Abstract
Background. Curved root canals are associated with the highest number of procedural errors during endodontic instrumentation. Recently, numerous rotary instruments have been developed, with both manual and automated mechanisms, to facilitate endodontic treatment and manage the complications related to it.
Objectives. The aim of the study was to assess post-endodontic pain after using the HyFlex® EDM OneFile (HEDM), WaveOne® Gold (WOG) and XP-endo® Shaper (XPS) systems in the preparation of curved canals in patients with asymptomatic irreversible pulpitis.
Material and methods. A total of 45 molars with curved canals and asymptomatic irreversible pulpitis were randomly divided into 3 equal groups based on the instrumentation used: HEDM (group A); WOG (group B); and XPS (group C). All teeth were prepared according to the manufacturers’ instructions. Post-endodontic pain was assessed using the visual analog scale (VAS) at 6, 12, 18, 24, 48, and 72 h after root canal instrumentation. The data was analyzed using the one-way analysis of variance (ANOVA) and the paired-samples t test with the Bonferroni correction, with a p-value of 0.05 set for statistical significance.
Results. The highest levels of post-endodontic pain were recorded at 6 h after treatment. Then, the values gradually decreased until the pain nearly vanished after 72 h. No statistically significant differences were observed in the VAS scores between groups A and B. At the same time, group C showed the lowest VAS scores at all follow-up time points.
Conclusions. The use of the XPS system resulted in the lowest pain scores at all follow-ups. The HEDM and WOG groups showed no differences in the pain scores throughout the whole follow-up period.
Keywords: visual analog scale, curved canals, post-endodontic pain, automated preparation
Introduction
Post-endodontic pain is an unpleasant outcome for both patients and clinicians. The degree of post-endodontic pain ranges from 25% to 40% worldwide. The incidence and intensity of post-endodontic pain are related to microbial factors, iatrogenic factors, like chemical and mechanical injuries to the periapical tissues during instrumentation, and patient-related factors, such as age, gender, pulp vitality, and the pathologies affecting the periapical tissues.1, 2
The goal of patient management is to relieve pain, maintain function and preserve esthetics. However, orofacial pain may occur during any step of treatment. The pain induced by interventions can interfere with orofacial pain, which is multifactorial and characterized by a wide spectrum of signs and symptoms.2
It is uncommon to find a tooth with both a straight root and a straight root canal, as most teeth exhibit some degree of canal curvature, even if the root is straight.3 Curved root canals are associated with the highest number of procedural errors during endodontic instrumentation, including perforations, blocked canals, ledges, and apical transportation. Treating a tooth with a curved canal remains a challenge, and requires suitable instruments and techniques.4 Apical debris extrusion is believed to induce acute inflammatory reactions and is considered a direct cause of post-endodontic pain.5, 6
Nowadays, numerous rotary instruments have been developed with advanced metallurgy and mechanisms to facilitate endodontic treatment. Nonetheless, all preparation instruments and techniques are still associated with some degree of debris extrusion, which may cause post-endodontic pain.7
Most nickel–titanium (NiTi) rotary and reciprocating instrument systems extrude less debris than stainless steel hand K-files, potentially reducing the risk of post-endodontic pain.8
The new HyFlex® EDM OneFile (HEDM) instrument (Coltène/Whaledent AG, Altstätten, Switzerland) is manufactured with the use of electrical discharge techniques. As a result, the file has a uniquely hardened surface, which is extremely flexible and highly resistant to fracture.9, 10
On the other hand, the WaveOne® Gold (WOG) system, launched in 2015 by Dentsply Sirona (Ballaigues, Switzerland), is manufactured using a new gold heat treatment. The file is made of a traditional NiTi alloy that first undergoes the grinding process and is then heat-treated to obtain a gold color. The heating process, combined with the latest reciprocating technology, enhances the flexibility of the file and its resistance to cyclic fatigue.11, 12 Also, WOG has a unique design that improves efficiency and fracture resistance. Due to its triangular, convex cross-section and 2 cutting edges, there are only 1 or 2 contact points between the cutting edges and the canal wall.13
A study performed by Alnassar et al. concluded that the manual instrumentation of root canals in primary molars might cause more pain as compared to automated preparation systems.14 In other words, the use of automated preparation systems in the root canal treatment of primary molars could reduce post-endodontic pain.14
The XP-endo® Shaper (XPS) (FKG Dentaire, La Chaux-de-Fonds, Switzerland) is manufactured using a NiTi MaxWire alloy. It has size 30 and a 0.01 taper. The XPS reaches the martensitic phase at 20°C and transforms to the austenitic phase at 37°C when placed in the canal. The file tip (Booster Tip) has 6 cutting edges, which enables the gradual shaping of the canal from size 15 to size 30 while keeping the instrument centered to prevent the straightening of the root canal. Due to its design, XPS shows good efficiency and fracture resistance.15, 16
Numerous studies have compared the effects of different reciprocating and rotary systems on post-endodontic pain, yielding varying results. Therefore, more research is necessary to determine the impact of different endodontic instruments on post-endodontic pain. The aim of the present study was to assess post-endodontic pain after using the HEDM, WOG and XPS systems in the preparation of curved canals in patients with asymptomatic irreversible pulpitis.
Material and methods
This randomized clinical study was conducted over a period of 2 years (2019–2020) at the Department of Endodontics, Faculty of Dentistry, Damascus University, Syria. The authors followed a pre-set protocol for the HEDM, WOG and XPS instrument systems. The study received ethical approval from the scientific committee at the Faculty of Dentistry of Damascus University (FMD\rct-758).
Sample selection
The study sample consisted of 45 molars with curved canals (20–45°), according to Schneider,17 and asymptomatic irreversible pulpitis.
Inclusion criteria
A clinical examination was performed to ensure the presence of acute, pulsating and continuous pain. Molars with acute pulpitis identified during previous examinations and curved canals (20–45°) were included.
Exclusion criteria
The exclusion criteria were molars with symptomatic/necrotic pulp, apical periodontitis, root resorption, and open apices, as well as patients with signs of systemic infection or uncontrolled systemic disease, and those using analgesics or non-steroidal or steroidal anti-inflammatory drugs.
Randomization
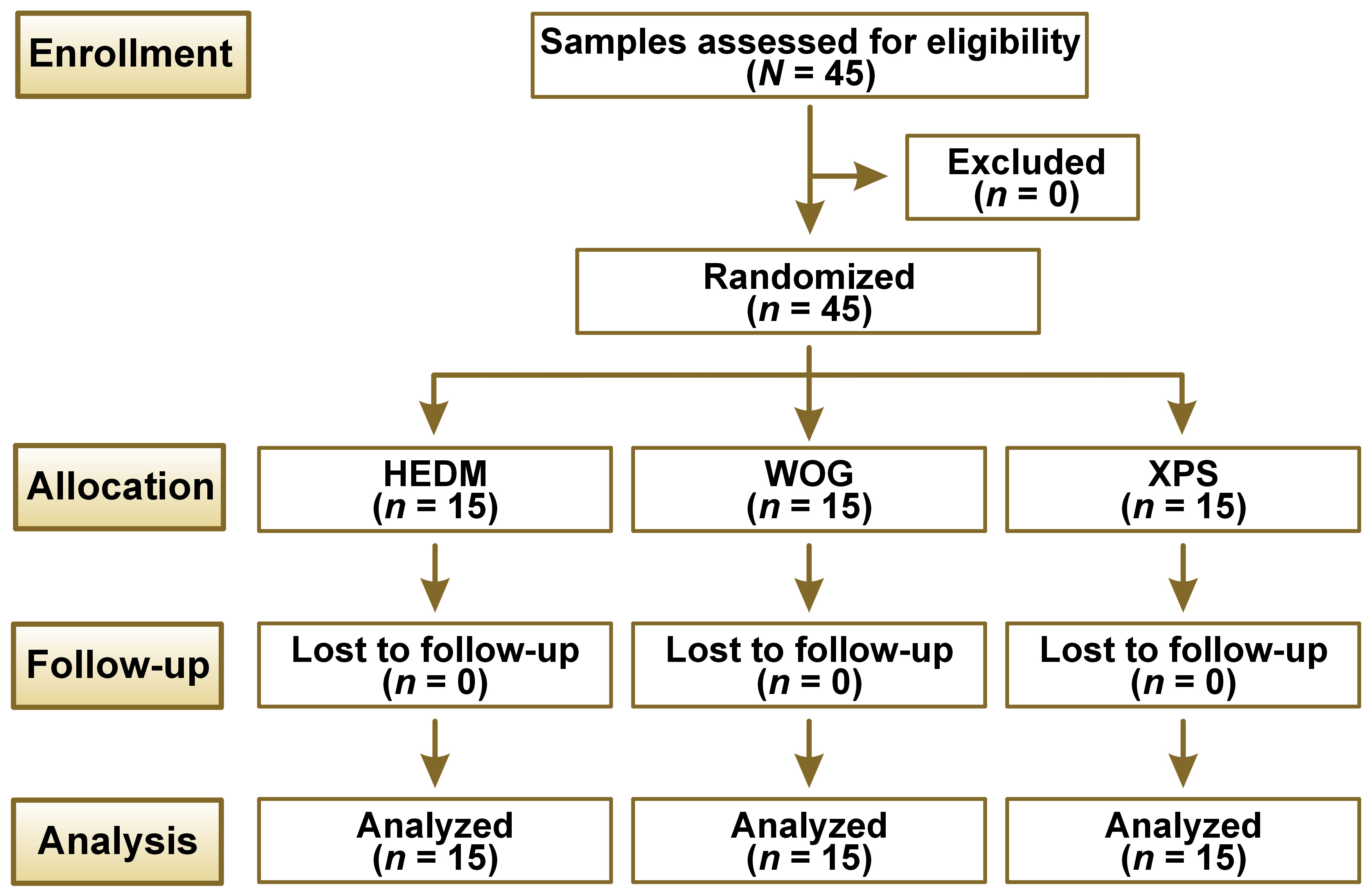
The study followed the Consolidated Standards of Reporting Trials (CONSORT) statement (Figure 1).18 Prior to treatment, the patient selected a card from a dark box containing 45 cards (15 red cards for HEDM, 15 yellow cards for WOG and 15 blue cards for XPS).
Then, the 45 molars were divided into 3 equal groups based on the instrumentation used: HEDM (group A); WOG (group B); and XPS (group C).
Treatment procedure
First, local anesthesia was performed using lidocaine 2% with epinephrine (1:100,000). Then, the access cavity was prepared using a round bur with a high-speed handpiece. A glide path was established with an ISO K-file up to size 15 after the working length was determined to be 1 mm from the apical foramen. All teeth were prepared according to the manufacturers’ instructions.
Group A: HEDM OneFile (25/~; Coltène/Whaledent AG) was used in a rotary motion (500 rpm, 2.5 N·cm). It was introduced into the canal with 3 in-and-out movements with a stroke amplitude of 3 mm until the full working length was reached.
Group B: WOG Primary File (25/.07; Dentsply Sirona) was used in the reciprocating mode after adjusting the working length. The file was introduced into the canal with an in-and-out picking motion (3 pecks with a stroke amplitude of 3 mm) while applying slight apical pressure until the full working length was obtained.
Group C: XPS single file (30/.01–.04; FKG Dentaire) was used in a continuous rotary movement at a speed of 1,000 rpm and a torque of N·cm. The file was inserted into the canal with an in-and-out motion, applying 5 strokes until the file reached its full working length.
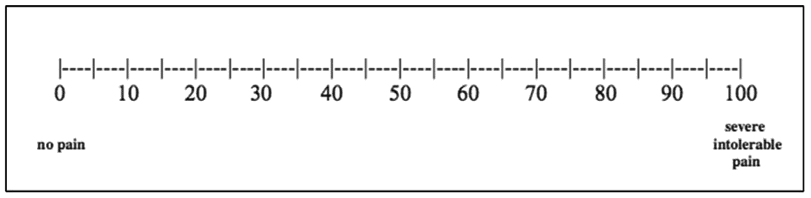
Post-endodontic pain was assessed using the visual analog scale (VAS) at 6, 12, 18, 24, 48, and 72 h after root canal instrumentation. For pain evaluation, the patients were asked to rate their pain level on VAS as follows: 0–24 – no pain; 25–49 – slight pain; 50–74 – moderate pain; and 75–100 – severe pain (Figure 2).19 They were reminded to register the pain values at different time points. If the pain was unbearable, the patients were allowed to take anti-inflammatory drugs after registering their pain level.
After 72 h, canal obturation was performed and the teeth were restored with composite.
Statistical analysis
Statistical analysis was performed using the IBM SPSS Statistics for Windows software, v. 22.0 (IBM Corp., Armonk, USA).
The data was analyzed using the one-way analysis of variance (ANOVA) and the paired-samples t test with the Bonferroni correction, with a p-value of 0.05 set for statistical significance.
Results
The study sample consisted of 45 molars in patients aged 19–55 years, divided into 3 equal groups. The descriptive analysis of all groups in terms of VAS pain scores is shown in Table 1.
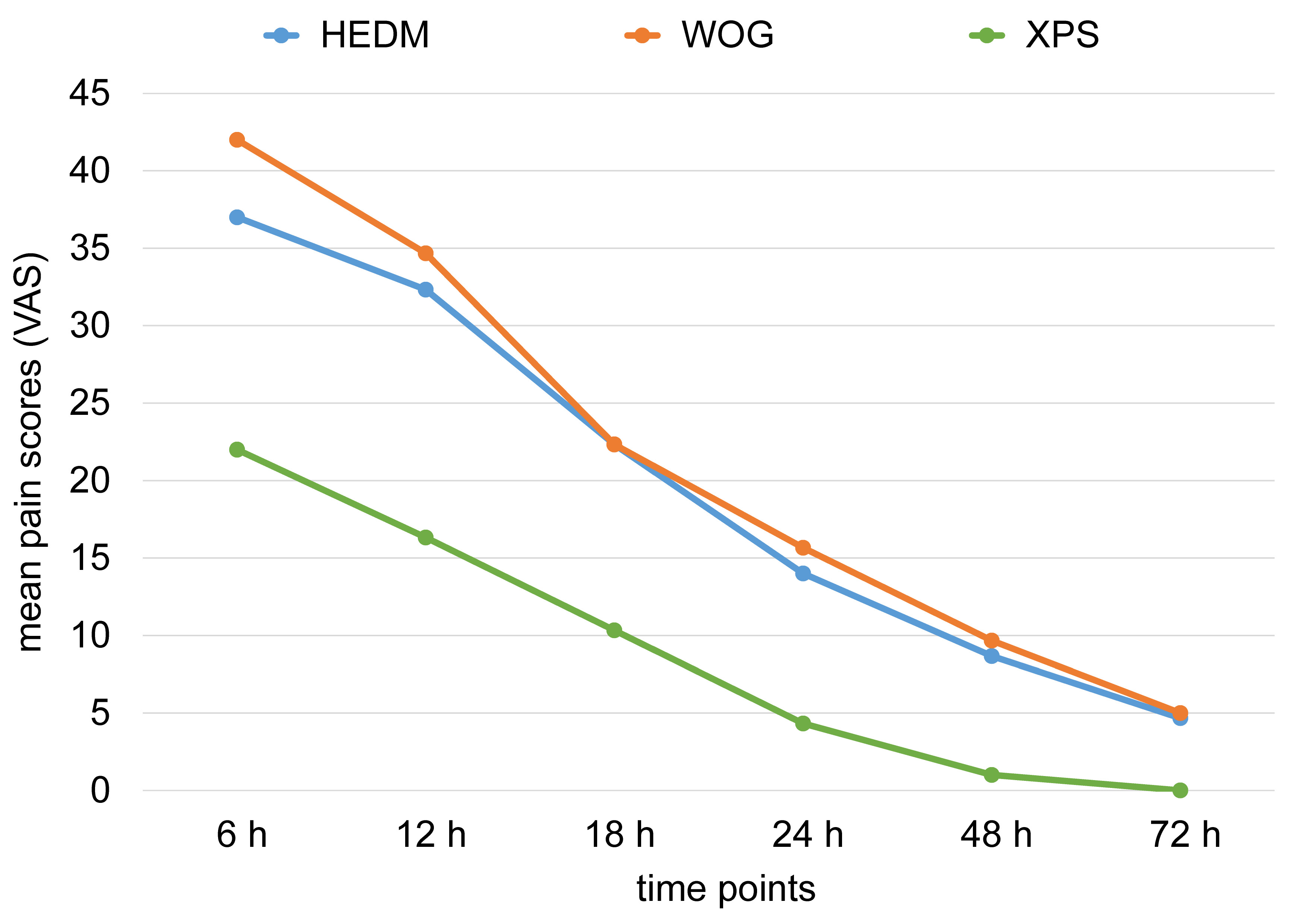
The results of the study indicate that the highest VAS pain values were observed at 6 h after canal instrumentation. Then, the values gradually decreased until the pain nearly vanished after 72 h.
The mean pain values after 6 h for HEDM, WOG and XPS were 37.00, 42.33 and 22.00, respectively. Then, the values gradually decreased over the specified periods until they reached 0 in the XPS group after 72 h (Figure 3). The XPS group exhibited the lowest mean VAS scores at all follow-up time points.
The one-way ANOVA was applied to detect intergroup differences in the VAS pain scores. At 6, 12, 18, 24, 48, and 72 h after root canal instrumentation, the p-values were lower than 0.05, indicating significant differences between the groups (Table 2).
The Bonferroni test was used to determine pairwise differences between the study groups. There were significant differences between group C (XPS) and groups A and B at all studied time points (p < 0.05). However, at a 95% confidence level, there were no significant differences in the VAS pain scores between groups A and B at any of the studied time points (p > 0.05) (Table 3).
Discussion
Post-endodontic pain is a serious complication following root canal treatment.20 The prevalence of post-endodontic pain ranges from 1.5% to 50%.21, 22
Only asymptomatic teeth were included in this study to minimize bias and isolate pre-endodontic pain as a variable factor that might affect post-endodontic pain, as previously reported.23
Besides, our study only included molars with curved canals (20–45°) due to a wide range of challenging cases; the preparation and shaping of curved canals may result in many post-treatment complications, such as pain and perforation.24, 25
Following pain assessment, all teeth were instrumented, and then obturated to control for the potential effect of obturation materials.26
Pain is difficult to assess and the evaluation of pain is considered subjective. Therefore, it is necessary to ensure that patients have a clear and full understanding of the questionnaires. In this study, VAS was chosen due to its ease of use, reliability and widespread application in previous pain assessment studies.27, 28
The results of our study show that the mean pain values were the highest at 6 h after endodontic treatment and gradually decreased over 72 h. This may be due to the irritation of the periapical area caused by the extrusion of instrumentation debris, leading to local inflammatory reactions and subsequent pain. The pain typically subsides after the healing of the periapical area at 72 h.5
This study found statistically significant differences in post-endodontic pain between the tested instrumentation techniques at 6, 12, 18, 24, 48, and 72 h. The XPS group had the lowest VAS pain values and the lowest amount of extruded debris, with the result being similar to that reported by Uslu et al.29
There were no statistically significant differences between the HEDM and WOG techniques. Similarly, Fontana et al.6 and Yeter et al.30 found that HEDM and WOG were comparable in terms of the amount of extruded debris.
These results are contrary to a study by Xavier et al., where the incidence of postoperative pain was higher in the XPS group than in the WOG group.28 It could be due to their study sample, which included premolars and molars, regardless of whether the canal was curved or straight.28
Contrary to the present study, Kherlakian et al. found no difference between the rotary and reciprocal systems.19 The researchers used different systems with varying tapers and sizes, and performed endodontic treatment during just one visit.19
Limitations
This study used the VAS score, which is a subjective method. In further research, we advise to extend the educational phase with regard to the patients included in the study. The other limitation is the type of rotary file used and the amount of excruded debris; slight differences might affect the results.
Conclusions
All systems used in the study caused pain, with the highest levels observed at 6 h after treatment. The pain gradually decreased until it almost disappeared at 72 h in all studied groups. The XPS group had the lowest pain values, whereas the HEDM and WOG groups showed no differences in pain values at all follow-up time points. In the XPS group, the pain reached its peak (22.00) at 6 h and gradually decreased to 0 after 72 h.
Trial registration
Trial registration number: 1119/2019.
Ethics approval and consent to participate
The study received ethical approval from the scientific committee at the Faculty of Dentistry of Damascus University, Syria (FMD\rct-758).
Data availability
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
Consent for publication
Not applicable.