorganisms, opportunistic, triple syringe, dental chairs
Introduction
Biofilm formation and microbial growth in the water lines of dental units result in a great amount of microorganisms in the water used for cooling, cleaning and ultrasonic treatment in dentistry.1 In Mexico and various places worldwide, water in dental units, including triple syringes, comes from municipal chlorinated water supply.2 Municipal water harbors free planktonic bacteria, fungi, viruses, protozoa, unicellular algae, amebae, and nematodes, and this diversity produces multi-species biofilm. The intensity of the water flow, stagnation for more than 12 h, temperature, and the type of piping all contribute to biofilm formation and consolidation.3
There are few regulations to determine the acceptable level of bacteria in these environments. In Mexico, it is stated that with regard to human use and consumption, water must not contain fecal coliform bacteria or other microorganisms considered pathogenic.4 Furthermore, it is recommended that the amount of heterotrophic bacteria in water does not exceed 200 colony-forming units (CFU) per milliliter for the water to be acceptable in dental practice.5 Although many microorganisms are not detected in the unit inlet water, differences in the number and variety of microorganisms have been found in the outlet water, suggesting other forms of contamination, from sources such as water tanks and cisterns that supply water to dental units, bottled water used as deposits for dental units,6 or finally the patient’s or operator’s skin.7 In Mexico, water contamination has been detected in the conduction lines of dental units in studies carried out in dental schools.8, 9
Biofilm bacteria secrete exopolysaccharides that protect them from disinfectants and antibiotics, allowing them to adhere to surfaces and acquire nutrients. The microorganisms located on the outermost part of the biofilm and fragments of the biofilm themselves can be carried by the water flow or spread by aerosols from dental work, and cause cross-contamination and infection in both healthy and immunocompromised individuals.8, 9
Therefore, the present work aimed to identify the bacteria present in the triple-syringe water lines of dental units at a dental school of a public university in Mexico. It was hypothesized that opportunistic bacteria of importance to human health would be found in the collected samples.
Material and methods
A cross-sectional study was carried out. A total of 50 dental units from 2 postgraduate clinics of a public university in Mexico (25 from an endodontic clinic and 25 from a pediatric dentistry clinic) were examined. For this purpose, 100 triple-syringe tube segments were obtained and segregated as follows:
– disinfected samples (n = 50): The triple-syringe tubing was disinfected by passing through a 2% sodium hypochlorite solution for 2 min and letting it stay overnight. The following day, the municipal water stored in a cistern was allowed to run for 2 min, and 5-centimeter tubing samples were taken;
– non-disinfected samples (n = 50): The samples of were obtained from the same dental units, but without prior disinfection; they were taken after 3 weeks of continuous use, following standard clinic protocols.
For sampling, the external surfaces of the tubes were cleaned with 70% alcohol. The tubes were cut with a sterile scalpel, obtaining two 2.5-centimeter-long sections for bacteriological and microscopic studies. The ends of the cut sections were heat-sealed to keep the interior intact until seeding. Each sample was placed in a sterile bag, and no more than 5 h elapsed until analysis.
Bacterial isolation
The biofilm was sampled using sterile swabs. The samples were inoculated in Petri dishes with the selective culture media – Brain-Heart Infusion (BHI) Agar (BD Bioxon™, cat. No. 214700; BD, Franklin Lakes, USA), Pseudomonas Agar (cat. No. 244820; BD) and Enterococcus Agar (cat. No. 274620; BD). All plates and the 3 culture media included were incubated at 37°C for 24–48 h. Colonies that developed were isolated and purified to establish their macroscopic morphology. Gram staining was performed to determine the microscopic morphological characteristics.
Bacterial identification by 16S rRNA gene sequence analysis
The genetic identification of the strains was performed by sequencing the 16S rRNA gene. Biomass for this purpose was obtained by inoculating pure cultures in BHI Agar through mass streaking. The cultures were incubated for 48 h at 37°C. The biomass was then recovered by scraping the bacterial growth. Bacterial DNA was extracted using the Wizard Genomic® DNA Purification Kit (cat. No. A1120; Promega Corporation, Madison, USA) according to the manufacturer’s instructions.
Once the DNA was obtained, the 16S rRNA gene was amplified through polymerase chain reaction (PCR). The reaction mixture consisted of 3 µL of template DNA, 0.20 µL of the MyTaq polymerase mix (5 U/μL, 5 mM dNTPs (deoxynucleotide triphosphates), 15 mM MgCl2) (cat. No. BIO-21105; Bioline, London, UK), 2.5 µL of the reaction buffer, and 2.5 µL (1 µM) of each primer. The following nucleotide sequences were used as universal primers: 27f: 5’-AGTTTGATCMTGCTCAG-3’; and 1492r: 5’-TACGGYTACCTTGTTACGACTT-3’.
Thermal cycling conditions for gene amplification were as follows: an initial denaturation cycle for 5 min (at 94°C); denaturation for 1 min (at 94°C); annealing for 30 s (at 59°C); and extension for 1 min (at 72°C). In total, 30 cycles were repeated, and the final extension cycle was performed for 10 min (at 72°C).
The amplified fragments were observed using 1% agarose gel (Pronadisa, cat. No. 8100.10; Condalab, Madrid, Spain) stained with ethidium bromide (cat. No. E7637-1G; Sigma-Aldrich, St. Louis, USA). Electrophoresis was performed at 120 V for 40 min. Subsequently, the amplification products were purified using the Amicon® Ultra centrifugal filtration kit (cat. No. UFC500308; Merck Millipore, Burlington, USA) and sent to Macrogen USA (Macrogen Sequencing Service; Macrogen, Rockville, USA) for sequencing.
The obtained sequences were analyzed and corrected using the ChromasPro, v. 2.6.4 (Technelysium Pty Ltd., South Brisbane, Australia), and BioEdit, v. 5.0.9,10 programs. The consensus sequences were compared with the sequences deposited in the National Center for Biotechnology Information (NCBI) GenBank, using the Basic Local Alignment Search Tool (BLAST) and the EzBioCloud public database.
Characterization of the biofilm
For the morphological characterization of the biofilm, 0.5-millimeter sagittal sections were cut. The samples were fixed in 0.1% glutaraldehyde, washed twice in 0.2 M cacodylate buffer at 4°C and dehydrated by increasing ethanol concentrations (from 30% to 100%). They were then dried overnight in hexamethyldisilazane (HMDS) (Electron Microscopy Sciences, Hatfield, USA), mounted in aluminum sample holders and coated with gold-palladium. A scanning electron microscope (SEM) (model 4000; Jeol, Tokyo, Japan) was used to examine the samples.
Results
Of the total of 100 triple-syringe tube segments included in this study (50 non-disinfected and 50 disinfected samples), bacterial growth occurred in 10 (20%) of the non-disinfected samples (6 samples from the endodontic clinic (12%) and 4 samples from the pediatric dentistry clinic (8%)). Moreover, growth was observed in 5 (10%) of the disinfected segments (1 dental unit from the endodontic clinic (2%) and 4 from the pediatric dentistry clinic (8%)). Bacterial growth was observed in the BHI and Pseudomonas media, although no growth was detected in the Enterococcus medium in either sample type. However, a representative of the genus Enterococcus was isolated in the non-selective culture medium.
Finally, the microscopic and macroscopic analysis identified 11 strains, of which 7 (64%) were from the non-disinfected samples and 4 (36%) from the disinfected samples, including 5 Gram-positive bacilli (one of them spore-forming) (45%), 3 Gram-positive cocci (27%) and 3 Gram-negative bacilli (27%), which were chosen for genetic identification by 16S rRNA gene sequencing (Table 1).
Six genera and 11 bacterial species were detected: Carnobacterium viridans; Staphylococcus epidermidis; Staphylococcus capitis subsp urealyticus; Bacillus gottheilii; Staphylococcus hominis subsp hominis; Niallia circulans; Bacillus safensis; Enterococcus quebecensis; Bacillus pumilus; Pseudomonas fluorescens; and Acinetobacter lwoffii (Table 1).
A total of 64% of the identified species are opportunistic human pathogens, namely S. epidermidis, S. capitis and S. hominis (coagulase-negative staphylococci (CoNS)), N. circulans, B. pumilus, P. fluorescens, and A. lwoffii (Table 1).
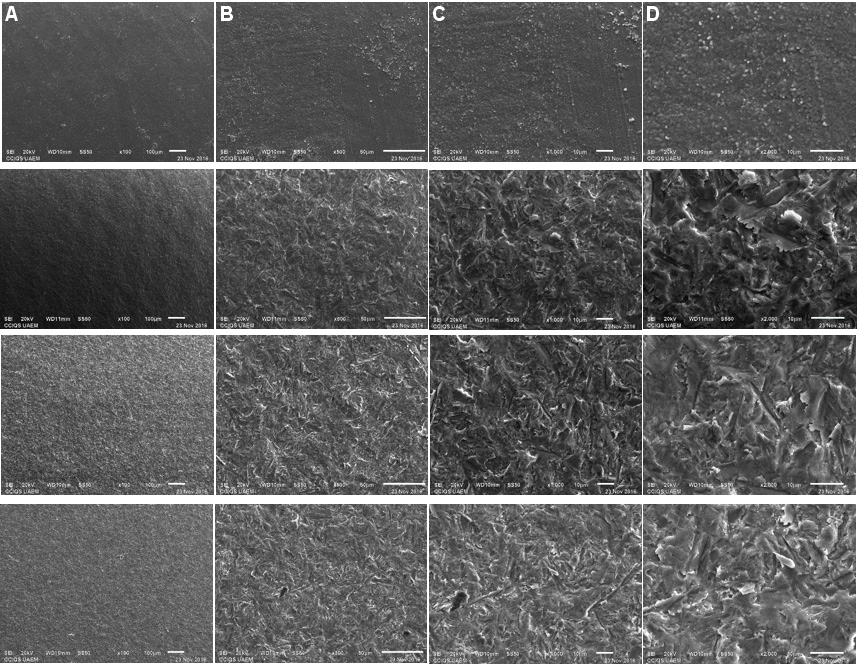
Regarding the characterization of the biofilm by SEM, a random sample of the 5 disinfected tubes that showed bacterial growth was analyzed (40%). In some disinfected samples, there was no evidence of biofilm formation (Figure 1A), while other disinfected samples showed biofilm formation (Figure 1B–D).
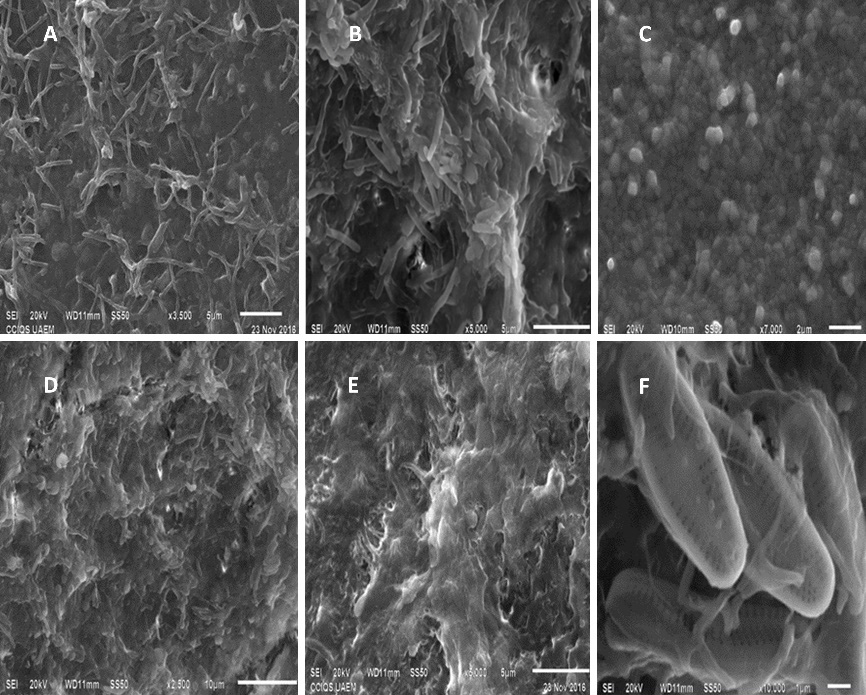
Three random samples were analyzed from the 10 non-disinfected tubes that showed bacterial growth (30%). The non-disinfected samples showed a thick polymeric matrix layer (Figure 2A,D,E). The detected biofilm comprised bacteria with coccoid and bacillary morphology (Figure 2B,C), and numerous diatoms (Figure 2F).
Discussion
The present quantitative study was conducted to evaluate contamination in triple-syringe tube sections of dental units. According to the study design, half of the tube sections were not disinfected, while the other half were previously disinfected with a 2% hypochlorite solution for 2 min. Despite prior disinfection, 5 dental units were found to be contaminated, as demonstrated by bacterial growth in the cultures and Gram staining, which was also confirmed by API (Analytical Profile Index) test galleries (data not shown). It was hypothesized that microorganisms would persist despite disinfection, since hypochlorite can reduce bacterial counts by preventing bacterial penetration into deeper layers by reacting with the surface organic matrix,7 but it does not eliminate bacteria adhering to the surface of the tubes in the form of biofilm. A better understanding of the ecology of biofilm in water lines is needed to control biofilm formation.
According to Hoogenkamp et al., in a system such as the water lines of dental units, it is necessary that first biofilm with bacteria of the vital liquid itself is established so that the colonization of bacteria of non-aqueous origin can subsequently occur.11 This study identified bacteria previously reported in the aquatic environment or as environmental contaminants that are not pathogenic for humans.
For example, E. quebecensis, unrelated to fecal contamination, was isolated from a water well in Canada.12 Since it is considered a species typical of the aquatic environment free of contamination, its presence in the evaluated water lines is probably “an unusual finding”. Moreover, we detected B. gottheilii, a species described in 2013, isolated from a pharmaceutical manufacturing site, the environmental implications of which have not yet been elucidated.13 Therefore, we report its presence in dental unit water lines. Also, B. safensis was identified; it is widespread in almost the entire aquatic and terrestrial environment.14 The bacillus N. circulans, an extraordinary exopolysaccharide producer,9 probably promoted biofilm growth in the studied water lines. A related species, B. pumilus, was also present in the dental unit water lines, and consequently, we could consider these bacilli as “normal” environmental contaminants in the odontological ecosystem. However, this does not imply that these species are not pathogenic for humans. The specific case of B. pumilus has been associated with septic arthritis, food intoxication, food-borne gastroenteritis, septicemia, peritonitis, and ophthalmitis.15, 16
As mentioned, once biofilm typical of the aquatic environment is established, it begins to colonize with bacteria of other origin. We detected bacteria from human skin and mucous membranes, such as S. epidermidis,17 S. capitis and S. hominis.18, 19, 20, 21 All these species are CoNS, considered opportunistic bacteria composed of genes encoding adhesive factors and biofilm production factors, hemolysins, and exoenzymes.18, 19
Coagulase-negative staphylococci, in general, can affect inpatients and outpatients, those on dialysis,22 newborns,23 cancer patients,20 transplant or transfused patients,24 those with autoimmune diseases or diseases such as acquired immune deficiency syndrome (AIDS),25 and those with chronic diseases,26 particularly diabetes.21, 26 The sources of contamination have been identified as skin (of the axillae, perineum and groin), membranes (of the nasal and respiratory tract)27 and oral cavity (in both healthy and non-healthy children); CoNS are also present in patients with malignant diseases.28 The bacteria have also been detected in human clinical specimens, purulent material, milk, and, less frequently, in blood.29
Niallia circulans, formerly called Bacillus circulans,30 is mainly considered an opportunistic pathogen in immunocompromised patients.31 However, many non-immunocompromised infections have been described, such as endophthalmitis,32 mixed abscess,31 peritonitis,33 wound infection,34 meningitis, and endocarditis.35 Specific studies on the presence of this bacterium in dental settings and its correlation with non-immunocompromised infections are needed.
In the case of P. fluorescens, this bacterium is not generally considered a human pathogen.36 It is widely studied for its role in the soil and the rhizosphere, but with the use of culture-independent methods, it has been found to possess several functional characteristics that enable it to inhabit mammalian hosts.36 It has been described as causing bacteremia in humans,37 and reports have identified it in respiratory samples.38 It is important to monitor the presence of this bacterium, which tends to be environmental, but can easily colonize humans, with the consequences still unknown.
Within the group of bacteria detected as human pathogens, A. lwoffii was also found. This species is a Gram-negative aerobic bacillus that is part of the microbiota of the skin, oropharynx and perineum in about 20–25% of healthy people.39 However, it is currently reported as an emerging pathogen associated with gastritis40 and infections in neonatal intensive care units (ICUs).41 Studies such as ours, in which emerging pathogens are reflected, aid in recognizing that dental units could be reservoirs of these microorganisms and, at some point, contaminate the dental work environment. Moreover, access to dental units with retrosuction valves or antibacterial materials is almost impossible in many countries, including Mexico. It is necessary to resort to low-cost resources to curb the possibility of cross-infection in the dental area.
Environmental factors, including soil, contaminated food, sewage, and animal feces, also contribute to contamination.42 The sources of contamination in dental offices include microorganisms from the normal human skin flora of the dentist and the office staff, aerosols from patients, contamination from surfaces the operator is in contact with while caring for the patient, and biofilm from dental unit drive systems, the formation of which is favored by warm temperatures and periods of unit inactivity.2 The water tanks of dental units supplied with distilled water have been identified as harboring various pathogenic and opportunistic microorganisms. In our study, we only observed the following, probably due to the type of sample used: S. epidermidis; P. fluorescens; and Staphylococcus saprophyticus.43
Specifically, S. epidermidis is a typical member of the human epithelial microbiota and one of the most frequent nosocomial pathogens. It can adhere to surfaces and form biofilm that protects it from antibiotics and host defenses; it can also detect the presence of antimicrobial peptides and respond with important defense mechanisms.44, 45, 46 While this species does not usually cause harm to humans, it can behave as a pathogen in immunosuppressed patients. According to Heilman et al., S. epidermidis from the CoNS group causes chronic foreign body-related infections, increasing human morbidity and mortality, and potentially posing a problem when caring for non-immunocompetent patients in dental offices.19
Studies evaluating the contamination of dental unit piping systems have reported the presence of human pathogenic microorganisms.2 The contamination degree and the identified bacterial genera depend on sociodemographic characteristics and the analyzed sample.3, 47, 48
In the present study, the microscopic characterization of the biofilm was carried out to analyze the morphology of the bacteria, the thickness of the biofilm, as well as changes in the implantation mechanisms in the previously disinfected tubes. Biofilm formation was found to be scarce, likely because little time elapsed between disinfection and measurement.
The detected biofilm showed a dense matrix with morphologically distinct bacteria, suggesting the presence of a complex structure that probably represented a remnant of mature biofilm that was not adequately removed by the chosen disinfection method.11, 49 This important finding points to a problem to be solved; it confirms that it is challenging to eradicate the biofilm formed in the aquatic environment, as it can resist antimicrobial treatment.
An unexpected finding was the presence of diatoms. They were identified through morphological analysis as Nupela vitiosa, described by Potapova.50 Diatoms are recognized as one of the biological components of lotic systems most suitable for monitoring water quality in terms of organic contamination. Their presence in most of the evaluated dental units suggests the possibility of the contamination of the water used in the unit dispensers, coming from the Faculty of Dentistry cistern.50
Limitations
With regard to the study limitations, we can report that the number of CFU per milliliter (CFU/mL) was not quantified, which would have helped establish whether the minimum cleanliness conditions of the water entering and leaving the dental units were met. We suggest implementing this analysis in future research. Furthermore, it is necessary to evaluate representative sections along the entire length of the pipeline and the water tanks of dental units. Our inability to detect biofilm by SEM in some units while finding it in others may be due to the fixation medium, although glutaraldehyde has previously been shown to be an effective fixative. Methacarn and Carnoy’s solution have also been suggested as fixatives that can preserve biofilm architecture more effectively.50 Notably, we only considered the analysis of the biofilm collected using the swabbing method. However, we propose the use of sonication as a complementary method to recover a more significant number of bacterial species for future studies. It is important to review the data on the municipal water used in dental units and the aerosol output of dental instruments, and correlate it with oral microorganisms in patients. Finally, we propose further studies analyzing the mechanisms of bacterial resistance the reported species may have, which would help elucidate their involvement in human disease.
Conclusions
The bacteria detected in the water lines of the dental units included in this study are considered opportunistic microorganisms from the normal microbiota of the skin and mucous membranes, and the environment. Dental unit water lines are critical elements, as there are many procedures and devices in which they are used – cooling, cleaning, sterilizing, or rinsing. This water must be in the best possible condition. Studies such as this allow new questions to be raised about particular microorganisms that might be present in the dental environment. Data on this topic should be updated until total biosafety is achieved in the numerous protocols in which water is involved in dental procedures.
Ethics approval and consent to participate
The study protocol was authorized by the Institutional Review Board at the Center for Advanced Studies and Research in Dentistry, School of Dentistry, Autonomous University of the State of Mexico, Toluca, Mexico (CEICIEAO-2019-007).
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.